Fill Out Your Mc 371 Form
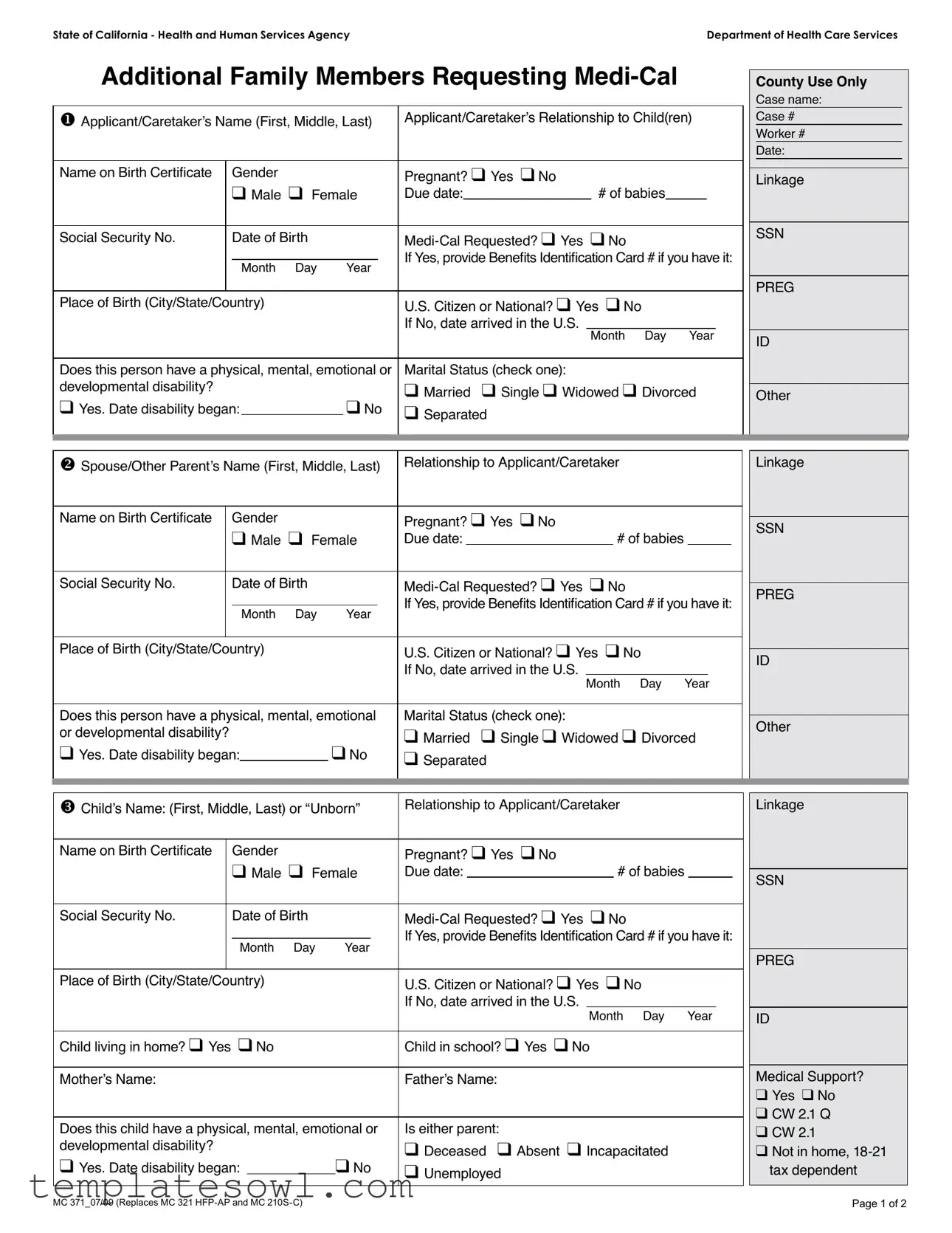
The MC 371 form is essential for families in California seeking to enroll additional members in the Medi-Cal program. Designed by the Health and Human Services Agency, this form facilitates the collection of vital information regarding the applicant and the family members seeking coverage. Applicants must provide details such as their name, relationship to the child, and various personal attributes, including date of birth and Social Security number. The form also gathers information on the health status of family members, including any disabilities and current health care coverage. Notably, questions regarding pregnancy and marital status are included to ensure the Medi-Cal program can accurately assess eligibility. It’s crucial that applicants are thorough and accurate, as the information will affect their access to medical services. By filling out this form, families can take a significant step toward obtaining the healthcare coverage they need.
