Fill Out Your Med 9 Form
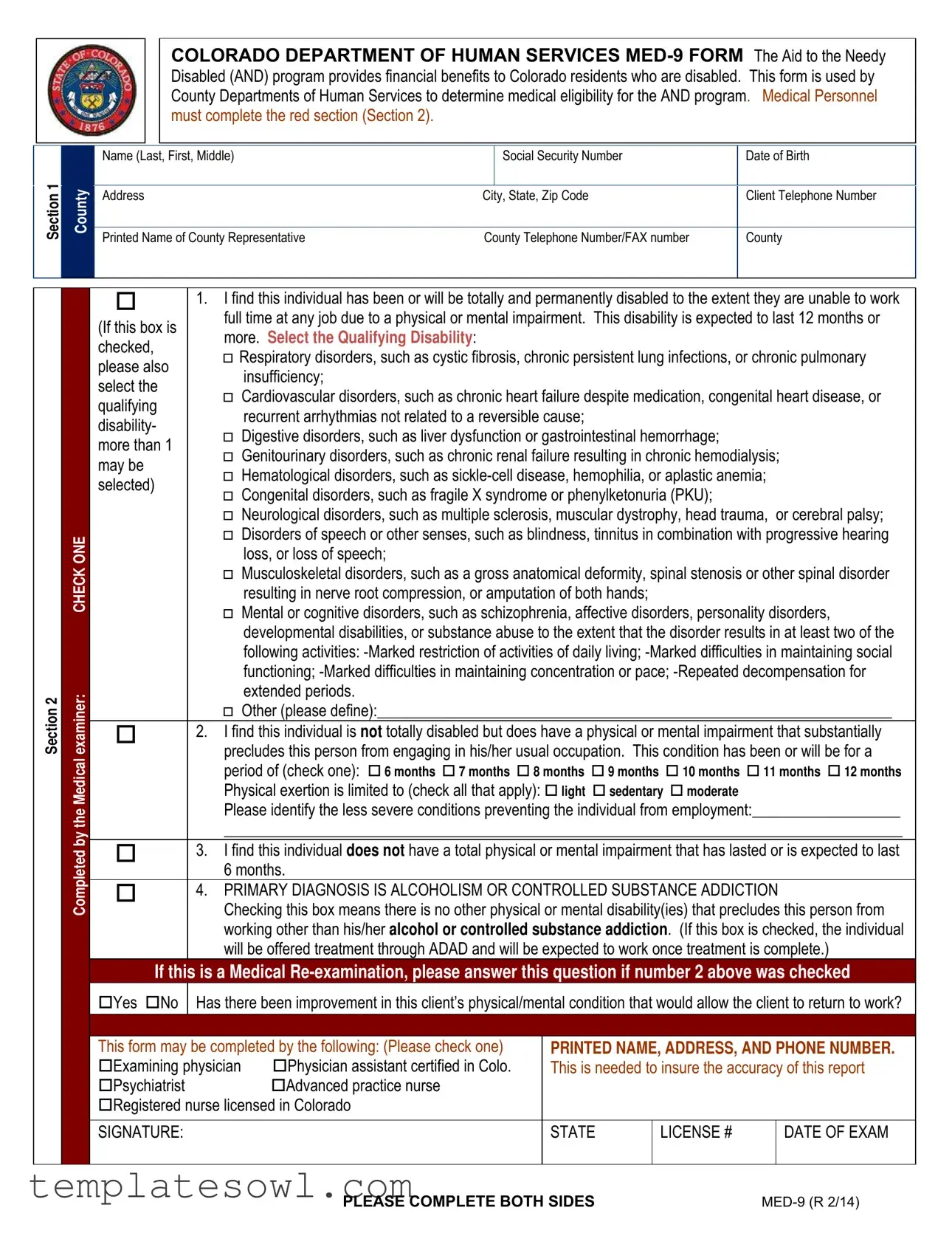
The Med 9 form plays a critical role in supporting individuals with disabilities in Colorado by assessing their eligibility for financial assistance under the Aid to the Needy Disabled (AND) program. Designed to streamline the evaluation process, this form is completed by County Departments of Human Services and includes several sections that capture essential personal information, medical assessments, and eligibility criteria. Section 1 gathers basic details such as the applicant’s name, address, date of birth, and social security number. Medical personnel are responsible for filling out Section 2, where they evaluate the individual’s medical condition. They must check one of four boxes to indicate the extent of the disability, ranging from total and permanent disability to conditions that only partially limit the individual's ability to work. The form covers a wide range of physical and mental impairments including respiratory, cardiovascular, neurological, and substance-related disorders. These clinical assessments help determine not just the nature of the disability but also the expected duration and impact on daily living and work capabilities. Completing the Med 9 form requires careful attention to detail, as it serves as a basis for financial support decisions impacting livelihood and quality of life for many individuals in need.
