Fill Out Your M11Q Form
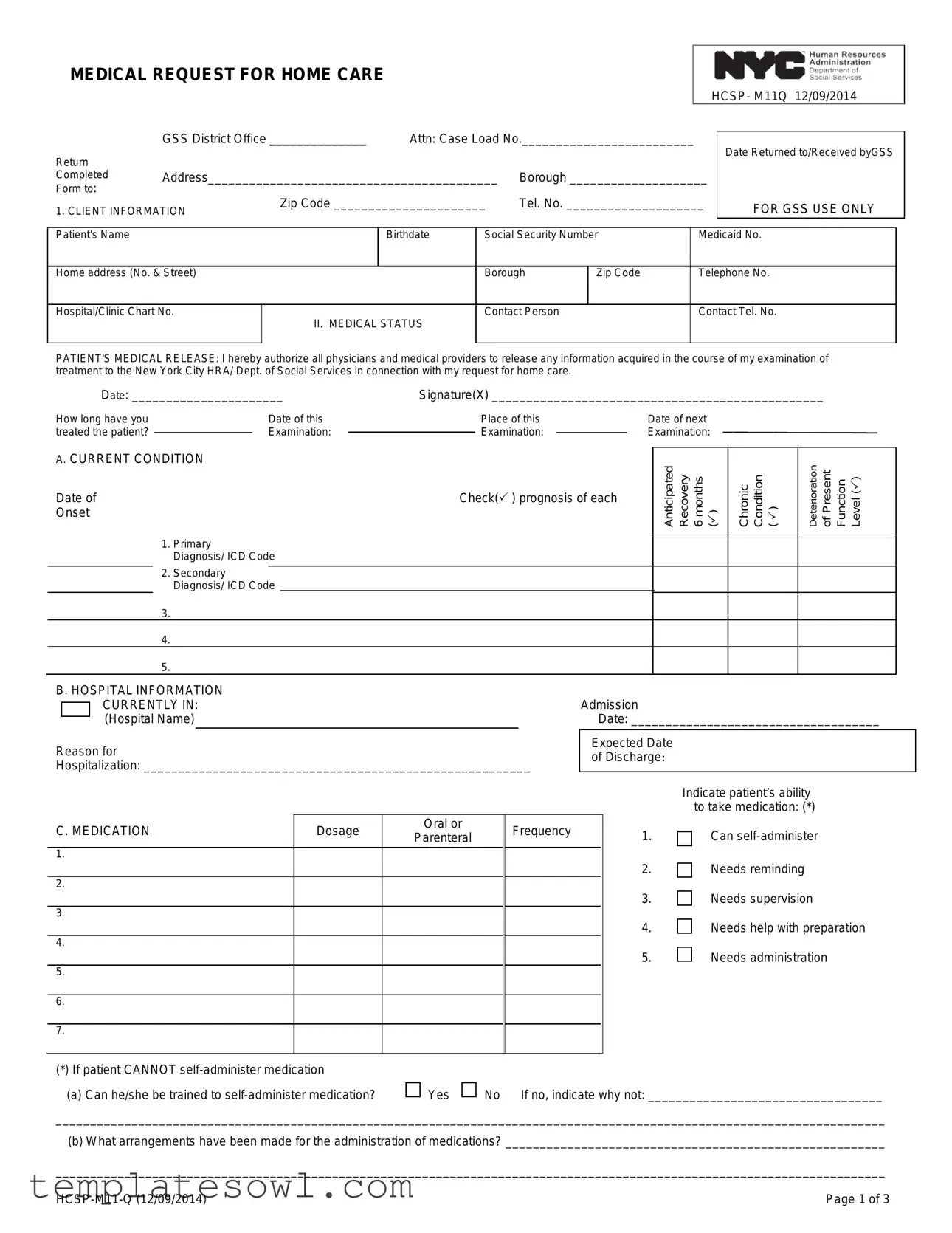
The M11Q form serves as a critical component for individuals seeking home care services through the New York City Human Resources Administration (HRA). This form, formally titled "Medical Request for Home Care," meticulously collects essential client information, including personal identifiers and medical statuses. It requires input from medical professionals who must authorize the release of necessary medical information while providing a comprehensive overview of the patient’s health conditions and treatment needs. The form emphasizes the importance of accurately documenting primary and secondary diagnoses, the patient's ability to self-administer medications, and any specialized medical treatments currently required. In addition, the M11Q prompts medical professionals to assess whether a patient can direct a home care worker and outlines any assistive equipment needed for daily living. To facilitate approval, the form mandates a physician's certification, ensuring that it aligns with state regulations and accurately reflects the patient's condition and needs. It also includes a section for additional comments, allowing for a nuanced perspective on the patient’s overall circumstances that may impact their home care requirements. As a result, the M11Q plays a pivotal role in streamlining the process of obtaining necessary home care services while safeguarding the health and well-being of patients.
