Fill Out Your Medicaid Standing Order Form
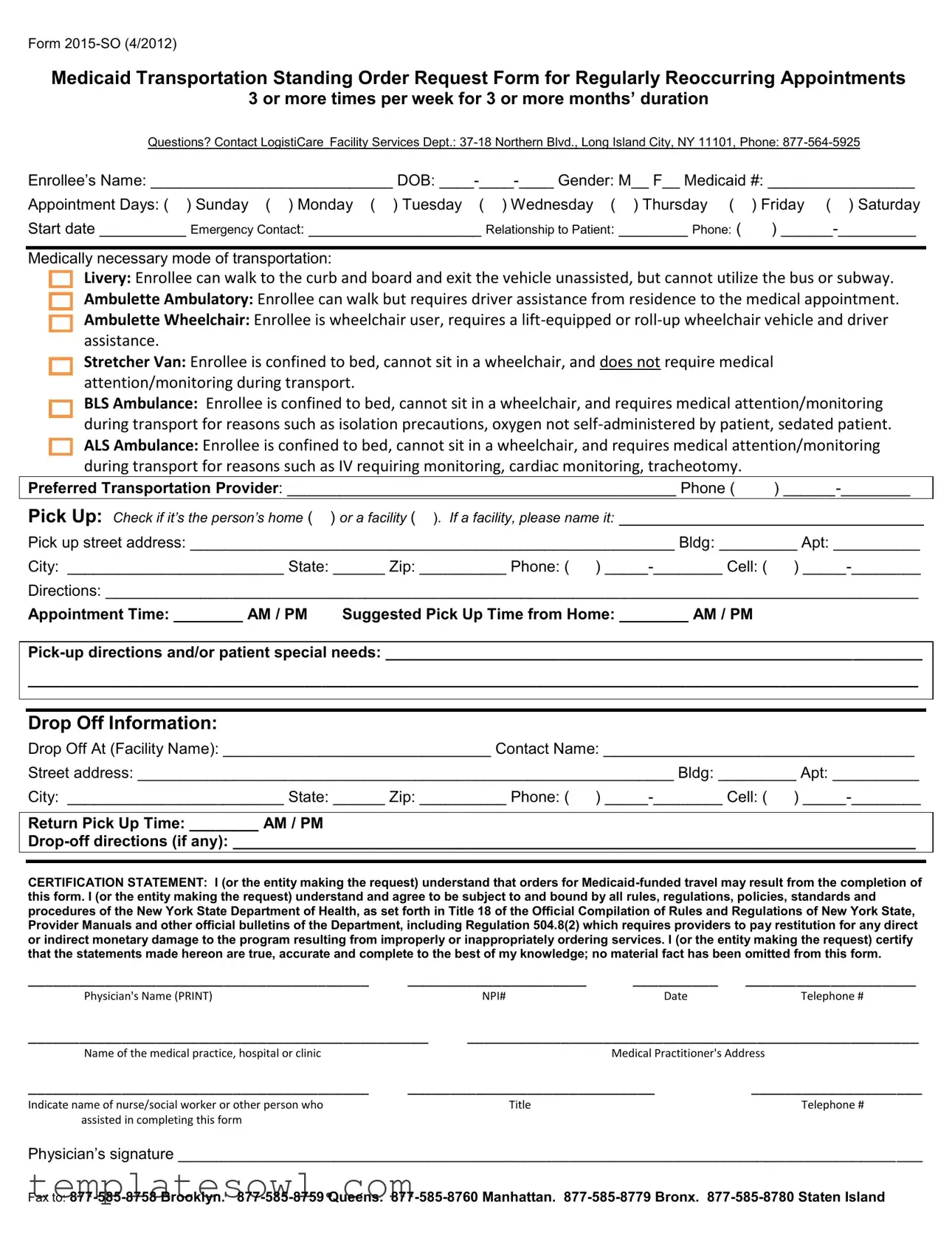
The Medicaid Standing Order form, specifically Form 2015-SO (4/2012), is essential for individuals requiring consistent transportation to medical appointments. This form caters to those who have appointments three or more times a week over an extended duration of three months or more. It facilitates access to various transportation modes, accommodating different levels of mobility and medical needs. Notably, it includes options for livery, ambulette, stretcher van, and various ambulance types, ensuring that every patient finds suitable transportation for their unique circumstances. The form requires detailed information such as the enrollee’s name, date of birth, Medicaid number, and emergency contact details. It also prompts for specific appointment information, including the exact days and times as well as the preferred transportation provider. Crucially, individuals must certify the accuracy of the information provided, acknowledging understanding of the relevant regulations related to Medicaid-funded travel. For assistance with the form or to address any questions, those in need can reach out to LogistiCare Facility Services. Completing this form with care allows for timely and appropriate transportation to necessary medical services, thereby supporting the overall well-being of those reliant on these arrangements.