Med 9 Example
Section 1
County
COLORADO DEPARTMENT OF HUMAN SERVICES
Name (Last, First, Middle) |
|
Social Security Number |
Date of Birth |
|
|
|
|
Address |
City, State, Zip Code |
Client Telephone Number |
|
|
|
|
|
Printed Name of County Representative |
County Telephone Number/FAX number |
County |
|
|
|
|
|
Section 2
CHECK ONE
Completed by the Medical examiner:
|
1. I find this individual has been or will be totally and permanently disabled to the extent they are unable to work |
||||||
(If this box is |
full time at any job due to a physical or mental impairment. This disability is expected to last 12 months or |
||||||
more. Select the Qualifying Disability: |
|
|
|
||||
checked, |
|
|
|
||||
|
Respiratory disorders, such as cystic fibrosis, chronic persistent lung infections, or chronic pulmonary |
||||||
please also |
|||||||
|
|
insufficiency; |
|
|
|
||
select the |
|
|
|
|
|
||
|
|
Cardiovascular disorders, such as chronic heart failure despite medication, congenital heart disease, or |
|||||
qualifying |
|
||||||
|
|
recurrent arrhythmias not related to a reversible cause; |
|
|
|||
disability- |
|
|
|
|
|||
|
|
Digestive disorders, such as liver dysfunction or gastrointestinal hemorrhage; |
|
||||
more than 1 |
|
|
|||||
|
|
Genitourinary disorders, such as chronic renal failure resulting in chronic hemodialysis; |
|||||
may be |
|
||||||
|
|
Hematological disorders, such as |
|
||||
selected) |
|
|
|||||
|
|
Congenital disorders, such as fragile X syndrome or phenylketonuria (PKU); |
|
||||
|
|
|
|||||
|
Neurological disorders, such as multiple sclerosis, muscular dystrophy, head trauma, |
or cerebral palsy; |
|||||
|
Disorders of speech or other senses, such as blindness, tinnitus in combination with progressive hearing |
||||||
|
|
|
loss, or loss of speech; |
|
|
|
|
|
Musculoskeletal disorders, such as a gross anatomical deformity, spinal stenosis or other spinal disorder |
||||||
|
|
|
resulting in nerve root compression, or amputation of both hands; |
|
|
||
|
Mental or cognitive disorders, such as schizophrenia, affective disorders, personality disorders, |
||||||
|
|
|
developmental disabilities, or substance abuse to the extent that the disorder results in at least two of the |
||||
|
|
|
following activities: |
||||
|
|
|
functioning; |
||||
|
|
|
extended periods. |
|
|
|
|
|
Other (please define):__________________________________________________________________ |
||||||
|
2. I find this individual is not totally disabled but does have a physical or mental impairment that substantially |
||||||
|
precludes this person from engaging in his/her usual occupation. This condition has been or will be for a |
||||||
|
period of (check one): 6 months 7 months 8 months 9 months 10 months 11 months 12 months |
||||||
|
Physical exertion is limited to (check all that apply): light sedentary moderate |
|
|||||
|
Please identify the less severe conditions preventing the individual from employment:___________________ |
||||||
|
_______________________________________________________________________________________ |
||||||
|
3. I find this individual does not have a total physical or mental impairment that has lasted or is expected to last |
||||||
|
6 months. |
|
|
|
|||
|
4. PRIMARY DIAGNOSIS IS ALCOHOLISM OR CONTROLLED SUBSTANCE ADDICTION |
||||||
|
Checking this box means there is no other physical or mental disability(ies) that precludes this person from |
||||||
|
working other than his/her alcohol or controlled substance addiction. (If this box is checked, the individual |
||||||
|
will be offered treatment through ADAD and will be expected to work once treatment is complete.) |
