Fill Out Your Ldss 3370 Form
The LDSS 3370 form plays a crucial role in ensuring the safety of children and families in various care settings across New York State. This form, officially known as the Statewide Central Register Database Check Form, is primarily utilized by agencies engaged in child care, adoption, foster care, and other related fields. Proper completion of this form is essential, as it allows the Statewide Central Register (SCR) to conduct background checks on individuals who may pose a risk to children. The form asks for detailed agency information, including a three-digit agency code and the agency liaison’s contact details, along with comprehensive applicant and household member data. It's imperative to include not only the applicant but also any adult household members, ensuring that all names are accurately recorded along with their relationships. Information about residency over the past 28 years must be meticulously documented, covering complete addresses without any gaps. The importance of legibility cannot be overstated, as any inaccuracies can result in delays or returned applications. Various signatures are required depending on the category of the application, emphasizing the need for everyone involved to provide their formal acknowledgment. Moreover, attention to detail extends to the payment of any applicable fees for certain categories, ensuring compliance with state laws. With the right information and careful attention to the instructions provided, the LDSS 3370 form serves as a vital tool for safeguarding children in care systems throughout the state.
Ldss 3370 Example
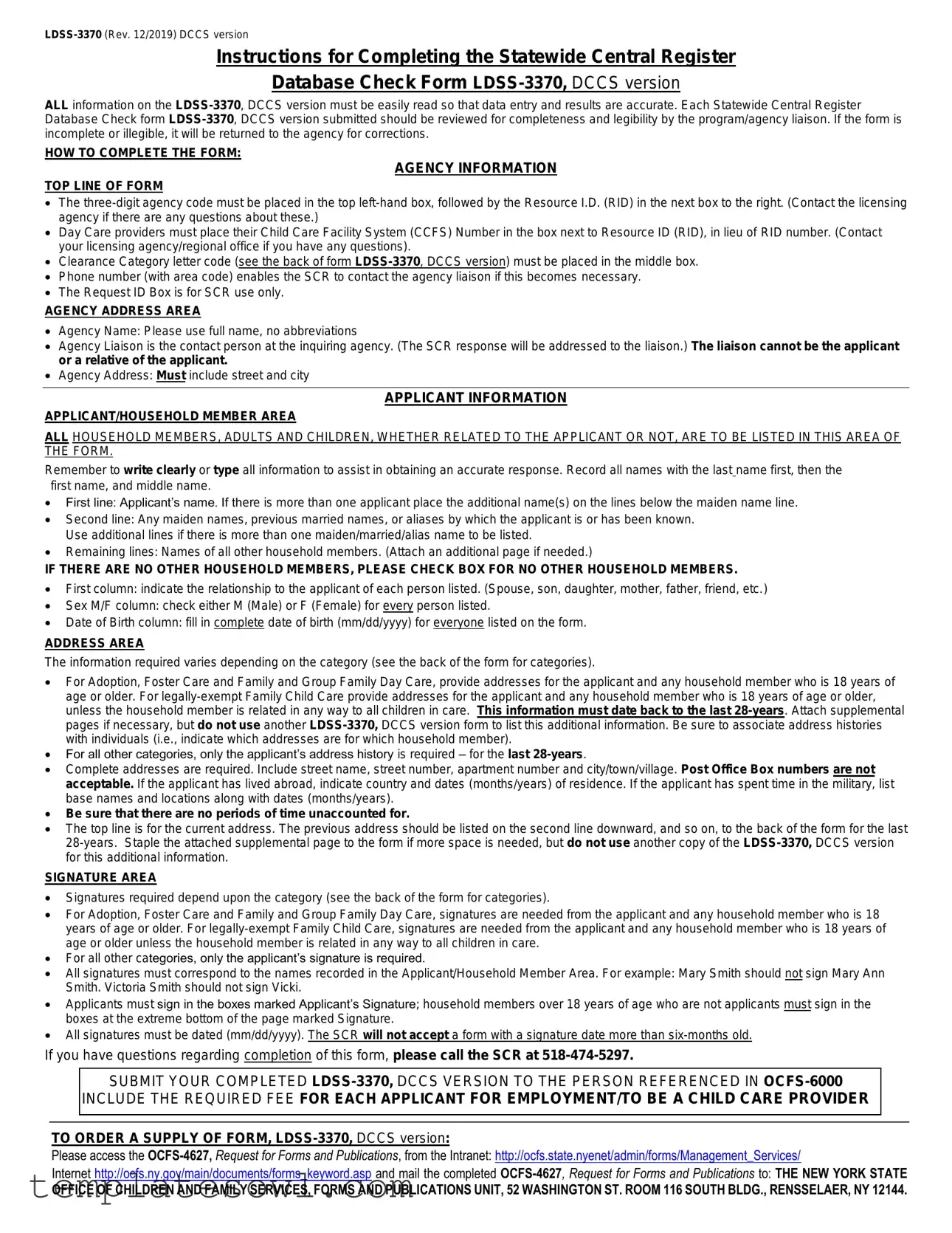
Instructions for Completing the Statewide Central Register
Database Check Form
ALL information on the
HOW TO COMPLETE THE FORM:
AGENCY INFORMATION
TOP LINE OF FORM
•The
•Day Care providers must place their Child Care Facility System (CCFS) Number in the box next to Resource ID (RID), in lieu of RID number. (Contact your licensing agency/regional office if you have any questions).
•Clearance Category letter code (see the back of form
•Phone number (with area code) enables the SCR to contact the agency liaison if this becomes necessary.
•The Request ID Box is for SCR use only.
AGENCY ADDRESS AREA
•Agency Name: Please use full name, no abbreviations
•Agency Liaison is the contact person at the inquiring agency. (The SCR response will be addressed to the liaison.) The liaison cannot be the applicant or a relative of the applicant.
•Agency Address: Must include street and city
APPLICANT INFORMATION
APPLICANT/HOUSEHOLD MEMBER AREA
