Fill Out Your Lic 603 Form
The LIC 603 form is an essential tool used by residential care facilities in California to gather vital information regarding an applicant's health and social needs. Before admission, this comprehensive appraisal captures a variety of details ranging from the applicant’s overall health condition and any dietary limitations to their physical and mental capabilities. Significant aspects of the form include sections on health history, which require a record of current medications, major illnesses, and any recent hospitalizations. It also assesses the individual’s social interactions and personal preferences, which can be critical for their wellbeing in a community setting. The form inquires about ambulation status, detailing the applicant’s ability to navigate various environments and the potential need for assistance. Furthermore, it specifically seeks to identify required services to ensure that the individual receives appropriate care and support upon admission. This structured approach not only helps in placement decisions but also facilitates a smoother transition into the residential care facility.
Lic 603 Example
STATE OF CALIFORNIA - HEALTH AND HUMAN SERVICES AGENCY |
CALIFORNIA DEPARTMENT OF SOCIAL SERVICES |
|
COMMUNITY CARE LICENSING |
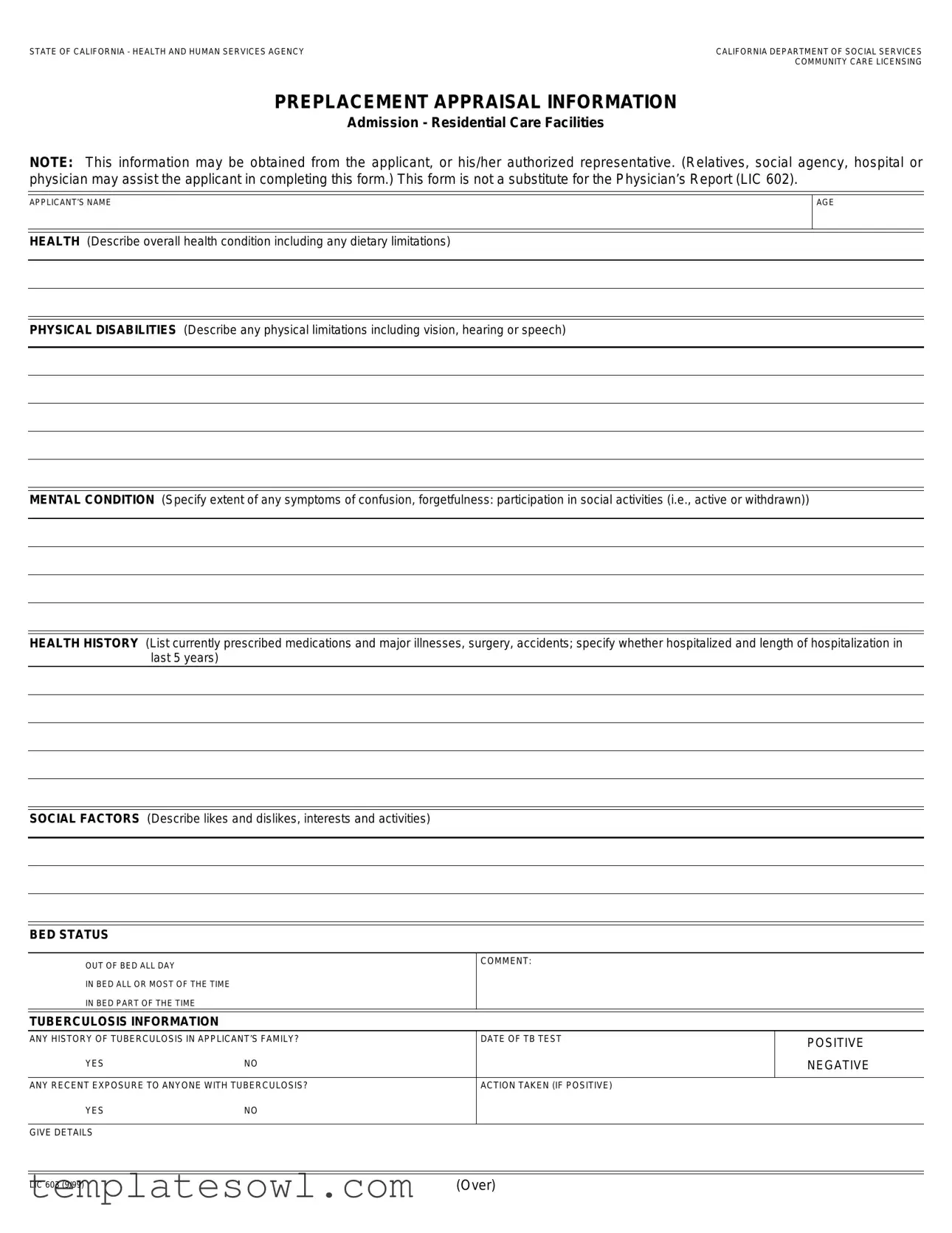
PREPLACEMENT APPRAISAL INFORMATION
Admission - Residential Care Facilities
NOTE: This information may be obtained from the applicant, or his/her authorized representative. (Relatives, social agency, hospital or physician may assist the applicant in completing this form.) This form is not a substitute for the Physician’s Report (LIC 602).