||||||
If this is a Medical |
|||||||
Yes No |
Has there been improvement in this client’s physical/mental condition that would allow the client to return to work? |
||||||
|
|
|
|
||||
This form may be completed by the following: (Please check one) |
PRINTED NAME, ADDRESS, AND PHONE NUMBER. |
||||||
Examining physician |
Physician assistant certified in Colo. |
This is needed to insure the accuracy of this report |
|||||
Psychiatrist |
|
|
Advanced practice nurse |
|
|
|
|
Registered nurse licensed in Colorado |
|
|
|
||||
|
|
|
|
|
|
|
|
SIGNATURE: |
|
|
|
STATE |
LICENSE # |
DATE OF EXAM |
|
|
|
|
|
|
|
|
|
PLEASE COMPLETE BOTH SIDES |
Section 3
Applicant
Applicant Complete this yellow section before your medical exam:
Highest Grade Completed:Your age:
Type of formal job training:
Explanation of disability or, if this is a redetermination, explain your progress since last medical examination:
Section 4
Section 5
Supervisor |
|
The physical/mental impairment (Box 2, Section 2 above) and other factors such as: |
|
Signature of County Eligibility |
|
|
||||
|
County must complete the Residual Functional Capacity Scoring Matrix below and |
|
|
|
||||||
|
|
Age, Training, Experience, or Education would render the person totally disabled from |
|
|
|
|
|
|||
|
|
having any employment that exists in the community for which they have competence. |
|
|
|
|
|
|||
|
|
document limitations in the case comments. |
|
|
|
Supervisor/Supervisor Designee |
(Date) |
|
||
|
|
|
|
|
|
|
|
|
||
|
|
|
RESIDUAL FUNCTIONAL CAPACITY SCORING MATRIX |
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Score Zero (0) |
Score One (1) |
Score Two (2) |
|
Score Three (3) |
Points |
||
|
|
|
Points |
Point |
Points |
|
Points |
|||
|
|
|
|
|
|
|||||
|
|
Age (in years) |
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Education |
GED, high school |
7th through 11th |
6th grade or less |
Illiterate |
|
|
||
|
|
diploma, or higher |
grade |
|
|
|||||
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
Communication Barriers |
None |
Mild |
Moderate |
|
Severe or Non- |
|
|
|
|
|
|
English Speaking |
|
|
|||||
Above |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Previous Work History |
Skilled |
Unskilled |
|
None |
|
|
|||
Marked |
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
Limitations Related to the |
|
|
|
|
|
|
|
|
|
2 is |
|
|
|
|
|
|
|
|
|
|
|
Ability to: |
|
|
|
|
|
|
|
|
|
Boxif |
|
● Remember, |
None |
Mild |
Moderate |
|
Severe |
|
|
|
Department |
|
● Understand, |
|
|
|
|||||
|
● Carry Out Instructions |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Limitations related to the |
|
|
|
|
|
|
|
|
County |
|
Ability to: |
|
|
|
|
|
|
|
|
|
● Use Judgment, |
|
|
|
|
|
|
|
|
|
|
● Concentrate, or |
None |
Mild |
Moderate |
|
Severe |
|
|
||
the |
|
● Respond Appropriately |
|
|
|
|
|
|
|
|
by |
|
in a Work |
|
|
|
|
|
|
|
|
Completed |
|
Environment |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Medical disability results |
|
Disabled six (6) |
Disabled six (6) |
Disabled twelve |
|
|
||
|
|
as reported on medical |
|
(12) months or |
|
|
||||
|
|
Disabled less than |
months or longer but |
months or longer but |
|
|
||||
|
|
certification form, a |
longer but able to |
|
|
|||||
|
|
six (6) months. |
able to work in some |
able to work in some |
|
|
||||
|
|
Medicaid disability |
work in some type |
|
|
|||||
|
|
The client is |
type of employment. |
type of employment. |
|
|
||||
|
|
determination, or other |
of employment. |
|
|
|||||
|
|
ineligible for AND- |
Physical exertion |
Physical exertion |
|
|
||||
|
|
medical evidence |
Physical exertion |
|
|
|||||
|
|
SO. |
limited to sedentary, |