ALL HOUSEHOLD MEMBERS, ADULTS AND CHILDREN, WHETHER RELATED TO THE APPLICANT OR NOT, ARE TO BE LISTED IN THIS AREA OF THE FORM.
Remember to write clearly or type all information to assist in obtaining an accurate response. Record all names with the last name first, then the first name, and middle name.
•First line: Applicant’s name. If there is more than one applicant place the additional name(s) on the lines below the maiden name line.
•Second line: Any maiden names, previous married names, or aliases by which the applicant is or has been known. Use additional lines if there is more than one maiden/married/alias name to be listed.
•Remaining lines: Names of all other household members. (Attach an additional page if needed.)
IF THERE ARE NO OTHER HOUSEHOLD MEMBERS, PLEASE CHECK BOX FOR NO OTHER HOUSEHOLD MEMBERS.
•First column: indicate the relationship to the applicant of each person listed. (Spouse, son, daughter, mother, father, friend, etc.)
•Sex M/F column: check either M (Male) or F (Female) for every person listed.
•Date of Birth column: fill in complete date of birth (mm/dd/yyyy) for everyone listed on the form.
ADDRESS AREA
The information required varies depending on the category (see the back of the form for categories).
•For Adoption, Foster Care and Family and Group Family Day Care, provide addresses for the applicant and any household member who is 18 years of age or older. For
•For all other categories, only the applicant’s address history is required – for the last
•Complete addresses are required. Include street name, street number, apartment number and city/town/village. Post Office Box numbers are not acceptable. If the applicant has lived abroad, indicate country and dates (months/years) of residence. If the applicant has spent time in the military, list base names and locations along with dates (months/years).
•Be sure that there are no periods of time unaccounted for.
•The top line is for the current address. The previous address should be listed on the second line downward, and so on, to the back of the form for the last
SIGNATURE AREA
•Signatures required depend upon the category (see the back of the form for categories).
•For Adoption, Foster Care and Family and Group Family Day Care, signatures are needed from the applicant and any household member who is 18 years of age or older. For
•For all other categories, only the applicant’s signature is required.
•All signatures must correspond to the names recorded in the Applicant/Household Member Area. For example: Mary Smith should not sign Mary Ann Smith. Victoria Smith should not sign Vicki.