Mc 371 Example
State of California - Health and Human Services Agency |
Department of Health Care Services |
Additional Family Members Requesting
u Applicant/Caretaker’s Name (First, Middle, Last) |
Applicant/Caretaker’s Relationship to Child(ren) |
|||||||
|
|
|
|
|
|
|
|
|
Name on Birth Certiicate |
Gender |
|
|
Pregnant? q Yes q No |
||||
|
|
q Male q Female |
Due date: _______________ # of babies_____ |
|||||
|
|
|
|
|
|
|
|
|
Social Security No. |
|
Date of Birth |
|
|
||||
|
|
|
|
|
|
If Yes, provide Beneits Identiication Card # if you have it: |
||
|
|
Month Day |
Year |
|||||
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
Place of Birth (City/State/Country) |
|
|
U.S. Citizen or National? q Yes q No |
|||||
|
|
|
|
|
|
If No, date arrived in the U.S. |
|
|
|
|
|
|
|
|
|
Month Day Year |
|
|
|
|
|
|
|
|
||
Does this person have a physical, mental, emotional or |
Marital Status (check one): |
|||||||
developmental disability? |
|
|
|
|
|
q Married q Single q Widowed q Divorced |
||
q Yes. Date disability began: |
|
q No |
q Separated |
|||||
|
||||||||
|
|
|
|
|
|
|
|
|
County Use Only
Case name:
Case #
Worker #
Date:
Linkage
SSN
PREG
ID
Other
v Spouse/Other Parent’s Name (First, Middle, Last) |
Relationship to Applicant/Caretaker |
|
|
|
|
|
Linkage |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name on Birth Certiicate |
|
Gender |
|
|
Pregnant? q Yes q No |
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
SSN |
||||||
|
|
q Male q Female |
Due date: |
|
|
|
# of babies |
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Social Security No. |
|
Date of Birth |
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
PREG |
||||||||
|
|
|
|
|
|
If Yes, provide Beneits Identiication Card # if you have it: |
|
|||||||||
|
|
|
|
|
|
|
|
|||||||||
|
|
|
Month Day |
Year |
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Place of Birth (City/State/Country) |
|
|
U.S. Citizen or National? q Yes |
q No |
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
ID |
|||||||||
|
|
|
|
|
|
If No, date arrived in the U.S. |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
Month Day |
Year |
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Does this person have a physical, mental, emotional |
Marital Status (check one): |
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
Other |
|||||||||
or developmental disability? |
|
|
|
|
q Married q Single q Widowed q Divorced |
|
||||||||||
|
|
|
|
|
|
|||||||||||
q Yes. Date disability began: |
q No |
q Separated |
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
w Child’s Name: (First, Middle, Last) or “Unborn” |
Relationship to Applicant/Caretaker |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
Name on Birth Certiicate |
Gender |
|
Pregnant? q Yes q No |
|
|
|
|
|
|||
|
q Male q Female |
Due date: |
|
|
|
# of babies |
|
|
|
||
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
Social Security No. |
Date of Birth |
|
|||||||||
|
_____ _____ ______ |
If Yes, provide Beneits Identiication Card # if you have it: |
|||||||||
|
Month Day |
Year |
|||||||||
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
Place of Birth (City/State/Country) |
|
U.S. Citizen or National? q Yes |
q No |
||||||||
|
|
|
|
If No, date arrived in the U.S. |
|
|
|
|
|
|
|
|
|
|
|
|
|
Month Day Year |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
Child living in home? q Yes q No |
|
Child in school? q Yes q No |
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
Mother’s Name: |
|
|
|
Father’s Name: |
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
Does this child have a physical, mental, emotional or |
Is either parent: |
|
|
|
|
|
|||||
developmental disability? |
|
|
|
q Deceased q Absent q Incapacitated |
|||||||
q Yes. Date disability began: |
q No |
q Unemployed |
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
Linkage
SSN
PREG
ID
Medical Support? q Yes q No
q CW 2.1 Q q CW 2.1
qNot in home,
MC 371_07/09 (Replaces MC 321 |
Page 1 of 2 |
x |
Is anyone currently covered by health/dental insurance or Medicare? q Yes q No |
q DHCS 6155 |
|
|
|
|
||||||||||||||
|
If so, who? |
|
|
|
|
|
OHC Code: |
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
y |
Has anyone iled a lawsuit because of an accident or injury? q Yes q No |
q DHCS 6268 |
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
z Do you or any family member want |
q MC 210 A |
|
|
|
|
|||||||||||||||
|
and wish to apply for |
|
|
|
|
|
Retroactive Coverage |