limited to light or |
|
|
||||
|
|
obtained by the county |
limited to light or |
|
|
|||||
|
|
|
light, or moderate. |
sedentary. |
|
|
|
|||
|
|
department |
|
|
sedentary. |
|
|
|||
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
TOTAL RESIDUAL FUNCTIONAL CAPACITY SCORE (maximum points possible = 21)
PLEASE COMPLETE BOTH SIDES |
Form Characteristics
| Fact Name | Description |
|---|---|
| Form Purpose | The Med 9 form is used to assess medical eligibility for the Aid to the Needy Disabled (AND) program in Colorado. |
| Governing Laws | The form operates under Colorado state law, specifically governing benefits for disabled residents. |
| Completion Responsibility | Medical personnel are responsible for completing the red section of the form, Section 2. |
| Eligibility Criteria | To qualify, an individual must be totally and permanently disabled, unable to perform any job due to a physical or mental impairment lasting 12 months or more. |
| Diagnosis Options | The form includes various categories of disabilities such as respiratory, cardiovascular, neurological, and mental disorders. |
| Partial Disability Assessment | It is possible for a person to be found partially disabled, allowing for a review of conditions preventing employment. |
| Medial Re-examination | If the form is a medical re-examination, it includes a section to assess any improvements in the client’s condition. |
| Residual Functional Capacity | The form requires an assessment of the individual's residual functional capacity to determine employability. |
Guidelines on Utilizing Med 9
Completing the Med 9 form requires attention to detail and accuracy to ensure eligibility for important assistance programs. By following these steps, you will be able to fill out the form correctly, allowing for a smooth review process by the relevant authorities. Make sure to gather all necessary information and consult with medical professionals if needed.
- Begin by filling in your personal information in Section 1. This includes your name (last, first, middle), Social Security Number, date of birth, address, city, state, zip code, client telephone number, the printed name of your county representative, and their contact number or fax.
- Proceed to Section 2, where a medical professional must indicate the disability status. They will check one of the four options regarding the nature and extent of your disability. Make sure they provide the relevant details and select the specific qualifying disability if applicable.
- If the medical examiner selects option 1, they need to specify which qualifying disability applies. They should also complete the information regarding any physical limitations.
- Should options 2 or 3 be checked, note that the medical examiner is responsible for detailing any physical or mental impairments limiting usual occupation activities and the duration of these conditions.
- If option 4 is chosen, ensure clarity on alcoholism or controlled substance addiction being the primary diagnosis and confirm that no other disabilities exist.
- Section 3 requires you, the applicant, to fill in personal information, including your highest grade completed, age, formal job training, and an explanation of your disability or progress if this is a redetermination.
- Once completed, the County representative needs to finalize Section 5. They will assess your Residual Functional Capacity and document this assessment in the scoring matrix provided.
- Finally, add the signature of the medical examiner and their state license number, along with the date of the examination. Verify that both sides of the form are filled out completely.