•Applicants must sign in the boxes marked Applicant’s Signature; household members over 18 years of age who are not applicants must sign in the boxes at the extreme bottom of the page marked Signature.
•All signatures must be dated (mm/dd/yyyy). The SCR will not accept a form with a signature date more than
If you have questions regarding completion of this form, please call the SCR at
SUBMIT YOUR COMPLETED
INCLUDE THE REQUIRED FEE FOR EACH APPLICANT FOR EMPLOYMENT/TO BE A CHILD CARE PROVIDER
TO ORDER A SUPPLY OF FORM,
Please access the
Internet http://ocfs.ny.gov/main/documents/forms_keyword.asp and mail the completed
OFFICE OF CHILDREN AND FAMILY SERVICES, FORMS AND PUBLICATIONS UNIT, 52 WASHINGTON ST. ROOM 116 SOUTH BLDG., RENSSELAER, NY 12144.
NEW YORK STATE
OFFICE OF CHILDREN AND FAMILY SERVICES
STATEWIDE CENTRAL REGISTER DATABASE CHECK
Agency Use Only
SCR USE ONLY
REQUEST I.D.:
ALL INFORMATION MUST BE COMPLETE. PLEASE PRINT OR TYPE
AGENCY CODE: |
RESOURCE I.D. (RID) |
CHILD CARE FACILITY SYSTEM (CCFS) NUMBER: |
CATEGORY (Use alpha codes on reverse): |
PHONE NUMBER (Area Code): |
||||
|
|
|
|
|
|
|
( ) |
- |
|
|
|
|
|
|
|
|
|
PRINT BELOW THE ADDRESS ASSOCIATED WITH YOUR RID/CCFS NUMBER: |
The particular classifications of persons who must or may be screened |
|||||||
AGENCY |
|
|
|
|
are set forth on the reverse side of this document. The alpha codes to |
|||
|
|
|
|
complete the “Category” box above, are also on the reverse side of this |
||||
NAME: |
|
|
|
|
||||
|
|
|
|
form. |
|
|||
|
|
|
|
|
|
|
||
AGENCY |
|
|
|
|
|
|||
|
|
|
|
FOR ALL CATEGORIES: Complete the following for yourself, your |
||||
LIAISON: |
|
|
|
|
||||
|
|
|
|
spouse, your children and any other person(s) in your home at the |
||||
|
|
|
|
|
|
|||
STREET |
|
|
|
|
present time. MAKE SURE YOU COMPLETE ALL MAIDEN |
|||
ADDRESS: |
|
|
|
|
NAME/ALIAS/MARRIAGE SECTIONS THAT APPLY. IF NONE, |
|||
|
|
|
|
|
|
STATE “NONE” List RELATIONSHIP in the fields below. |
||
CITY: |
|
STATE: |
ZIP CODE: |
|||||
|
(see reverse side for instructions) Attach additional page if necessary. |
|||||||
|
|
|
|
|
|
|||
The purpose of collecting the demographic data on other persons in your household who are not screened pursuant to Section
APPLICANT/HOUSEHOLD MEMBER AREA |
PLEASE TYPE OR PRINT CLEARLY |
|
|
|
|||
IF THERE ARE NO OTHER HOUSEHOLD MEMBERS, PLEASE CHECK THIS BOX. |
|
|
|
|
|
||
|
|
|
|
|
|
|
|
RELATIONSHIP TO |
LAST NAME |
|
FIRST NAME |
SEX |
DATE OF BIRTH |
||
APPLICANT |
|
M/F |
mm |
dd |
yyyy |
||
|
|
|
|||||
APPLICANT |
|
|
|
M |
|
|
|
|
|
|
F |
|
|
|
|
APPLICANT MAIDEN/ALIAS/ |
|
|
|
M |
|
|
|
MARRIED NAME |
|
|
|
F |
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
|
F |
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
|
F |
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
|
F |
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
|
F |
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
|
F |
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
|
F |
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
|
F |
|
|
|
Please provide your current address and any other addresses at which you have resided for the last
CURRENT STREET ADDRESS |
APT # |
CITY |
STATE |
ZIP |
FROM (Mo/Yr) |
TO (Mo/Yr) |
|
|
|
|
|
/ |
/ |
|
|
|
|
|
|
|
PREVIOUS STREET ADDRESS |
APT # |
CITY |