Medicaid Standing Order Example
Form
Medicaid Transportation Standing Order Request Form for Regularly Reoccurring Appointments
3 or more times per week for 3 or more months’ duration
Questions? Contact LogistiCare Facility Services Dept.:
Enrollee’s Name: ____________________________ DOB:
Appointment Days: ( ) Sunday ( ) Monday ( ) Tuesday ( ) Wednesday ( |
) Thursday ( |
) Friday ( ) Saturday |
Start date __________ Emergency Contact: ____________________ Relationship to Patient: |
________ Phone: ( |
) |
Medically necessary mode of transportation:
Livery: Enrollee can walk to the curb and board and exit the vehicle unassisted, but cannot utilize the bus or subway.
Ambulette Ambulatory: Enrollee can walk but requires driver assistance from residence to the medical appointment.
Ambulette Wheelchair: Enrollee is wheelchair user, requires a
Stretcher Van: Enrollee is confined to bed, cannot sit in a wheelchair, and does not require medical attention/monitoring during transport.
BLS Ambulance: Enrollee is confined to bed, cannot sit in a wheelchair, and requires medical attention/monitoring during transport for reasons such as isolation precautions, oxygen not
Preferred Transportation Provider: _____________________________________________ Phone ( )
Pick Up: Check if it’s the person’s home ( ) or a facility ( ). If a facility, please name it: ________________________________
Pick up street address: ________________________________________________________ Bldg: _________ Apt: __________
City: _________________________ State: ______ Zip: __________ Phone: ( )
Directions: ______________________________________________________________________________________________
Appointment Time: ________ AM / PM Suggested Pick Up Time from Home: ________ AM / PM
_______________________________________________________________________________________________________
Drop Off Information:
Drop Off At (Facility Name): _______________________________ Contact Name: ____________________________________
Street address: ______________________________________________________________ Bldg: _________ Apt: __________
City: _________________________ State: ______ Zip: __________ Phone: ( )
Return Pick Up Time: ________ AM / PM
CERTIFICATION STATEMENT: I (or the entity making the request) understand that orders for
________________________________________ |
_____________________ |
__________ |
____________________ |
|
Physician's Name (PRINT) |
|
NPI# |
Date |
Telephone # |
_______________________________________________ |
_____________________________________________________ |
|||
Name of the medical practice, hospital or clinic |
|
|
Medical Practitioner's Address |
|
________________________________________ |
_____________________________ |
____________________ |
||
Indicate name of nurse/social worker or other person who |
|
Title |
|
Telephone # |
assisted in completing this form |
|
|
|
|
Physician’s signature ______________________________________________________________________________________
Fax to:
Form Characteristics
| Fact Name | Description |
|---|---|
| Form Identifier | The Medicaid Transportation Standing Order Request Form is labeled as Form 2015-SO (4/2012). |
| Purpose | This form is used for requesting Medicaid-funded transportation for regularly recurring medical appointments, specifically for individuals needing transport three or more times per week for a minimum of three months. |
| Contact Information | For inquiries, users can contact LogistiCare Facility Services Department at 877-564-5925, located at 37-18 Northern Blvd., Long Island City, NY 11101. |
| Transportation Modes | Various medically necessary transportation options include livery, ambulette (both ambulatory and wheelchair), stretcher van, BLS ambulance, and ALS ambulance. |
| Certification Requirement | The individual or entity making the request must certify that the information provided is accurate and agrees to comply with all relevant regulations, including New York State Department of Health policies. |
| Relevant Law | This form operates under New York State regulations, specifically Title 18 of the Official Compilation of Rules and Regulations, including Regulation 504.8(2) which deals with restitution for improper service orders. |
| Submission | The completed form should be faxed to the appropriate borough-specific LogistiCare numbers, as provided on the form. |
Guidelines on Utilizing Medicaid Standing Order
Completing the Medicaid Standing Order form requires accurate information to ensure that transportation is arranged properly for recurring medical appointments. After filling out the form, it must be submitted to the relevant medical or transportation provider for processing.