What You Should Know About This Form
What is the Med 9 form, and who uses it?
The Med 9 form is a crucial piece used by the Colorado Department of Human Services. It's specifically designed for the Aid to the Needy Disabled (AND) program. This program provides financial assistance to residents of Colorado who are disabled. County Departments of Human Services rely on the Med 9 form to evaluate medical eligibility. Medical professionals complete the red section to determine an individual's physical or mental impairments and their ability to work.
How does a medical examiner complete the Med 9 form?
A medical examiner must carefully fill out Section 2 of the Med 9 form. This section includes a series of checked boxes that indicate the level of disability and the specific impairments present. The examiner must assess whether the individual is totally and permanently disabled or if they can engage in their usual occupation under certain limitations. Additionally, they must specify the qualifying disability from a list that includes various disorders, such as respiratory or cardiovascular issues. Accurate completion of this section is vital as it directly impacts the client's eligibility for benefits.
What information does the applicant need to provide?
Before their medical examination, the applicant is responsible for filling out the yellow section of the Med 9 form. They need to provide personal information, including their highest grade completed and age, along with any formal job training they may have received. Most importantly, the applicant must explain their disability or detail any progress made since the last evaluation. This information helps medical personnel gain a complete understanding of the applicant's situation.
What should I expect after submitting the Med 9 form?
After submitting the completed Med 9 form, the county agency will review the information provided. They will evaluate the medical details and the applicant's personal statements for accuracy and completeness. Depending on the findings, the county may approve or deny the application for the Aid to the Needy Disabled (AND) program. If approved, financial assistance will be arranged. However, if there are questions or concerns about the application, the county may reach out for additional information or clarification.
Common mistakes
Filling out the Med 9 form can be a bit daunting, and it's easy to make mistakes. One common error is not providing complete information. Individuals often skip filling out crucial fields like social security numbers or addresses. Omitting these details can delay processing as the county departments may need to reach out for additional information.
Another mistake frequently observed is failing to communicate clearly about the disability. When individuals do not adequately describe their condition or its impact on their daily lives, it can hinder the evaluation process. It's important to provide a comprehensive explanation of how the disability affects daily activities to help assess eligibility accurately.
People also sometimes mischeck the boxes related to their disabilities. This error could mean selecting a box that does not accurately reflect the individual’s condition. Misclassification can lead to incorrect assessments, affecting the approval for benefits. Always double-check which boxes are checked before submitting the form.
Some applicants neglect to complete the yellow section of the form before the medical exam. This section asks for important details about education, job training, and an explanation of the disability. Skipping this can create more work for medical personnel as they rely on this information for a complete evaluation.
It’s not uncommon for individuals to overlook the expiration of their medical certifications. When the form is submitted with outdated information, the approval process can stall. Ensure that any medical information or certifications attached to the form are current.
A third mistake people make is forgetting to have a qualified medical professional sign the form. This signature is essential for the verification of the medical information provided. Without it, the form may be deemed incomplete, further delaying acceptance into the program.
Lastly, individuals sometimes submit the form without understanding their rights regarding the process. Familiarizing oneself with how the process works can provide better insight into what to expect. Knowing this can foster a sense of empowerment during what can be a challenging time.
Documents used along the form
When applying for the Aid to the Needy Disabled (AND) program in Colorado, the Med 9 form serves as a vital tool in assessing medical eligibility. However, several other forms and documents complement the Med 9 form. Understanding each of these can streamline the application process and ensure that necessary information is available for a thorough evaluation.
- Application for Aid to the Needy Disabled (AND) Form: This form initiates the application process for the AND program, capturing essential personal and financial information of the individual applying for assistance.
- Verification of Income Form: Used to verify the income of the applicant, this document includes information on wages, benefits, and other sources of income. Proper completion is necessary to assess financial eligibility for the program.
- Medicaid Application: A separate application that determines eligibility for Medicaid benefits. Since AND recipients often also require Medicaid, this form can facilitate access to additional health benefits.