|||||||||||||
|
List name(s): |
Month(s) of coverage: |
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
Month |
Month |
|
Month |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
1 |
|
|
2 |
3 |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Have you or any family member ever been in U.S. military service? q Yes q No |
q CW 5 |
|
|
|
|
|
|
||||||||||||
|
If Yes, who? Name(s): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
Relationship: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The |
|
|
|
|
|
|
|
|
|
|
||||||||||
|
• |
We will share your child’s application with Healthy Families if your child no longer qualiies for free |
||||||||||||||||||
do not want us to share it, check here q
• We will share your child’s application with Healthy Kids or similar county program if your child does not qualify for
Family Income: List the income of every person listed in this application. Include child support and spousal support received. (Use a separate line for each source of income.)
Name of person with Income |
Source of Income |
How often is income |
How much is |
Social Security No. |
(Children who are in school do not have to list |
(Job, social security, |
received? |
the income? |
(Optional) |
their income from a job.) |
pension, etc.) |
(Weekly, biweekly, monthly) |
(Total gross |
|
|
|
|
income) |
|
|
|
|
|
|
|
|
|
$ |
|
|
|
|
|
|
|
|
|
$ |
|
|
|
|
|
|
|
|
|
$ |
|
|
|
|
|
|
|
|
|
$ |
|
|
|
|
|
|
|
|
|
$ |
|
|
|
|
|
|
Expenses: List the monthly expenses for all persons listed above.
Child Day Care or Disabled Dependent Care
For (child or dependent’s name):__________________________________________ Age: ______ Amount Paid: _____________
How Often?______________
For (child or dependent’s name):__________________________________________ Age: _______ Amount Paid: ____________
How Often? _____________
Paid to: ________________________________ Paid by: _________________________________ Amount paid:_____________
Paid to: ________________________________ Paid by: _________________________________ Amount paid:_____________
Please note that additional information about your property, income and/or resources may be required if applicable.
I certify that I have read and understand the information above. I also certify that the information I have given on this form is true and correct.
Signature_____________________________________________________________________ Date: ________________
MC 371_07/09 (Replaces MC 321 |
Page 2 of 2 |
Form Characteristics
| Fact Name | Description |
|---|---|
| Form Purpose | The MC 371 form is used to request Medi-Cal coverage for additional family members. |
| Governing Law | This form operates under California state laws regarding Medicaid eligibility. |
| Applicant Information | The form requests essential details from the applicant or caretaker, including their name, relationship to the child, and social security number. |
| Pregnancy Status | It includes a section to identify if the applicant or family member is pregnant, alongside the due date and number of babies. |
| Disability Inquiry | The form asks whether any family member has a physical, mental, or developmental disability, requiring additional details if applicable. |
| U.S. Citizenship | Individuals must indicate their U.S. citizenship status and, if not a citizen, the date of their arrival in the U.S. |
| Income Reporting | Applicants must list income sources for all household members, specifying how often it is received and the total gross amount. |
| Expense Disclosure | Monthly expenses related to child care and spousal or child support payments must also be detailed. |
| Certification Statement | Applicants must certify that all information provided is accurate and truthful, under penalty of perjury. |
| Form Versions | The current version is MC 371_07/09, which replaces earlier forms MC 321 HFP-AP and MC 210S-C. |
Guidelines on Utilizing Mc 371
After gathering all necessary personal information and documents, you can proceed to fill out the MC 371 form. This form allows families to request Medi-Cal benefits for additional members. It is essential to complete it accurately to ensure a smooth application process. Here are the steps to guide you through filling out the form:
- Applicant/Caretaker’s Information: Start by entering the applicant or caretaker’s full name, relationship to the child, and gender. Indicate if the individual is pregnant, and if so, provide the due date and number of babies.