M11Q Example
MEDICAL REQUEST FOR HOME CARE |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
HCSP- M11Q 12/09/2014 |
||
|
GSS District Office ______________ |
Attn: Case Load No._________________________ |
|
|
|
|
||||||
Return |
|
|
Date Returned to/Received byGSS |
|||||||||
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
Completed |
Address__________________________________________ |
Borough ____________________ |
|
|
|
|||||||
Form to: |
|
Zip Code ______________________ |
Tel. No. ____________________ |
|
|
|
||||||
1. CLIENT INFORMATION |
|
FOR GSS USE ONLY |
||||||||||
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|||
Patient’s Name |
|
|
|
Birthdate |
Social Security Number |
|
Medicaid No. |
|||||
|
|
|
|
|
|
|
|
|
||||
Home address (No. & Street) |
|
|
|
Borough |
Zip Code |
|
Telephone No. |
|||||
|
|
|
|
|
|
|
|
|
||||
Hospital/Clinic Chart No. |
II. MEDICAL STATUS |
Contact Person |
|
|
Contact Tel. No. |
|
||||||
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
PATIENT'S MEDICAL RELEASE: I hereby authorize all physicians and medical providers to release any information acquired in the course of my examination of treatment to the New York City HRA/ Dept. of Social Services in connection with my request for home care.
Date: ______________________ |
Signature(X) ________________________________________________ |
|||||
How long have you |
|
Date of this |
|
Place of this |
|
Date of next |
treated the patient? |
|
Examination: |
|
Examination: |
|
Examination: |
|
|
|
||||
A. CURRENT CONDITION
Date of
Onset
1. Primary
Diagnosis/ ICD Code
2. Secondary
Diagnosis/ ICD Code
3.
4.
5.
Check( ) prognosis of each
Anticipated Recovery 6 months ()
Chronic Condition ( )
Deterioration of Present Function Level ()
B. HOSPITAL INFORMATION |
|
|
|
|
|
|
|
|||
|
|
CURRENTLY IN: |
|
|
|
|
Admission |
|
||
|
|
|
|
|
|
|
||||
|
|
(Hospital Name) |
|
|
|
|
|
Date: ____________________________________ |
||
|
|
|
|
|
|
|||||
Reason for |
|
|
|
|
Expected Date |
|
||||
|
|
|
|
of Discharge: |
|
|||||
Hospitalization: ________________________________________________________ |
|
|||||||||
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
Indicate patient’s ability |
|
|
|
|
|
|
|
|
|
|
to take medication: (*) |
C. MEDICATION |
Dosage |
Oral or |
Frequency |
|
1. |
Can |
||||
Parenteral |
|
|||||||||
|
|
|
|
|
|
|
|
|||
1. |
|
|
|
|
|
|
|
2. |
Needs reminding |
|
|
|
|
|
|
|
|
|
|
||
2. |
|
|
|
|
|
|
|
3. |
Needs supervision |
|
|
|
|
|
|
|
|
|
|
||
3. |
|
|
|
|
|
|
|
4. |
Needs help with preparation |
|
|
|
|
|
|
|
|
|
|
||
4. |
|
|
|
|
|
|
|
5. |
Needs administration |
|
|
|
|
|
|
|
|
|
|
||
5. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(*)If patient CANNOT
(a)Can he/she be trained to
Yes
No If no, indicate why not: __________________________________
________________________________________________________________________________________________________________________
(b)What arrangements have been made for the administration of medications? _______________________________________________________
________________________________________________________________________________________________________________________
Page 1 of 3 |
D. MEDICAL TREATMENT |
Does the patient receive any of the following medical treatment? |
Yes |
No |
||||||||
|
|
Indicate medical treatment currently received: ( ) |
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
1. |
Decubitus Care |
|
7. Colostomy Care |
|
15. |
Suctioning |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
2. |
Dressings: Sterile |
|
8. |
Ostomy Care |
|
16. |