APPLICANT’S NAME
AGE
HEALTH (Describe overall health condition including any dietary limitations)
PHYSICAL DISABILITIES (Describe any physical limitations including vision, hearing or speech)
MENTAL CONDITION (Specify extent of any symptoms of confusion, forgetfulness: participation in social activities (i.e., active or withdrawn))
HEALTH HISTORY (List currently prescribed medications and major illnesses, surgery, accidents; specify whether hospitalized and length of hospitalization in last 5 years)
SOCIAL FACTORS (Describe likes and dislikes, interests and activities)
BED STATUS
■
■
■
OUT OF BED ALL DAY
IN BED ALL OR MOST OF THE TIME IN BED PART OF THE TIME
COMMENT:
TUBERCULOSIS INFORMATION
ANY HISTORY OF TUBERCULOSIS IN APPLICANT’S FAMILY? |
DATE OF TB TEST |
■ POSITIVE |
|
|
|
|
|
■ YES |
■ NO |
|
■ NEGATIVE |
|
|
|
|
ANY RECENT EXPOSURE TO ANYONE WITH TUBERCULOSIS? |
ACTION TAKEN (IF POSITIVE) |
|
|
■ YES |
■ NO |
|
|
|
|
|
|
GIVE DETAILS |
|
|
|
LIC 603 (9/99) |
(Over) |
AMBULATORY STATUS (this person is ■ ambulatory ■ nonambulatory)
Ambulatory means able to demonstrate the mental and physical ability to leave a building without the assistance of a person or the use of a mechanical device. An ambulatory person must be able to do the following:
YES NO
■■ Able to walk without any physical assistance (e.g., walker, crutches, other person), or able to walk with a cane.
■■ Mentally and physically able to follow signals and instructions for evacuation.
■■ Able to use evacuation routes including stairs if necessary.
■■ Able to evacuate reasonably quickly (e.g., walk directly the route without hesitation).
FUNCTIONAL CAPABILITIES (Check all items below)
YES |
NO |
|
|
|
■ |
■ |
Active, requires no personal help of any kind - able to go up and down stairs easily |
|
|
■ |
■ |
Active, but has difficulty climbing or descending stairs |
|
|
■ |
■ |
Uses brace or crutch |
|
|
■ |
■ |
Feeble or slow |
|
|
■ |
■ |
Uses walker. If Yes, can get in and out unassisted? |
■ Yes |
■ No |
■ |
■ |
Uses wheelchair. If Yes, can get in and out unassisted? |
■ Yes |
■ No |
■■ Requires grab bars in bathroom
■■ Other: (Describe)
_______________________________________________________________________________________________________________
SERVICES NEEDED (Check items and explain)
YES NO
■ ■
■ ■
■ ■
■ ■
■ ■
■ ■
■ ■
■ ■
■ ■
■ ■
■ ■
■ ■
■ ■
■ ■
■ ■
Help in transferring in and out of bed and dressing________________________________________________________________________
_______________________________________________________________________________________________________________
Help with bathing, hair care, personal hygiene ___________________________________________________________________________
Does client desire and is client capable of doing own personal laundry and other household tasks (specify) ___________________________
Help with moving about the facility ____________________________________________________________________________________
_______________________________________________________________________________________________________________
Help with eating (need for adaptive devices or assistance from another person) _________________________________________________
_______________________________________________________________________________________________________________
Special diet/observation of food intake _________________________________________________________________________________
_______________________________________________________________________________________________________________
Toileting, including assistance equipment, or assistance of another person_____________________________________________________
Continence, bowel or bladder control. Are assistive devices such as a catheter required? _________________________________________
Help with medication _______________________________________________________________________________________________
_______________________________________________________________________________________________________________
Needs special observation/night supervision (due to confusion, forgetfulness, wandering) _________________________________________
Help in managing own cash resources _________________________________________________________________________________
Help in participating in activity programs ________________________________________________________________________________
_______________________________________________________________________________________________________________
Special medical attention ___________________________________________________________________________________________
_______________________________________________________________________________________________________________
Assistance in incidental health and medical care _________________________________________________________________________
_______________________________________________________________________________________________________________
Other “Services Needed” not identified above ___________________________________________________________________________
_______________________________________________________________________________________________________________
Is there any additional information which would assist the facility in determining applicant’s suitability for admission? |
■ Yes |
■ No |
If Yes, please attach comments on separate sheet. |
|
|
To the best of my knowledge; I (the above person) do not need skilled nursing care.