- Medical Records Release Form: This allows designated medical professionals to share pertinent health information with the county department. It ensures that details can be obtained directly from healthcare providers to support the applicant's case.
- Physician's Statement: A detailed letter or form completed by a physician which outlines the individual's medical condition, treatments, and limitations. This document often provides the necessary evidence to support claims of disability.
- Social Security Administration (SSA) Disability Determination: If the individual has applied for Social Security Disability Insurance (SSDI) or Supplemental Security Income (SSI), the determination of the SSA can provide critical documentation concerning their disability status.
- Medication List: A comprehensive list of medications the applicant is currently taking. This document can provide insight into the severity of the individual’s medical issues and how they impact daily functioning.
- Worker’s Compensation Documentation: If applicable, this paperwork relates to any claims made concerning employment-related injuries. It can include forms detailing the nature of the injuries and ongoing treatment plans.
- Personal Statement: This informal document gives the applicant a chance to describe their condition, the impact it has on their daily life, and any other relevant circumstances. Personal narratives can be incredibly compelling in disability assessments.
By familiarizing yourself with these additional forms, you can better navigate the process of applying for the AND program. Remember, each document plays a specific role in providing a comprehensive view of an applicant's eligibility and needs.
Similar forms
The Med 9 form is used to determine medical eligibility for the Aid to the Needy Disabled (AND) program in Colorado. Several other forms bear similarities to the Med 9 in purpose and function. Here’s a breakdown of those forms:
- Social Security Administration (SSA) Disability Report: This form collects information about a person's medical conditions to assess eligibility for Social Security Disability Insurance (SSDI) or Supplemental Security Income (SSI). Like the Med 9, it requires detailed medical documentation and personal information.
- State Medicaid Application Form: This application is used to evaluate eligibility for Medicaid benefits. It involves a review of medical conditions and financial status, similar to how the Med 9 assesses both elements for AND eligibility.
- Long-Term Disability (LTD) Claim Form: Individuals seeking long-term disability benefits must complete this form to demonstrate how their medical conditions prevent them from working. Similar to the Med 9, it requires supporting medical evidence and personal information.
- Veterans Affairs (VA) Disability Compensation Application: Veterans applying for disability benefits must submit this application, which also evaluates medical conditions. Like the Med 9, it seeks detailed documentation of disabilities and functional limitations.
- Worker's Compensation Claim Form: When workers are injured on the job, they need to complete this form to claim benefits. The evaluation process is akin to the Med 9, as both establish the impact of a disability on the individual’s ability to work.
- Functional Capacity Evaluation (FCE): This assessment reviews an individual’s physical and mental abilities to perform work-related tasks. It shares the common goal of determining the extent of a disability with the Med 9.
- Personal Care Service Application: Used to assess one’s eligibility for personal care services, this application evaluates the extent of the individual’s physical or cognitive limitations, similar to the assessments performed in the Med 9.
- Supplemental Nutrition Assistance Program (SNAP) Medical Deduction Form: This form allows individuals to report medical expenses to receive deductions in their SNAP benefits. It assesses medical conditions affecting households, paralleling how the Med 9 assesses disability impacts.
Each of these documents serves a specific purpose while requiring thorough medical and personal details to evaluate an individual’s eligibility for various assistance programs.
Dos and Don'ts
When filling out the Med 9 form, consider the following important guidelines:
- Provide Accurate Information: Ensure that all details, including personal information and medical history, are correct. Mistakes or omissions can delay processing.
- Be Clear on Disability: When selecting the qualifying disability, provide a clear explanation or definition if necessary. This assists in the proper assessment of eligibility.
- Consult Medical Personnel: Have a qualified medical professional complete Section 2. Their input is crucial for determining eligibility for the Aid to the Needy Disabled program.
- Keep Copies: Retain a copy of the completed form for your records. This helps track the submission and any follow-up required.