- Social Security Number: Write the applicant’s Social Security number along with the date of birth and place of birth (city, state, country).
- U.S. Citizenship: Check whether the applicant is a U.S. citizen or national. If not, include the date when they arrived in the U.S.
- Disability Information: Indicate if the applicant has a physical, mental, emotional, or developmental disability and provide the date the disability began, if applicable.
- Marital Status: Select the marital status from options like married, single, widowed, divorced, or separated.
- Spouse/Other Parent Information: Fill in the spouse or other parent’s name, relationship to the applicant, gender, and pregnancy status, if relevant.
- Children’s Information: For each child (including unborn), list their names, gender, Social Security number, date of birth, place of birth, and indicate if they are living in the home or attending school.
- Health/Dental Insurance: State whether anyone is currently covered by health or dental insurance or Medicare.
- Military Service: Indicate if any family member has served in the U.S. military, including their names and relationships.
- Income Details: List the income for every person in the application, specifying the source and amount received.
- Expense Information: Document monthly expenses, including any child or spousal support payments.
- Certification: Sign and date the form, confirming the accuracy of the provided information.
Make sure to review the completed form for any missing information or errors before submitting it to ensure a comprehensive and accurate application for Medi-Cal benefits.
What You Should Know About This Form
What is the purpose of the MC 371 form?
The MC 371 form is used in California to request Medi-Cal coverage for additional family members. It gathers essential information about the applicant, their relationship to the child or children, and any existing health coverage. The form helps determine eligibility for Medi-Cal, a program offering free or low-cost health insurance to eligible individuals and families.
Who should complete the MC 371 form?
The form should be completed by the applicant or caretaker who is responsible for the child or children applying for Medi-Cal. This individual should provide accurate information about themselves and the children, including details such as social security numbers, date of birth, and birth certificate names.
What information is required on the MC 371 form?
The MC 371 form requires personal details for the applicant and all additional family members. This includes names, gender, social security numbers, dates of birth, citizenship status, and any disabilities. Additionally, information about income, expenses, and existing health insurance is essential. Accurate completion of the form is crucial for eligibility assessment.
Can the MC 371 form be submitted in a language other than English?
Is there a deadline for submitting the MC 371 form?
While there is no specific deadline, it is recommended to submit the form as soon as possible to avoid delays in obtaining Medi-Cal coverage. Timely submission is crucial for receiving benefits, especially if there are immediate medical needs or if retroactive coverage is being requested.
What happens after the MC 371 form is submitted?
Upon submission, the form will be reviewed by the local Medi-Cal office. A caseworker will assess the information for completeness and accuracy. Applicants may be contacted for additional information. If approved, individuals will receive a Medi-Cal Benefits Identification Card outlining their coverage.
What should I do if I make a mistake on the form?
If a mistake is made on the MC 371 form, it is important to correct it immediately. Contact the local Medi-Cal office for guidance on how to rectify the error. This will help ensure that eligibility is properly assessed and that potential issues do not arise during the approval process.
Common mistakes
Filling out the MC 371 form can be challenging, and errors may lead to delays or complications in receiving Medi-Cal benefits. One common mistake occurs when applicants fail to provide complete names as they appear on legal documents. It is essential to use full first, middle, and last names, as any variation may result in rejection of the application.