SIGNATURE
DATE COMPLETED
APPLICANT (CLIENT) OR AUTHORIZED REPRESENTATIVE
SIGNATURE
DATE COMPLETED
LICENSEE OR DESIGNATED REPRESENTATIVE
DATE COMPLETED
Form Characteristics
| Fact Name | Description |
|---|---|
| Purpose | The LIC 603 form collects comprehensive health and personal information to assess an applicant's suitability for admission to a residential care facility in California. |
| Origin | This form is governed by California Health and Safety Code Section 1569.68, which provides regulations for community care licensing. |
| Who Completes It | The applicant or an authorized representative, such as a relative or social agency, is responsible for completing this form. |
| Not a Substitute | The LIC 603 is explicitly noted as not being a substitute for the Physician’s Report (LIC 602), which must also be provided. |
| Health Information Required | The form requires detailed descriptions of the applicant's health, physical disabilities, mental condition, and relevant health history, including current medications. |
| Ambulatory Status | It assesses whether the applicant is ambulatory or nonambulatory, which affects evacuation capability and safety in a residential facility. |
| Services Needed | Specific needs for assistance with daily activities, such as bathing, eating, and medication management, are identified to ensure appropriate care is provided. |
Guidelines on Utilizing Lic 603
Once the Lic 603 form has been filled out, it serves as a critical step in the process of evaluating an applicant's suitability for admission to a residential care facility. Completing this form accurately ensures that the facility can meet the applicant's specific needs and provide appropriate care.
- Begin by entering the applicant’s name at the top of the form.
- Next, provide the age of the applicant.
- Describe the applicant’s overall health condition, including any dietary limitations in the designated section.
- Detail the physical disabilities, if any, covering limitations related to vision, hearing, or speech.
- Specify the mental condition of the applicant, particularly any symptoms such as confusion or forgetfulness, as well as their participation in social activities.
- List the health history, including current medications, major illnesses, surgeries, or hospitalizations within the last five years.
- Describe the applicant's social factors, including likes, dislikes, interests, and activities.
- Select the appropriate bed status from the provided options: 'Out of bed all day', 'In bed all or most of the time', or 'In bed part of the time'.
- Provide information regarding any tuberculosis history in the applicant’s family and the date of the TB test.
- Indicate if there has been any recent exposure to someone with tuberculosis.
- Fill in the ambulatory status section, verifying if the applicant is ambulatory or non-ambulatory.
- In the functional capabilities section, check applicable boxes to indicate the applicant's abilities.
- Complete the services needed section, checking the relevant services and providing details where necessary.
- If applicable, indicate if there is any additional information that would assist the facility in assessing the applicant.
- Finally, ensure the form is signed and dated by the applicant or authorized representative and by the licensee or designated representative.
What You Should Know About This Form
What is the purpose of the Lic 603 form?
The Lic 603 form is designed to gather important information about individuals seeking admission to residential care facilities in California. It focuses on the applicant's health conditions, physical and mental capabilities, and any specific needs that must be addressed. This information helps facilities assess the suitability of the applicant for their services and ensure proper care is provided upon admission.
Who can assist with filling out the Lic 603 form?
The form can be completed by the applicant themselves or by an authorized representative. This representative may include family members, staff from social agencies, or healthcare professionals such as doctors or hospital personnel. Having someone help with this form can ensure all necessary information is accurately captured.
What types of health information are required on the Lic 603 form?
The form asks for various health-related details, including overall health condition, any dietary restrictions, and a history of major illnesses or surgeries. Specific information about current medications and any past hospitalizations in the last five years is also required. This ensures that the care facility can meet the medical needs of the applicant.
How does the Lic 603 form assess an applicant's physical capabilities?