Speech/Hearing/ Therapy |
|
|||
|
Simple |
|
|
|
|
|
|
|
|
|
|
|
|
9. |
Oxygen Administration |
|
17. |
Occupational Therapy |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
3. |
Bed bound Care (turning, |
|
10. |
Catheter Care |
|
18. |
Rehabilitation Therapy |
|
|||
|
exercising, positioning) |
|
|
|
|
|
|
|
|
|
|
|
11. |
Tube Irrigation |
|
19. |
Indicate any special |
|
|||||
|
|
|
|
|
|
|
|
|
|
dietary needs |
|
4. |
Ambulation Exercise |
|
12. |
Monitor Vital Signs |
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
5. |
ROM/Therapeutic Exercise |
|
13. |
Tube Feedings |
|
20. |
Other |
||||
|
|
|
|
|
|
|
|
|
|
|
|
6. |
Enema |
|
|
14. |
Inhalation Therapy |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
For each treatment checked, indicate frequency recommended, how the service is currently being provided and what plans have been made to provide the service in the future: (Attach additional documentation as necessary.)
_____________________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________________
Based on the medical condition, do you recommend the provision of service to assist with personal care and/or light housekeeping tasks?
Yes
No
Please indicate contributing factors (e.g. limited range of motion, muscular motor impairments, etc.) and any other information that may be pertinent to the patient's need for assistance with personal care services tasks.
_________________________________________________________________________________________________________________________
_________________________________________________________________________________________________________________________
_________________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________________________
Can patient direct a home care worker?
Yes
No If no, explain below:
____________________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________________
E. EQUIPMENT/SUPPLIES
Please indicate which equipment/supplies the client has, needs or has been ordered.
Has Needs Ordered
Cane
Crutches
Walker
Wheelchair
Hospital Bed
Side Rails
Has Needs Ordered
Bedpan/Urinal
Commode
Diapers
Hoyer Lift
Dressings
Respiratory Aids
Has Needs Ordered
Bath Bar
Bath Seat
Grab Bar
Shower Handle
Other (Specify)
If any needed equipment was not ordered, what other plans have been made to meet this need?
_________________________________________________________________________________________________________________________
_________________________________________________________________________________________________________________________
_________________________________________________________________________________________________________________________
SSN: _________________________________
Page 2 of 3 |
F. REFERRALS
Has a referral been made to any of these agencies: Certified Home Health Agency,
Facility (HRF), a Skilled Nursing Facility (SNF) or the Lombardi Program? |
Yes |
No |
|
|
*IDENTITY AGENCY |
SERVICE |
|
STATUS OF SERVICE |
REFERRAL DATE |
__________________________________ |
__________________________________ |
__________________________________ |
___________________________________ |
|
__________________________________ |
__________________________________ |
__________________________________ |
___________________________________ |
|
G. ADDITIONAL COMMENTS
Describe any other aspects of the patient’s medical, social, family or home situation which affects the patient‘s ability to function, or may affect need for home care. If necessary, please attach an additional sheet(s) explaining the patient’s condition in greater detail.