- Enter the enrollee's full name in the appropriate space.
- Provide the date of birth in the format of year-month-day.
- Select the gender by marking the appropriate box.
- Fill in the Medicaid number of the enrollee.
- Choose the appointment days by checking the corresponding boxes for Sunday through Saturday.
- Write the start date for transportation services.
- Fill in the emergency contact's name, relationship to the patient, and phone number.
- Select the medically necessary mode of transportation by checking the appropriate option: Livery, Ambulette Ambulatory, Ambulette Wheelchair, Stretcher Van, BLS Ambulance, or ALS Ambulance.
- Enter the preferred transportation provider’s name and phone number.
- Indicate the pick-up location by checking whether it is at home or a facility and provide the facility name if applicable.
- Fill in the pick-up street address, including building, apartment, city, state, and zip code.
- Record any additional phone or cell numbers for contact during pick-up.
- Provide specific directions for the pick-up if necessary.
- Fill in the appointment time and the suggested pick-up time from home.
- Detail any patient special needs or additional instructions.
- Enter the drop-off facility name and contact name for arrival verification.
- Provide the street address of the drop-off location, including building, apartment, city, state, and zip code.
- Fill in the return pick-up time and any special drop-off directions if needed.
- Complete the certification statement by entering the physician’s name, NPI number, date, and telephone number.
- Enter the name of the medical practice, hospital, or clinic.
- Provide the address of the medical practitioner.
- Indicate the name and title of the person who assisted in completing the form.
- Obtain the physician's signature for the certification statement.
- Fax the completed form to the appropriate number based on the location of service: Brooklyn, Queens, Manhattan, Bronx, or Staten Island.
What You Should Know About This Form
What is the Medicaid Transportation Standing Order form?
The Medicaid Transportation Standing Order form, also known as Form 2015-SO, is used to request transportation for individuals who have regularly scheduled medical appointments. It applies to those needing transportation three or more times each week for a duration of at least three months. This form helps ensure that eligible individuals can access necessary medical care with the proper mode of transportation.
Who should fill out the form?
The form should be filled out by someone who can provide accurate information about the enrollee, which may be the patient themselves, a family member, or a healthcare professional. It’s important that all sections are completed to ensure the enrollee receives the correct transportation assistance based on their medical needs.
What types of transportation can be requested?
There are several medically necessary modes of transportation included in the form. These range from livery services for those who can walk to ambulatory transport for those needing assistance. For patients who are wheelchair users, a lift-equipped vehicle can be requested. If the patient is confined to bed and needs medical attention during transport, options such as BLS and ALS ambulances are available. Each option is tailored to meet specific medical requirements.
How can I ensure my information is correct on the form?
Double-checking all details before submitting the form is essential. Verify the enrollee's information, such as name, date of birth, Medicaid number, and transportation needs. Make sure the appointment days and times are accurate. Also, confirm that the preferred provider's contact details are correct. Accurate information will help avoid delays in securing transport.
What should I do if I have questions about the form?
If you have questions, you can contact the LogistiCare Facility Services Department. They are available at their office located at 37-18 Northern Blvd., Long Island City, NY 11101, or you can call them at 877-564-5925. They can provide guidance and answer any questions related to completing the form or transportation services.
How is the form submitted?
Once the form is completed, it should be faxed to the appropriate number based on the enrollee's location. For example, if the enrollee is in Brooklyn, fax to 877-585-8758. Make sure to keep a copy of the completed form for your records as well.