Applicants are asked to disclose their ambulatory status, which determines if they can move independently within the facility. The form includes questions about mobility, the ability to follow evacuation procedures, and any necessary aids, such as wheelchairs or walkers. Understanding an individual's physical capabilities helps the facility prepare for emergencies and tailor their support services.
What social factors are considered in the Lic 603 form?
In addition to physical and health-related questions, the form requests information about the applicant's social preferences, including likes, dislikes, and interests. This information is valuable for helping staff engage the resident in activities and ensuring their overall well-being in the facility.
Can additional information be provided on the Lic 603 form?
Yes, if there is extra information that would assist the facility in determining the applicant's suitability, there is a section on the form for additional comments. This can include specifics about the applicant's needs or any other relevant details that may not be covered in the standard questions.
Is the Lic 603 form a substitute for a physician's report?
No, the Lic 603 form is not a substitute for a Physician’s Report (LIC 602). The two forms serve different purposes. While the Lic 603 gathers comprehensive appraisal information for the facility, the Physician’s Report focuses specifically on medical evaluations and recommendations from a healthcare provider. Both forms are important for ensuring proper care for residents.
Common mistakes
Filling out the Lic 603 form can be a straightforward process, but many people make mistakes that can cause delays or issues during admission. One common error is incomplete health information. It’s essential to provide a thorough description of the applicant's overall health, including any dietary restrictions. Omitting critical details can lead to complications in care and affect the applicant's suitability for the facility.
Another frequent mistake is misunderstanding the ambulation status. Applicants may incorrectly check the boxes regarding their ability to walk and evacuate in emergencies. It is vital to accurately assess and report on whether the individual is ambulatory or nonambulatory, as this information directly impacts their safety and the type of assistance they may need.
Additionally, many individuals fail to thoroughly detail physical disabilities and mental conditions. This section requires careful consideration. Describing any limitations in vision, hearing, or speech, along with mental health symptoms, helps the facility prepare adequately. Inadequate descriptions can lead to a mismatch between the care provided and the applicant's actual needs.
People also often forget to include complete health history. Listing medications, past surgeries, and any significant health events within the last five years is crucial. Facilities rely on this history to provide safe and effective care. Missing medication details or hospitalizations might leave caregivers unprepared for the applicant's specific needs.
Lastly, some applicants do not check the services needed section carefully. This area allows for specifying required assistance, which is vital for the staff to understand the support necessary for the individual. Failing to indicate all needed services can result in insufficient planning and inadequate care for the applicant once they arrive.
Documents used along the form
The LIC 603 form is essential for assessing an individual's suitability for admission to residential care facilities in California. To complete the admission process, several other forms and documents often accompany the LIC 603. These additional documents provide a fuller picture of the applicant's needs and medical history, ensuring that the facility can provide appropriate care.
- Physician's Report (LIC 602): This form details the applicant's medical history and current health status, including diagnoses, treatments, and any necessary medical recommendations. It serves as a crucial complement to the LIC 603 by offering professional insights into the applicant's health and medical requirements.
- Request for Transfer (LIC 625): Used when transferring a client from one facility to another, this form ensures continuity of care. It includes essential information about the resident's health, treatment plans, and any special needs that should be considered during the transfer process.
- Personal Rights (LIC 613): This form outlines the rights of residents within a care facility. It ensures that the applicant is aware of their rights regarding privacy, dignity, and personal choice, setting the tone for respectful and compassionate care.
- Admission Agreement: An important contract between the resident and the facility, this document details the terms of admission, services provided, fees charged, and the rights and responsibilities of both parties. It helps to clarify expectations and protect the interests of the applicant.
By utilizing these forms, care facilities can ensure they understand each applicant's unique needs, allowing for tailored care and support. Proper documentation is a critical step in fostering a safe and effective environment for residents.
Similar forms
- LIC 602 - Physician’s Report: This form provides a detailed medical evaluation and is required to assess an applicant’s overall health status. It complements the LIC 603 by providing a professional examination of the applicant's medical history and current health conditions.
- LIC 610 - Emergency Disaster Plan: This document outlines procedures for emergencies within the facility. While the LIC 603 focuses on the applicant's health and capabilities, the LIC 610 ensures the facility is prepared to handle any potential emergencies, including considerations for residents’ health needs.
- LIC 700 - Personnel Record: The personnel record contains information about staff qualifications and training. Like the LIC 603, it focuses on assessment but pertains to the caregivers rather than the residents, ensuring that they are equipped to meet the needs depicted in the LIC 603.