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
Signature of Person Completing Additional Comments Section
Title Agency
Date
Physician’s Certification
I, the undersigned physician, certify that this patient can be cared for at home, and that I have accurately described his or her medical condition, needs and regimens, including any medication regimens, at the time I examined him or her. I understand that I am not to recommend the number of hours of personal care services this patient may require. I also understand that this physician’s order is subject to the New York State Department of Health regulations at part 515, 516, 517, and 518 of title 18 NYCRR, which permit the department to impose monetary penalties on, or sanction and recover overpayments from, providers or prescribers of medical care, services or supplies when medical care, services or supplies that are unnecessary, improper or exceed the patient’s documented medical condition are provided or ordered.
|
|
|
|
|
|
|
|
|
|
Intern |
|
|
Resident |
||||
*(PRINT) Physician’s Name |
|
|
Specialty |
|
|
*Physician’s Signature |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
*Business Address |
|
|
|
|
|
|
*City |
|
*State |
|
|
*Zip Code |
|||||
Signature date must be within thirty days after medical exam of patient. |
|
|
|
|
|
|
|
|
|||||||||
______________________ |
________________ |
____________________ |
__________________________________ |
_____________________________ |
|
|
|||||||||||
*Date Form Completed |
*Registry Number |
*NPI Number |
|
|
*Physician’s Telephone |
Physician’s |
|||||||||||
Indicate where form was completed: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
___________________________________ |
________________________________________________________ |
__________________________ |
|||||||||||||||
Hospital/Clinic/Institution Name |
|
Address |
Telephone No. / |
||||||||||||||
If Nurse /Social Worker/other person assisted in completing this form:
______________________________ |
_______________________ |
________________________________________________ |
____________________________ |
Name |
Title |
Address |
Telephone No. / |
*Mandatory |
|
|
|
|
|
Page 3 of 3 |
EIGHT HELPFUL HINTS FOR ACCURATE COMPLETION OF THE MEDICAL
REQUEST FOR HOME CARE (M11Q)
* Please provide this sheet to the physician filling out the Medical Request for Home Care
Eight Helpful Hints for Accurate Completion of the
Medical Request for Home Care
1.The client’s name, address and Social Security number must be provided.
2.The medical professional must complete the
3.The medical professional must not recommend or request the number of hours of personal care services.
4.The
5.The date of the examination must be provided.
6.The physician must sign and date the
7.The registry number, NPI (national provider ID), and the complete business address of the physician must be indicated.
8.The completed signed copy of the
Form Characteristics
| Fact Title | Details |
|---|---|
| Purpose | The M11Q form is a Medical Request for Home Care, designed to assess a patient's eligibility for home care services. |
| Date of Creation | The form was created on December 9, 2014. |
| Mandatory Information | Clients must provide their name, address, and Social Security number on the form. |
| Provider Requirements | Only a New York State licensed physician can complete and sign the M11Q. |
| Examination Date | The physician must indicate the date of the patient's examination when submitting the form. |
| Regulatory Compliance | The completion of the form is subject to New York State Department of Health regulations, specifically parts 515, 516, 517, and 518 of title 18 NYCRR. |
| Signature Timeline | The physician must sign and date the form within 30 days of the examination date. |
| Submission Deadline | The completed form must be forwarded within 30 calendar days after the patient's medical examination. |
| Additional Comments | The form allows for additional comments concerning the patient's medical, social, or family situation that may affect home care needs. |
Guidelines on Utilizing M11Q
Filling out the M11Q form accurately is essential for ensuring that appropriate services can be accessed. This form requires detailed medical information and authorizations that need to be gathered before submission. Follow these steps to effectively complete the M11Q form.
- At the top of the form, write down the District Office and the Case Load Number. Fill in the Return Date. Provide the Address where the form will be sent, including the Borough, Zip Code, and Telephone Number.
- In the CLIENT INFORMATION section, fill in the patient's Name, Birthdate, Social Security Number, Medicaid Number, Home Address, Borough, Zip Code, and Telephone Number. Enter the Hospital/Clinic Chart Number.
- Provide details about the Contact Person and their Telephone Number.