Another frequent error is not indicating the correct relationship to the child(ren). The form requires clarity regarding the applicant or caretaker’s connection to each child. Failing to specify this relationship could confuse processing staff and hinder timely approval.
Omitting the Social Security number is a critical oversight. Each applicant and member listed must have their Social Security number included, unless specifically exempt. Leaving this field blank can cause significant delays, as the agency needs this information to verify identities and eligibility.
Providing inaccurate information about residency status is another mistake that can have serious implications. Applicants must clearly indicate whether they are U.S. citizens or nationals, or if they are not, the date they arrived in the U.S. Misrepresenting residency can lead to disqualification from benefits.
Many also overlook the section regarding physical or developmental disabilities. Not checking "Yes" when applicable can prevent extra support and resources from being provided. Accurately representing the health needs of all family members is crucial.
Failing to report all sources of income is another common pitfall. Each person’s income must be disclosed clearly, including child support and spousal support. This ensures that eligibility is assessed accurately, taking into account all financial resources.
Lastly, applicants sometimes neglect the expenses section, where they are required to detail monthly spending for childcare or medical support. Providing this information is key to understanding the financial situation of the family and its needs, which ultimately influences the Medi-Cal evaluation.
In summary, careful attention to detail is paramount when completing the MC 371 form. Errors can lead to lengthy processing times and potentially limit access to vital health care services.
Documents used along the form
When applying for Medi-Cal, various forms and documents may be required in addition to the MC 371 form. Each of these documents serves a unique purpose in ensuring an accurate and comprehensive application for health care assistance. Below is a list of common forms and documents that may accompany the MC 371 form.
- MC 210 A: This form is used to apply for Medi-Cal benefits for medical expenses incurred in the last three months. It is essential for those seeking retroactive coverage.
- DHCS 6268: This document gathers information on whether any similar health benefits exist due to an accident or injury. It helps the Department of Health Care Services assess liability and information sharing.
- DHCS 6155: This form is used to report any existing health or dental insurance coverage that family members may have, which can impact Medi-Cal eligibility.
- CW 2.1: This form gathers pertinent information regarding family structure and is critical for assessing a child's eligibility for Medi-Cal and other programs.
- CW 5: This document inquires about military service for applicants. It is essential, as it may affect health care benefits and services available.
- Required Income Documentation: Applicants should provide evidence of income, including sources such as pay stubs and tax returns. This information is crucial for determining eligibility.
- Expense Verification: Applicants are required to list monthly expenses like child care or spousal support. Providing this information ensures a complete financial assessment.
- Social Security Number Documentation: It is necessary to provide Social Security Numbers for everyone listed on the application to verify identity and eligibility.
- Proof of Residency: Documentation required may include utility bills or rental agreements that confirm a family's current address. Proof of residency helps establish eligibility based on local program guidelines.
- Birth Certificates: Copies of birth certificates for all dependents are often requested. This is used to verify identity, age, and eligibility for Medi-Cal benefits.
Each of these forms and documents plays a significant role in facilitating a smooth application process for Medi-Cal. Ensuring all required materials are submitted can help increase the likelihood of a timely response from the appropriate health care services.
Similar forms
The MC 371 form functions primarily as a request for Medi-Cal benefits for additional family members. There are various other documents that serve similar purposes, notably in the context of applying for healthcare-related assistance and benefits. Below are five documents that share similarities with the MC 371 form:
- MC 210 A: This form is a Medi-Cal application for individuals seeking retroactive coverage for medical expenses incurred in the past three months. Just like the MC 371, it collects detailed information about the applicant and any additional family members for eligibility assessment.
- MC 210S-C: Serving as a revision of the MC 210 application, this document specifically caters to families with children under the age of 19. Both forms inquire about family size, income, and medical needs to determine eligibility for Medi-Cal assistance.
- DHCS 6155: This form allows individuals to disclose health insurance coverage details for family members. Similarly to the MC 371, it collects reliance on medical support for evaluating the need for Medi-Cal benefits.