- LIC 500 - Application for License: This application initiates the process of seeking a license for a care facility. While the LIC 603 evaluates an individual applicant's needs, the LIC 500 represents the overall intention to provide care that meets those needs, forming a crucial part of the licensing process.
Dos and Don'ts
When filling out the Lic 603 form, here are five important things to do and avoid:
- Do ensure accurate information: Provide all necessary details truthfully, including health conditions and capabilities.
- Do ask for help if needed: If you’re unsure about any part of the form, consider seeking assistance from a family member or a professional.
- Do keep it clear and concise: Use straightforward language and avoid any unnecessary jargon to enhance understanding.
- Do include relevant medical history: Detail any previous illnesses, surgeries, or medications to provide a comprehensive health overview.
- Do review your answers: Before submitting, double-check for accuracy and completeness to prevent delays in processing.
- Don't omit crucial information: Leaving important questions unanswered can lead to complications later in the process.
- Don't rush through the form: Take your time to ensure each section is thoughtfully and completely filled out.
- Don't use abbreviations: Writing in full sentences helps avoid misunderstandings and confusion during the review.
- Don't hesitate to provide additional notes: If there are specific concerns or considerations, include them in a separate attachment.
- Don't forget to sign: Ensure that the appropriate signatures are present to validate your submission.
Misconceptions
When it comes to the Lic 603 form, many people may have misunderstandings about its purpose and function. Here are eight common misconceptions:
- The Lic 603 form is the same as the Physician’s Report (LIC 602). Many assume that the two forms serve identical purposes. However, the Lic 603 is specifically for preplacement appraisal and does not substitute for the Physician’s Report, which provides a detailed medical evaluation.
- The form can only be filled out by the applicant. This is incorrect. The form can also be completed by an authorized representative, such as a family member, social agency, or healthcare provider, which can help ensure all necessary information is accurately collected.
- Phealth history and medication lists are not required. Some individuals believe that providing health history and current medications is optional. In reality, detailed information about medications and medical history is key to determining appropriate care for the applicant.
- The form only addresses physical health. A common misunderstanding is that the Lic 603 focuses solely on physical ailments. The form also inquires about mental health, social factors, and functional capabilities, recognizing the importance of holistic assessment.
- Filling out the form is a simple task. Many people think the form is straightforward and quick to fill out. However, it requires comprehensive details across several categories, which may take time and careful consideration.
- Ambulatory status only refers to whether the person can walk. While this is partially true, the ambulatory status section also assesses the individual's ability to follow evacuation instructions and navigate safely, which are crucial for safety in residential care settings.
- Services needed are only about physical assistance. Some might think that the services needed section only considers physical help. In fact, the form encompasses a wide range of needs, including emotional support and participation in activities, highlighting the importance of overall well-being.
- Once submitted, the information is unchangeable. Many believe that after submitting the form, no changes can be made. In reality, the form allows for ongoing updates, especially if additional information or circumstances arise that might influence care decisions.
Understanding these misconceptions can help individuals complete the Lic 603 form more effectively and ensure that the applicant receives the most appropriate care tailored to their needs.
Key takeaways
When filling out the Lic 603 form, it is essential to gather comprehensive information about the applicant to assist with their admission into a residential care facility.
- The form must be completed with the assistance of the applicant or their authorized representative.
- Detailed descriptions of the applicant’s overall health condition and any dietary limitations are required.
- It is important to specify any physical and mental disabilities accurately.
- Listing current medications, major illnesses, surgeries, and hospitalizations within the last five years is necessary.
- Understanding the applicant’s social factors, including interests and activities, can help tailor care services.
- The bed status section clarifies the applicant's typical daily routine regarding bed use.
- Inquiries about any history of tuberculosis, including family history and exposure, should be honestly answered.
- Ambulatory status affects the care plan; provide clear indications of the applicant's mobility and evacuation capabilities.
- Functional capabilities relating to personal care and mobility need to be checked to ensure the appropriate services are offered.
- Identifying services needed, such as help with bathing or medication management, assists in creating a customized care strategy.
- Any additional information that could aid in assessing the applicant's suitability for admission should be documented.
Signature and dates are required from both the applicant (or authorized representative) and the facility’s licensee to validate the information provided.
Browse Other Templates
Why Did Angie's List Change Its Name - Help us achieve excellence through your comments.
Alabama Court Forms - The CS-22 form contains specific timelines for when payments must be made.