Common mistakes
Filling out the Medicaid Transportation Standing Order Request Form can seem straightforward, yet numerous mistakes frequently occur. The first mistake is not providing complete and accurate personal information. When applicants leave fields blank or enter incorrect data, it can delay the approval process. Ensuring that the enrollee's name, date of birth, and Medicaid number are correct is essential.
Another common error involves the selection of appointment days. Individuals sometimes check multiple days or fail to indicate all relevant days. This oversight can create confusion for transportation providers and complicate scheduling. It is crucial to clearly mark all days for transportation.
Many people misunderstand the medically necessary mode of transportation section. Choosing the wrong mode can have significant implications. For instance, selecting "Ambulette" when a "BLS Ambulance" is needed could result in inadequate transport for the patient’s condition. Readers must carefully review the definitions before making a selection.
People also often forget to fill out emergency contact information. Leaving this blank can impede communication in case of an issue during transport. Ensuring that a reliable contact person is listed helps streamline processes should something unexpected occur.
The address section can be especially prone to mistakes. Missing details like apartment numbers or incorrect street names can cause delays or missed pickups entirely. To mitigate these risks, it’s vital to double-check the entire address before submitting the form.
Some applicants do not specify the pick-up location clearly. Indicating whether the pick-up point is a home or facility is crucial, along with naming the facility if applicable. Vague descriptions can lead to confusion or miscommunication with transport providers.
Failing to provide appropriate times for appointments and suggested pick-up can disrupt the entire scheduling process. Always specify the appointment time and suggest a pick-up time to ensure accuracy. This detail enriches the form and aids the transportation provider.
Returning pick-up details are often overlooked as well. Not including this information can be problematic. Clearly stating return times helps ensure that transportation can be arranged effectively.
Finally, individuals sometimes neglect their certification statement. This section is critical, as it confirms that the information provided is true and complete. Omitting signatures or dates here may lead to delays or denials of transportation services. Always ensure that these responsibilities are fulfilled completely.
Documents used along the form
When navigating the processes associated with Medicaid transportation, several important forms often accompany the Medicaid Standing Order form. Understanding these documents can help streamline the request and approval process. Below is a list of some commonly used documents:
- Medicaid Application Form: This form is used by individuals to apply for Medicaid benefits. It collects important information about the applicant's income, household size, and medical needs, helping determine eligibility.
- Prior Authorization Request: Before certain services can be covered, this document may be needed to obtain approval from Medicaid. It provides details on the requested service and justifies the medical necessity.
- Physician's Order Form: A doctor's written directive that specifies the need for a particular medical service or treatment. This form helps ensure that services are medically necessary and aligns with Medicaid guidelines.
- Patient Transport Request Form: Similar to the Standing Order form, this document is specifically for scheduling one-off or non-recurring medical transportation. It includes crucial details about the patient and the nature of the transport needed.
- Emergency Contact Form: This form provides crucial information about who should be contacted in case of emergencies. It typically includes contact names, relationships, and phone numbers.
- Service Provider Agreement: A contract between the Medicaid recipient and the transportation provider. It outlines the services provided, rates, and expectations for both parties.
- Patient Information Form: This document collects comprehensive information about the patient’s medical history and current health status, which can be essential for transportation and care planning.
- Medicaid Review Form: Periodically, Medicaid requires a review of a recipient’s eligibility. This form helps to ensure the recipient continues to meet the requirements for necessary services.
By being familiar with these forms, individuals can navigate the Medicaid transportation system more effectively. Gathering the necessary documents can reduce delays and ensure that essential services are provided without unnecessary obstacles.
Similar forms
Medicaid Prior Authorization Form: This document requests approval for medical services before they are provided. Like the Medicaid Standing Order, it outlines specific medical needs and justifies the necessity of services based on patient conditions.
Medicaid Transportation Request Form: Similar to the Standing Order, this form is specifically used to request transport services under Medicaid. It includes details about the patient's needs and the required mode of transportation.
Medicaid Application for Benefits: This application collects information to determine eligibility for Medicaid and encompasses healthcare needs. Both documents have a focus on patient care and essential services.
Medicaid Managed Care Enrollment Form: This form initiates enrollment in a Medicaid managed care program. It includes personal and health information, much like the Standing Order document, to ensure appropriate service allocation.