STATE |
ZIP |
FROM (Mo/Yr) |
TO (Mo/Yr) |
|
|
|
|
|
/ |
/ |
|
|
|
|
|
|
|
PREVIOUS STREET ADDRESS |
APT # |
CITY |
STATE |
ZIP |
FROM (Mo/Yr) |
TO (Mo/Yr) |
|
|
|
|
|
/ |
/ |
|
|
|
|
|
|
|
PREVIOUS STREET ADDRESS |
APT # |
CITY |
STATE |
ZIP |
FROM (Mo/Yr) |
TO (Mo/Yr) |
|
|
|
|
|
/ |
/ |
|
|
|
|
|
|
|
PREVIOUS STREET ADDRESS |
APT # |
CITY |
STATE |
ZIP |
FROM (Mo/Yr) |
TO (Mo/Yr) |
|
|
|
|
|
/ |
/ |
|
|
|
|
|
|
|
I affirm that all the information provided on this form is true to the best of my knowledge. I understand that if I knowingly give false statements, such action could be grounds for denial or dismissal from employment or denial or revocation of a license, certificate, permit, registration or approval.
APPLICANT’S SIGNATURE |
DATE (mm/dd/yyyy) |
|
|
/ |
/ |
APPLICANT’S SIGNATURE
DATE (mm/dd/yyyy)
/ /
I understand that as a person 18 years of age or older in a home of an applicant to become an Adoptive or a Foster Parent or a Family or Group Family Day Care provider or a
SIGNATURE
DATE (mm/dd/yyyy)
/ /
SIGNATURE
DATE (mm/dd/yyyy)
/ /
AGENCY LIAISON INSTRUCTIONS
Please verify that each form is completed. Incomplete forms will be returned to the sender. For ADOPTION, FOSTER CARE, and FAMILY and GROUP FAMILY DAY CARE, if both spouses are applicants, both are to sign. Persons 18 years of age or older residing in the home of applicants for ADOPTION, FOSTER CARE and FAMILY AND GROUP FAMILY DAY CARE also must sign the form.
AGENCY CODE: Record your
DAYCARE PROVIDERS: Must place their Child Care Facility System (CCFS) Number in the box next to Resource ID (RID), in lieu of RID number. (Contact your licensing agency/regional office if you have any questions).
RESOURCE I.D. (RID): Record your RID in this field. OCFS, OMH, OMRDD, DOH, OASAS and SED licensed agencies and programs and local departments of social services, have RIDs as of 9/2001. Verify your RID with your licensing agency. If you need assistance, email: ocfs.sm.conn_app@ocfs.ny.gov
CLEARANCE CATEGORIES: Record the appropriate alpha code in the category box.
care. (This category is only to be used by Enrollment Agencies). |
||
|
||
(fee required - see below) * |
||
|
||
traveling day camp. |
||
|
||
reimbursement) ** |
submitted by authorized licensing agency only.) |
|
|
(fee required - see below) * |
|
(fee required - see below) * |
below) * Provide address history for all household members 18- |
|
years old or over. |
||
|
||
care who does not reside in the home. No checks required |
||
when provider is a |
||
(fee required - see below) * Provide address history for all |
||
care provider. |
||
household members 18 years old or over. |
||
|
||
(This category is only to be used by Enrollment Agencies) (fee |
||
required - see below) * |
||
|
||
|
||
required when provider is a |
|
|
child care provider. (This category is only to be used by |
||
Enrollment Agencies) (fee required - see below) * For providers, |
pending before the inquiring agency. |
|
include address history for all household members |
||
or over who are not related in any way to all children in care. |
||
|
||
|
(fee required - see below) * |
|
Prospective employee of |
||
|
||
|
||
|
|
AGENCY LIAISON: Record the name of the person to whom the response should be sent (cannot be the same as applicant or related to the applicant).