- In the PATIENT'S MEDICAL RELEASE section, sign and date the authorization for physicians to release necessary medical information.
- Specify how long the physician has treated the patient and indicate the Date of Examination and Place of Examination.
- In the CURRENT CONDITION section, list the primary and secondary diagnoses along with their respective ICD codes. Note the Date of Onset and check the appropriate boxes for prognosis.
- Provide information about the hospital if the patient is currently admitted, including the Admission Date, Reason for Hospitalization, and Expected Date of Discharge. Indicate the patient’s ability to take medication.
- In the MEDICATION section, list medication names, dosages, administration methods, and any needs the patient may have related to medication administration.
- In the MEDICAL TREATMENT section, check any types of treatment the patient is currently receiving and provide relevant details.
- Indicate whether assistance for personal care and light housekeeping tasks is recommended. Provide any contributing factors affecting the patient's ability to perform these tasks and whether the patient can direct a home care worker.
- List any EQUIPMENT/SUPPLIES the client has or needs. Describe any plans made to meet equipment needs not already ordered.
- Answer questions regarding REFERRALS by indicating if a referral has been made to any relevant agencies. Include agency details and the status of the service.
- In the ADDITIONAL COMMENTS section, describe any other relevant medical or social factors affecting the patient's situation. Attach extra sheets if necessary.
- The physician must complete the Physician’s Certification section. This includes the physician’s name, specialty, signature, and contact information. Ensure that the certification date is within 30 days of examination.
- If assistance was provided by a nurse or social worker in completing the form, include their details in the designated area.
After completing the M11Q form, ensure that all sections are thoroughly filled out. The signed form should be submitted promptly to avoid delays in processing. Double-check that all mandatory fields are completed to ensure the best chance of a smooth review process.
What You Should Know About This Form
What is the M11Q form and why is it important?
The M11Q form, also known as the Medical Request for Home Care, is an essential document used in New York City to facilitate home care services for patients. This form collects critical information about a patient's medical condition, needs, and home care requirements. It is completed by a licensed physician and ensures that patients receive appropriate medical assessments for the home care services they require. Completing this form accurately is vital for obtaining approval for necessary care, which can greatly enhance a patient's quality of life while allowing them to remain in their home environment.
Who is responsible for completing the M11Q form?
The responsibility for completing the M11Q form falls primarily on a licensed physician who is familiar with the patient's medical history and current condition. Physicians must provide detailed information regarding the patient's diagnoses, treatments, and any additional needs for home care. It is imperative that this section is filled out comprehensively to support the patient's request for services. In some cases, a nurse or social worker may assist in gathering information, but ultimately, a qualified physician must sign and complete the form to ensure its validity.
What specific information is required on the M11Q form?
The M11Q form requires a variety of information aimed at painting a complete picture of the patient's health. Key details include the patient's identifying information, primary and secondary diagnoses, current medical treatments, medication administration capabilities, and any special equipment needs. Additionally, the physician must describe the patient's ability to perform daily activities and whether they can direct home care workers. All of this information is crucial for determining eligibility for home care services and must be documented accurately.
What happens after the M11Q form is completed?
Once the M11Q form is completed and signed by the physician, it needs to be submitted to the appropriate home care services agency or the New York City Human Resources Administration (HRA). The agency will review the information provided to determine the patient's eligibility for home care services. It is important that the completed form is submitted within 30 calendar days after the medical examination to avoid delays in care. The agency will then make a decision regarding the necessary services, ensuring the patient receives the support they need in a timely manner.
Common mistakes
Completing the M11Q form correctly is crucial for ensuring that patients receive the necessary home care services. However, many individuals make common mistakes that can delay processing or lead to denials. Here are nine common errors to avoid.
1. Missing Patient Information: One of the most frequent errors is failing to include complete patient details, such as the full name, date of birth, and Social Security number. Any missing information can lead to delays in processing the form.
2. Inaccurate Medical Descriptions: It’s important that the medical professional describes the patient’s condition accurately. Vague or incomplete descriptions can create confusion and result in inadequate care being recommended.