Patient Referral Form: This is used to direct patients to specialists or specific services. It describes medical necessity and coordinates care. Thus, it shares a common goal with the Standing Order of facilitating access to healthcare.
Medical Necessity Letter: This letter outlines the need for specific medical services. It informs insurers, including Medicaid, about the patient's conditions and requests necessary authorizations, paralleling the intent of the Medicaid Standing Order.
Dos and Don'ts
When filling out the Medicaid Standing Order form, certain practices can help in ensuring a smooth process. Here are some important dos and don’ts to consider:
- Do provide accurate personal information for the enrollee, such as name, date of birth, and Medicaid number.
- Do clearly indicate all necessary details about the type of transportation required.
- Do specify the appointment and pick-up times to avoid any scheduling conflicts.
- Do ensure you have the correct contact information for emergency contacts and transportation providers.
- Don't leave any sections of the form blank unless instructed.
- Don't provide misleading or incorrect information about the enrollee’s condition or transportation needs.
- Don't forget to have the physician sign the form before submission.
- Don't submit the form without reviewing it for completeness and accuracy.
Misconceptions
Misconceptions about the Medicaid Standing Order form can lead to confusion and potential issues in accessing services. Below is a list of common misunderstandings along with clarifications.
- The form is only for emergency situations. The Medicaid Standing Order form is intended for regularly recurring appointments, not just emergencies. It can be used when transportation is needed consistently over a period of time.
- Completing the form guarantees transportation. While the form initiates the request for transportation, approval is subject to the policies of the Medicaid program and availability. A completed form does not automatically secure a ride.
- Any mode of transportation can be requested. The form specifies medically necessary modes of transportation. Options include livery, ambulette, stretcher van, and ambulance, based on the enrollee’s specific needs.
- All types of transportation are covered equally. Different modes of transportation come with varied eligibility criteria. Understanding the enrollee’s medical condition determines the appropriate option.
- The enrollee must provide all details themselves. Assistance can be provided when completing the form. Family members, medical providers, or social workers may help ensure the form is filled out accurately.
- The enrollee's emergency contact is not necessary. Including an emergency contact serves as a safeguard. Should any issues arise during transportation, having a reliable contact can be crucial.
- Transportation needs do not change over time. Individuals' medical conditions can evolve. Regularly assessing and updating the form ensures that the appropriate transportation type is always utilized.
- Submitting the form is the responsibility of the enrollee only. It is often a shared responsibility. Physicians or facilities requesting transportation on behalf of the enrollee also play a vital role in submitting the form correctly.
- The form is only applicable in specific locations. While this form is part of New York’s Medicaid program, similar requirements may exist in other states. However, distinct procedures may apply depending on local regulations.
Understanding these misconceptions can facilitate smoother interactions with the Medicaid system. It is essential to have clear information and support when navigating healthcare transportation needs.
Key takeaways
- Understand the Purpose: The Medicaid Standing Order form is used for requesting transportation to medical appointments on a regular basis, specifically three or more times a week for three months or longer.
- Gather Necessary Information: Ensure all personal details of the enrollee are accurately filled out, including name, date of birth, and Medicaid number.
- Select Appointment Days: Clearly mark the specific days of the week the transportation is needed.
- Choose the Right Transportation: Indicate the medically necessary mode of transportation based on the enrollee's mobility needs.
- Specify Pickup and Drop-off Locations: Provide accurate addresses for both the pickup location and the medical appointment destination to avoid confusion.
- Detail Special Needs: Include any special requirements or directions that may assist the driver or transporter during appointments.
- Certification Statement: A signed statement certifying the truthfulness of the information must be included, as it holds accountability for the accuracy of the request.
- Know Where to Send the Form: Fax the completed form to the correct number based on the enrollee's borough to ensure timely processing.
Browse Other Templates
Termite Inspection Arizona - The form guides both inspectors and property owners toward effective pest control solutions.
Nyc Corp Tax Rate - Filing this form is essential for corporations seeking additional time to prepare their tax documents.
Cash Withdrawal Slip Fill Up - The Chase Withdrawal Slips form is designed for secure financial transactions.