APPLICANT/HOUSEHOLD MEMBER AREA INSTRUCTIONS: This information is to be provided by the applicant/employee/ provider. (See front of form).
APPLICANT(S):
MAIDEN NAME/ALTERNATIVE/AKA: MUST be completed for every applicant. Record ALL previous names used. Start with second line. Use as many lines as needed (one last name per line)
OTHER HOUSEHOLD MEMBERS: describe relationship to applicant, e.g., son, daughter, father, mother, friend, etc. on remaining lines
(ATTACH ADDITIONAL PAGE IF NECESSARY)
IF THERE ARE NO OTHER HOUSEHOLD MEMBERS, PLEASE CHECK BOX FOR NO OTHER HOUSEHOLD MEMBERS.
*Social Services Law
N.B.: a separate check must accompany each form.
**Social Services Law
If you have questions, please call the SCR at
SUBMIT YOUR COMPLETED FORM,

STAPLE TO
STATEWIDE CENTRAL REGISTER DATABASE CHECK FORM
ADDITIONAL PAGE
(Use only if the space on the form,
APPLICANT NAME:
Print clearly, all dates must be consecutive (month/year). Be sure to associate address histories with particular individuals.
|
PREVIOUS STREET ADDRESS |
|
|
CITY |
|
|
STATE |
|
|
ZIP |
|
|
FROM |
|
|
TO |
|
|
|
|
|
|
|
|
|
|
(Mo/Yr) |
|
|
(Mo/Yr) |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
/ |
|
/ |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
/ |
|
/ |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
/ |
|
/ |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
/ |
|
/ |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
/ |
|
/ |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
/ |
|
/ |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
/ |
|
/ |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
/ |
|
/ |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
/ |
|
/ |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
/ |
|
/ |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
/ |
|
/ |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
/ |
|
/ |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
/ |
|
/ |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
/ |
|
/ |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
/ |
|
/ |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
/ |
|
/ |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
/ |
|
/ |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
/ |
|
/ |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
/ |
|
/ |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
/ |
|
/ |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
/ |
|
/ |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
/ |
|
/ |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
/ |
|
/ |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
/ |
|
/ |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
/ |
|
/ |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
STAPLE TO
STATEWIDE CENTRAL REGISTER DATABASE CHECK FORM
ADDITIONAL PAGE
(Use only if the space on the form,
APPLICANT NAME:
Other Household Members are: (please print clearly):

 IF THERE ARE NO OTHER HOUSEHOLD MEMBERS, PLEASE CHECK THIS BOX.
IF THERE ARE NO OTHER HOUSEHOLD MEMBERS, PLEASE CHECK THIS BOX.
SCR USE |
RELATIONSHIP |
LAST NAME |
FIRST NAME |
SEX |
DATE OF BIRTH |
||
ONLY |
TO APPLICANT |
|
|
M/F |
mm |
dd |
yyyy |
|
|
|
|
M |
|
|
|
|
|
|
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
|
F |
|
|
|
|
|
|
|
|
|
|
|
Form Characteristics
| Fact Name | Details |
|---|---|
| Form Title | LDSS-3370 is titled "Instructions for Completing the Statewide Central Register Database Check Form." |
| Governing Law | The form is governed by New York State Social Services Law Section 424-a. |
| Submission Requirements | All information on the form must be complete and legible; otherwise, the form will be returned for corrections. |
| Agency Information | Submitter must include a three-digit agency code and the Child Care Facility System (CCFS) number, if applicable. |
| Applicant Information | All household members, regardless of relation to the applicant, must be listed on the form. |
| Signature Requirements | Dependent on the category, signatures may be required from applicants and household members aged 18 or older. |
| Mailing Instructions | The completed form should be mailed to the Statewide Central Register at P.O. Box 4480, Albany, NY 12204-0480. |
Guidelines on Utilizing Ldss 3370
Completing the LDSS-3370 form requires attention to detail to ensure that all information is accurately captured. Following these instructions will help facilitate the process and avoid delays.
- Begin by filling in the **Agency Information** at the top left corner of the form:
- Enter the three-digit agency code.
- Next, in the box to the right, input the Resource I.D. (RID).