- CW 2.1: The CW 2.1 form requests further information about a household’s income and expenses, playing a crucial role in assessing eligibility for multiple assistance programs. The income reporting process is akin to the one outlined in the MC 371 form.
- DHCS 6268: This document pertains to reporting any lawsuits related to accidents or injuries. It complements information necessary for determining overall healthcare coverage needs, similar to aspects covered in the MC 371 related to injury claims and coverage for medical expenses.
Dos and Don'ts
When filling out the MC 371 form for Medi-Cal, it is essential to follow certain guidelines to ensure a smooth application process.
- Do: Provide accurate and complete information for each member listed.
- Do: Include all income sources for everyone in the application.
- Do: Check the correctness of Social Security numbers and dates of birth.
- Do: Mark clearly if any family member has a disability.
- Don't: Leave any sections blank; if information does not apply, indicate that it is not applicable.
- Don't: Rush through the form; take your time to review all answers carefully before submitting.
Following these guidelines can help prevent delays and ensure that your application is processed efficiently.
Misconceptions
Understanding the MC 371 form is crucial for those navigating the Medi-Cal application process. However, there are several misconceptions about it. Here is a clear breakdown of these misunderstandings:
- Misconception 1: The MC 371 form is only for new applicants.
- Misconception 2: All family members must meet income requirements individually.
- Misconception 3: The form needs to be filled out in one sitting.
- Misconception 4: Applicants need to provide physical copies of all income documentation.
- Misconception 5: The MC 371 form is only for families with children.
- Misconception 6: Once submitted, the application status cannot be checked.
- Misconception 7: It's unnecessary to keep copies of the submitted form.
- Misconception 8: All medical expenses must be reported in detail.
- Misconception 9: Applicants can only apply for Medi-Cal during open enrollment.
This form can be used for both new applicants and current Medi-Cal recipients looking to add additional family members.
The income is assessed collectively for the household, not per individual family member.
You can gather the required information over time. However, timely submission is important to avoid delays.
While you do need to report income, electronic documentation can suffice in certain cases.
Any family member can be added to the Medi-Cal request, including spouses and other dependents.
You can check your application's status by contacting your local Medi-Cal office after a few weeks.
For your records, always keep a copy of any forms you submit, as this information may be needed later.
Only those relevant to the Medi-Cal request may be necessary to report; detailed records are not always required.
Medi-Cal applications can be submitted year-round, especially for those who qualify due to major life changes.
Clarifying these misconceptions is vital for ensuring that the application process runs smoothly and efficiently.
Key takeaways
1. The MC 371 form is primarily used to request Medi-Cal benefits for additional family members. Ensure that all required data is accurately filled out to prevent delays in processing.
2. The applicant's or caretaker's name, along with their relationship to the children, must be clearly listed at the beginning of the form.
3. For each family member, input essential details such as their date of birth, gender, and Social Security number, if available. This information is crucial for determining eligibility.
4. If any family members are pregnant, specify the due date and number of babies expected. This helps assess coverage needs effectively.
5. Verify the citizenship status for each family member. Indicate if they are a U.S. citizen or national; if not, provide the date they arrived in the U.S.
6. Document any disabilities by checking the appropriate box and providing the start date if applicable. This information can influence the level of support received.
7. Disclose family income accurately by listing all sources, including child and spousal support. Specify how frequently this income is received.
8. Enter monthly expenses related to child or disabled dependent care. This can enhance the assessment of financial needs, even if further documentation may be requested.
9. After completing the form, sign and date it. This certification affirms that the information provided is correct. Inaccuracies may lead to complications in the application process.
Browse Other Templates
WITS Access Application,Wisconsin Incident Reporting Access Form,F-20483 WAMS User Request,WITS User Account Request,Wisconsin Health Services Web Access Form,Access Authorization for WITS,Incident Tracking System Access Form,WITS System Access Reque - A section is available for detailing incidents involving elder adults-at-risk.
Dhs 38 Verification of Employment - The signature of the employer on the form indicates acknowledgment of the information’s importance.
Wells Fargo Beneficiary Form - The form includes general provisions that participants should read carefully.