3. Recommendations for Care Hours: Some practitioners mistakenly recommend specific hours of personal care services. The form explicitly states that professionals are not to request this information. Doing so can invalidate the request.
4. Signature Issues: The M11Q form must be signed by a licensed physician in New York State. A common mistake occurs when other healthcare professionals sign the form or when there is no signature at all.
5. Examination Dates: Failing to include the date of the examination can lead to complications. It is vital that this date is provided accurately to ensure compliance with processing timelines.
6. Timeliness of the Submission: Physicians need to sign and date the form within 30 days of the examination. If it isn't submitted on time, it may be rejected, necessitating the completion of a new form.
7. Missing Registry and NPI Numbers: The completion of the registry number and National Provider Identifier (NPI) is mandatory. Omitting these could impede the verification of the physician’s status.
8. Incomplete Additional Comments Section: The additional comments section often goes underutilized. Providing necessary context about the patient’s social or home situation can be crucial for determining care needs.
9. Forwarding the Form Late: Finally, the completed and signed M11Q must be submitted within 30 calendar days after the medical examination. Delays in sending the form can affect the patient’s home care eligibility.
By being aware of these common mistakes and taking steps to avoid them, both healthcare providers and patients can ensure a smoother process in securing necessary home care services.
Documents used along the form
The M11Q form, also known as the Medical Request for Home Care, plays a crucial role in requesting home care services. Several other forms and documents often accompany it to facilitate the assessment and delivery of home care. Here is a list of these documents, detailing their purpose and importance.
- Authorization for Release of Medical Information: This document allows health care providers to share a patient's medical details with relevant authorities or agencies, ensuring that the home care request is backed by accurate health information.
- Client Assessment Form: This form gathers comprehensive information about the client's medical history, living situation, and personal care needs. It serves as a baseline for healthcare providers to determine the level of care required.
- Plan of Care: Developed by healthcare professionals, this outlines specific services and interventions the client will receive. It ensures a coordinated approach in managing the patient’s home care services.
- Consent for Home Health Services: This document is a formal agreement between the client and the home health agency, consenting to the provided care and the terms of service.
- Insurance Authorization Form: Used to verify a patient's insurance benefits, this form assists in determining coverage for home care services, aiding in financial planning and service approval.
- Patient Experience Survey: A feedback tool used to evaluate the quality of care provided. Gathering this information helps agencies improve their services and address any client concerns.
- Physician’s Order for Home Care: Similar to the M11Q, this document outlines the specific medical treatments and therapies the patient needs at home, reinforcing the physician’s recommendations.
- Emergency Contact Form: This form collects critical contact information for family members or caregivers who can be reached in case of emergencies concerning the patient’s care.
- Home Care Agreement: This document formally outlines the responsibilities of the home health agency and the client. It ensures that both parties understand their roles and expectations during the care process.
These documents complement the M11Q form, facilitating a comprehensive approach to home care that addresses medical, financial, and personal needs. Proper completion and coordination of these forms can streamline the entire process, ensuring clients receive the care they require promptly and effectively.
Similar forms
- Home Health Certification Form: This document is similar in that it verifies a patient's need for home healthcare services, including a medical evaluation by a doctor.
- Request for Medical Services: Like the M11Q, it requires detailed patient information and authorizes healthcare providers to share medical data for care coordination.
- Physician's Order for Home Care: This form also outlines the type of medical services a patient requires at home based on their condition and treatment plan.
- Home Care Needs Assessment: It assesses the specific needs of a patient for home care, similar to how the M11Q evaluates medical status and home care requirements.
- Patient Medical Release Form: This document allows medical professionals to disclose information about a patient, closely paralleling the authorization aspect of the M11Q.
- Care Plan Template: This form sets out a patient’s care strategy and needs, much like how the M11Q details the services protocol based on medical conditions.
- Medicaid Home Care Application: It is used to secure funding for home care services, similarly to how the M11Q supports requests for such assistance.
- Certificate of Medical Necessity: This document validates the need for medical equipment or services and is akin to how the M11Q captures medical needs for home support.