- Avoid Incomplete Sections: Do not leave any required fields blank. Every section must be addressed to avoid processing issues.
- Avoid Generalizations: Be specific about disabilities and limitations. Vague descriptions can result in misunderstandings and may affect eligibility.
- Skip Legal Jargon: Use clear language that is easily understood. Avoid terms that might confuse the reader.
- Do Not Rush: Take your time to ensure that every section is filled out carefully. Rushed submissions often contain errors.
Misconceptions
Misconceptions about the Med 9 form can lead to confusion and incorrect assumptions regarding its purpose and use. Below is a list of seven common misconceptions, along with clarifying explanations.
-
The Med 9 form is only for individuals with severe disabilities.
In reality, the Med 9 form is intended for individuals with a range of disabilities, not just severe cases. It includes options for those who may have temporary impairments or conditions that make it difficult to engage in usual work but do not necessarily constitute total disability.
-
Once the Med 9 form is submitted, the application process is complete.
This is a misconception. The form must be reviewed and processed by the County Department of Human Services. Additional information may be required, and applicants may need to attend further evaluations or assessments.
-
Only medical professionals can complete the Medical section of the Med 9 form.
While it is true that medical personnel must fill out Section 2, applicants complete the yellow section before their medical exam. This collaborative approach ensures that accurate and comprehensive information is available.
-
The Med 9 form guarantees approval for benefits.
Completion of the Med 9 form does not guarantee that an individual will be approved for benefits. The decision is based on a comprehensive evaluation of the provided information and how it meets the program's criteria.
-
Alcoholism or substance addiction automatically disqualifies someone from receiving benefits.
This is misleading. While alcoholism or controlled substance addiction can complicate an application, the Med 9 form allows for treatment options. If these conditions are the only impairments, individuals may be offered treatment and expected to seek employment afterward.
-
The Med 9 form process is quick and straightforward.
In practice, the process may take time. Factors such as the complexity of a person’s medical condition and the completeness of the submitted information can influence how long the evaluation takes.
-
Filling out the Med 9 form is the final step in applying for assistance.
This is not correct. After submitting the Med 9 form, additional follow-up may be required. Applicants should remain engaged and responsive to any requests from the County for further information or documentation.
Key takeaways
When filling out and utilizing the Med 9 form, several important considerations should be kept in mind to ensure accuracy and prevent delays in processing applications for the Aid to the Needy Disabled (AND) program.
- The Med 9 form consists of multiple sections, each serving a specific purpose. Medical personnel must pay close attention to Section 2, as it addresses crucial medical determinations regarding an applicant's disability status.
- This form must be completed accurately. Providing detailed information, especially in the “Qualifying Disability” section, can significantly affect the outcome of the disability assessment. Each checkbox corresponds to different categories of disabilities; ensuring that the relevant options are carefully checked is essential.
- It is vital for the applicant to complete Section 3 before the medical exam. This section includes pertinent personal information and an explanation of the applicant's disability. This context can aid medical personnel in making informed decisions.
- If the individual applying has undergone a medical re-examination, the questions related to improvement in the client’s condition must be addressed. This ensures the evaluation reflects any changes in the applicant's health status since the last review.
- County representatives must be meticulous when filling out Section 5, which involves the Residual Functional Capacity Scoring Matrix. Evaluating factors such as age, education, and previous work history can influence whether an applicant is deemed eligible for benefits.
Meticulous attention to detail when completing each section of the Med 9 form can improve the accuracy of the assessment and expedite the benefits approval process.
Browse Other Templates
Qualification Certificate,Professional Certification Document,Authority Verification Form,Certification Record,Standards Compliance Certificate,Qualification Verification Form,Credentialing Document,Certification of Expertise,Professional Validation - Conveys official recognition of professional qualifications.
Multiplication Worksheets 0 12 - Helps identify areas needing improvement in multiplication skills.
Illinois State Llc Filing Fee - Clarity and correctness in form submission contribute to a smoother approval process.