- If you are a daycare provider, input your Child Care Facility System (CCFS) Number in the adjacent box.
- In the middle box, add the Clearance Category letter code.
- Then, provide a phone number (including area code) for the agency liaison.
- Leave the Request ID Box blank, as it is for SCR use only.
- Provide the **Agency Address**:
- List the full Agency Name without abbreviations.
- Identify the Agency Liaison, who should not be the applicant or a relative.
- Include the full Agency Address with street, city, state, and zip code.
- Complete the **Applicant and Household Member Area**:
- List all household members, regardless of relationship, in order with the last name first.
- Start with the Applicant's name. Use separate lines for any additional applicants.
- On the next line, indicate any maiden names, previous married names, or aliases.
- For remaining lines, list other household members. If none, write "NONE" below the Maiden/Alias section.
- Indicate the relationship to the applicant for each person listed.
- Fill in M (Male) or F (Female) for each listed person in the sex column.
- Provide the complete date of birth (mm/dd/yy) for each individual.
- Address information varies by category:
- For Adoption, Foster Care, and Family/Group Family Day Care, list addresses for all adults in the home for the past 28 years.
- For other categories, only the applicant's address history is required for the last 28 years.
- Ensure that complete addresses (street name, city, state, and zip code) are provided.
- List current address on the top line, followed by previous addresses downwards.
- In the **Signature Area**:
- For Adoption, Foster Care, and Family/Group Family Day Care categories, both applicants and any household members over 18 must sign.
- Others only need the applicant's signature. Ensure the signature matches the name provided.
- Date all signatures in mm/dd/yy format. Avoid signatures dated more than six months prior.
- Finally, ensure the form is complete:
- Review for clarity and completeness.
- Mail the completed form to:
P.O. Box 4480, Albany, N.Y. 12204-0480.
After submission, the Statewide Central Register will process the information provided. If any issues arise, the agency liaison may be contacted for clarification. It is crucial to keep a copy of the completed form for your records.
What You Should Know About This Form
What is the purpose of the LDSS-3370 form?
The LDSS-3370 form is used to conduct background checks through the Statewide Central Register. It helps ensure that individuals involved in adoption, foster care, and other child care settings do not have a history of child abuse or maltreatment. The information collected is essential for maintaining the safety and welfare of children in these environments.
Who needs to fill out the LDSS-3370 form?
The form must be completed by the applicant and any household members who are 18 years or older. This includes anyone living with the applicant, regardless of their relationship to the applicant. This information is vital for thorough background checks.
What information is required on the form?
Detailed information is needed, such as names, dates of birth, and addresses for the last 28 years for both the applicant and other adult household members. This helps create a comprehensive profile for the background check. All names should be recorded with the last name first, followed by the first and middle names.
What happens if the form is incomplete or illegible?
If the LDSS-3370 form is not filled out correctly, it will be returned to the agency for corrections. Accurate and legible information is crucial to avoid delays in the background check process. It is recommended that someone review the form before submission to ensure all fields are complete.
How should I submit the LDSS-3370 form?
The completed form should be mailed to the Statewide Central Register at P.O. Box 4480, Albany, NY 12204-0480. Make sure to send it to the attention of the Service Center Unit. Double-check that the form is filled out completely to avoid returns.
Are there any fees associated with submitting the LDSS-3370 form?
Yes, certain categories require a fee of $25. This fee needs to be submitted alongside the completed form in the form of a certified check or money order made out to the "New York State Office of Children and Family Services." Each submission requires its own payment.
What if I have questions while filling out the form?
If you have questions about completing the LDSS-3370 form, you can call the Statewide Central Register at 518-474-5297. They can provide guidance and clarification on any concerns you may have during the process.
Common mistakes
When completing the LDSS-3370 form, people often make mistakes that can lead to delays or rejections. One common error is failing to provide legible information. Since the form requires clarity for accurate data entry, any illegible handwriting can result in the form being returned for corrections. Ensuring that all information is written clearly, either by printing or typing, is crucial.