Dos and Don'ts
- Do: Provide accurate client information, including the client’s name, address, and Social Security number.
- Don’t: Leave out details about the patient’s medical condition; ensure the medical professional thoroughly describes it.
- Do: Ensure the form is signed by a physician who is licensed in New York State.
- Don’t: Recommend the number of hours for personal care services; this is not permitted.
- Do: Include the date of the medical examination on the form.
- Don’t: Forget to sign and date the M-11Q within 30 days following the examination.
- Do: Provide the physician’s registry number, NPI, and full business address on the form.
- Don’t: Delay sending the completed form; it must be forwarded within 30 calendar days after the exam.
Misconceptions
1. The M11Q form is only for people with severe disabilities. This form is used for various medical requests and is not limited to severe disabilities. Individuals with different health needs can also benefit from this form.
2. Only doctors can fill out the M11Q form. While a physician must sign the form, other qualified medical professionals, such as nurse practitioners or social workers, can assist in completing it.
3. The M11Q form guarantees home care services. Filling out the M11Q is a necessary step, but it does not guarantee that services will be approved. Each case is evaluated individually.
4. You can request a specific number of care hours on the M11Q. The form explicitly states that the medical professional should not request specific hours of service. That decision is made through further evaluation processes.
5. The M11Q form must be completed on the same day as the medical exam. Although it’s best for the form to reflect recent medical status, the completed form must be submitted within 30 days of the exam date.
6. Any healthcare provider can provide a signature on the M11Q. Only a licensed physician in New York State can sign the M11Q. Signatures from other professionals will not be accepted.
7. The M11Q form doesn't require additional supportive documents. If more information is needed, it is permissible and often advisable to attach additional documentation to support the patient's home care request.
8. It's okay to leave sections of the M11Q form blank. Every section is important and must be completed to ensure a comprehensive understanding of the patient's needs. Incomplete forms may delay the process.
9. Anyone can access the M11Q after it’s filled out. This form contains sensitive personal and medical information, and access is limited to authorized individuals only, ensuring patient privacy is upheld.
10. The M11Q is a one-size-fits-all form for home care requests. Each patient's situation is unique. The M11Q helps assess individual needs, allowing for specific recommendations for care tailored to the patient's condition.
Key takeaways
Filling out the M11Q form is a crucial step in the process of requesting home care services. Here are some key takeaways to keep in mind:
- Accurate Client Information: Ensure the client's name, address, and Social Security number are correctly listed at the beginning of the form.
- Detail Medical Condition: The medical professional must provide a detailed description of the patient’s medical status, as this will impact the level of care needed.
- No Hour Recommendations: The physician should not determine the number of hours of personal care services required. This decision is made later in the evaluation process.
- Physician's Signature Required: The M11Q form must be signed by a New York State licensed physician to validate the request.
- Examination Date: It’s important to include the date of the medical examination. This information helps to ensure the request is timely.
- 30-Day Rule: The physician needs to sign and date the M11Q form within 30 days after the patient's examination. This keeps the information current and relevant.
- Registry and NPI Numbers: The form must include the registry number, National Provider ID (NPI), and complete business address of the physician.
- Timely Submission: After completing and signing the M11Q, submit the form within 30 calendar days from the date of examination to avoid delays in processing.
- Additional Comments: Utilize the section for additional comments to provide any other information that may assist in understanding the patient’s needs for home care services.
Following these guidelines can help streamline the application process for home care services and ensure that all essential information is considered.
Browse Other Templates
Beneficiary Update Request,Beneficiary Designation Modification,Beneficiary Assignment Change,Beneficiary Information Update,Beneficiary Selection Form,Beneficiary Nomination Document,Beneficiary Revision Form,Beneficiary Declaration Form,Beneficiary - Include the date on which the form is signed to establish the effective date.
Starbucks Vacancies - Review the at-will employment statement to understand your employment rights.
Lic2 - Any unpaid fees associated with the electrician’s license must be disclosed.