Another mistake frequently observed is incorrect or incomplete agency details. The agency code and Resource I.D. (RID) must be accurately filled out in the designated areas. Daycare providers need to ensure that their Child Care Facility System (CCFS) number is placed correctly. If this information is faulty or missing, the processing of the form may be delayed.
Individuals also tend to overlook the requirement to list all household members accurately. All adults and children living in the household must be included, regardless of their relationship to the applicant. Failure to include everyone can create gaps in the information, potentially leading to additional inquiries or complications during the database check.
In addition to listing all household members, mistakes are often made when recording their information. People sometimes forget to provide complete names, including maiden names or aliases. This oversight complicates the process of matching records in the statewide central register and could result in inaccuracies in the database check.
Lastly, not paying attention to the signature requirements can cause issues. Each signature must match the name as recorded on the form. Any discrepancies, such as using a nickname instead of a full name, may invalidate the submission. Additionally, all signatures need to be current and dated appropriately. If a signature is more than six months old, the form will be rejected, requiring resubmission.
Documents used along the form
The LDSS-3370 form is essential for individuals and agencies seeking to check the Statewide Central Register Database regarding child abuse or maltreatment allegations. However, to complete the process smoothly, several other documents often accompany the LDSS-3370 form. Understanding these documents can facilitate the application process and ensure compliance with state requirements.
- OCFS-4627 Request for Forms and Publications: This form is used to order supplies of the LDSS-3370 and other related forms from the Office of Children and Family Services (OCFS). Agencies can submit this request through specified channels to maintain necessary paperwork.
- Supplemental Information Sheet: This sheet may be attached to the LDSS-3370 if additional space is needed for addresses or household members. It allows applicants to provide necessary information without cluttering the original form.
- Agency Code Verification Letter: Agencies are often required to include their unique three-digit code on the LDSS-3370. This letter serves as confirmation that the agency's code has been validated with the appropriate licensing authority, ensuring proper processing.
- Proof of Identity Documents: In some cases, applicants may need to submit IDs such as driver’s licenses or social security cards. This documentation helps verify identities and is particularly relevant for background checks.
- Clearance Category Letter: Depending on the nature of the application, a letter indicating the appropriate clearance category may be required. This letter helps classify the level of scrutiny needed for individuals applying as foster care or daycare providers.
- Signature Verification Form: When additional household members over the age of 18 are involved, a signature verification form may be utilized. This ensures that all necessary adults consent to the background check and confirms their identity in relation to the applicant.
Having these accompanying documents ready not only streamlines the submission process but also minimizes potential delays while awaiting background checks. Therefore, it’s advisable to gather them ahead of time, ensuring a smoother experience for everyone involved in the child welfare system. Understanding these requirements can make a significant difference in fulfilling your obligations when working with the LDSS-3370 form.
Similar forms
The LDSS-3370 form is an important document used primarily for background checks on individuals involved with child care services. There are various other documents that serve similar purposes in screening or verifying information. Below is a list of eight such documents, outlining how they are similar to the LDSS-3370 form.
- Fingerprint Card: Like the LDSS-3370, fingerprint cards are used to conduct background checks. They require detailed personal information, ensuring that criminal histories can be thoroughly searched and accurately matched to individuals.
- Child Care License Application: This application requires information about the applicant, including their background, similar to the details needed in the LDSS-3370. Both forms assess suitability for child care roles.
- Criminal Background Check Form: This form collects personal details and previous addresses, just as the LDSS-3370 does. It focuses on ensuring that individuals do not have a history that would make them unsuitable for child-related positions.
- Foster Parent Application: The information sought in the foster parent application resembles that in the LDSS-3370. Both documents involve comprehensive background checks, including household member details and living history.
- Child Adoption Application: The adoption application mirrors the LDSS-3370 by requiring a full disclosure of household members and their histories. It serves the same purpose of ensuring the safety and well-being of children.
- Medical Clearance Form: This form is used to verify the health status of individuals in child care roles. Much like the LDSS-3370, it ensures that all relevant information about the applicant and household members is considered.
- Employee Background Disclosure: Required by many child care agencies, this disclosure demands personal history similar to that in the LDSS-3370. It aims to protect children by vetting those who will work closely with them.
- Home Study Report: Conducted for prospective adoptive or foster parents, the home study report evaluates individual and family histories, paralleling the thoroughness of the LDSS-3370 in assessing suitability for child care roles.
Each of these documents emphasizes the importance of gathering comprehensive and accurate information to ensure the safety and welfare of children. Completing them accurately and thoroughly is crucial in fulfilling the intended purpose of safeguarding minors.
Dos and Don'ts
Do's:
- Ensure all information is clearly printed or typed.
- Include the complete names of all household members.
- List the agency information accurately at the top of the form.
- Provide comprehensive addresses for all relevant individuals over the past 28 years.
- Sign in the designated areas and ensure dates are current (not older than 6 months).
- Include the three-digit agency code where required.
- Contact the licensing agency with any questions regarding the details needed.
Don'ts:
- Do not use abbreviations when naming the agency.
- Avoid omitting any household members or their details.
- Do not sign the form with names that do not match the recorded names.
- Do not leave any field blank; incomplete forms will be returned.
- Do not use periods of time that go unaccounted for on address histories.
- Avoid using Post Office Box numbers; complete street addresses are required.
- Do not submit multiple LDSS-3370 forms for additional address information; use a separate page instead.
Misconceptions
- Misconception: The LDSS-3370 form is only for applicants. The form needs to include all household members, whether they are related to the applicant or not. This is to ensure a thorough background check.
- Misconception: Incomplete forms will still be processed. If the form is incomplete or illegible, it will be returned for corrections. Making sure all sections are filled out properly is essential for timely processing.
- Misconception: Only the applicant’s current address is required. Depending on the category, the applicant's address history for the last 28 years must be submitted. For households with members over 18, their address histories are also necessary for certain categories.
- Misconception: The form can be signed by anyone in the household. Only the applicant and other household members who are 18 years or older need to sign, and their signatures must match the names provided on the form.
- Misconception: Post Office Box addresses are acceptable. Only complete street addresses are required. Post Office Box addresses cannot be used on the form.
- Misconception: There is no time limit on signature dates. All signatures must be dated and cannot be more than six months old at the time of submission. Ensure the signatures are timely to avoid processing delays.
- Misconception: Daycare providers do not need to provide a specific number. Daycare providers must include their Child Care Facility System (CCFS) Number in the appropriate area of the form instead of a Resource ID number.
Key takeaways
When filling out the LDSS-3370 form, it is crucial to ensure accuracy and clarity. Here are ten key takeaways:
- Complete Legibility: All information on the form must be easily read to prevent errors in data entry and results.
- Agency Information: Provide the three-digit agency code and Resource I.D. (RID), along with the Child Care Facility System (CCFS) Number for daycare providers.
- Clearance Category: Enter the appropriate Clearance Category letter code to indicate the purpose of the request.
- Contact Information: Include the phone number of the agency liaison for potential follow-up by the SCR.
- Applicant Details: List all household members, both adults and children, whether or not they are related, including their full names, relationship, sex, and date of birth.
- Address History: Provide a detailed address history for the applicant and household members over 18 for the past 28 years when applicable.
- No Abbreviations: Use full names and addresses without abbreviations to avoid confusion during processing.
- Signature Requirements: Depending on the category, ensure that necessary signatures are obtained, especially from household members over 18 in specific situations.
- No Acceptance of Post Office Boxes: All addresses must include street names and numbers; Post Office Box numbers are not acceptable for this form.
- Mailing Instructions: After completion, mail the form to the designated address at the Statewide Central Register to ensure it is processed correctly.
Filling out the LDSS-3370 correctly aids in timely processing and contributes to better handling of child protection matters.
Browse Other Templates
Discharge Paperwork From Hospital - Signature of the person completing the form is required.
Herbalife Purchase Request,Herbalife Product Order Sheet,Herbalife Customer Order Form,Herbalife Supply Acquisition Form,Herbalife Transaction Form,Herbalife Product Order Invoice,Herbalife Distributor Order Document,Herbalife Orders & Transactions,H - Information privacy: Your details will remain confidential.
Khsaa Middle School Physical Form - Insurance carrier details must be provided for students participating in athletics.