Fill Out Your Medical Choice Form
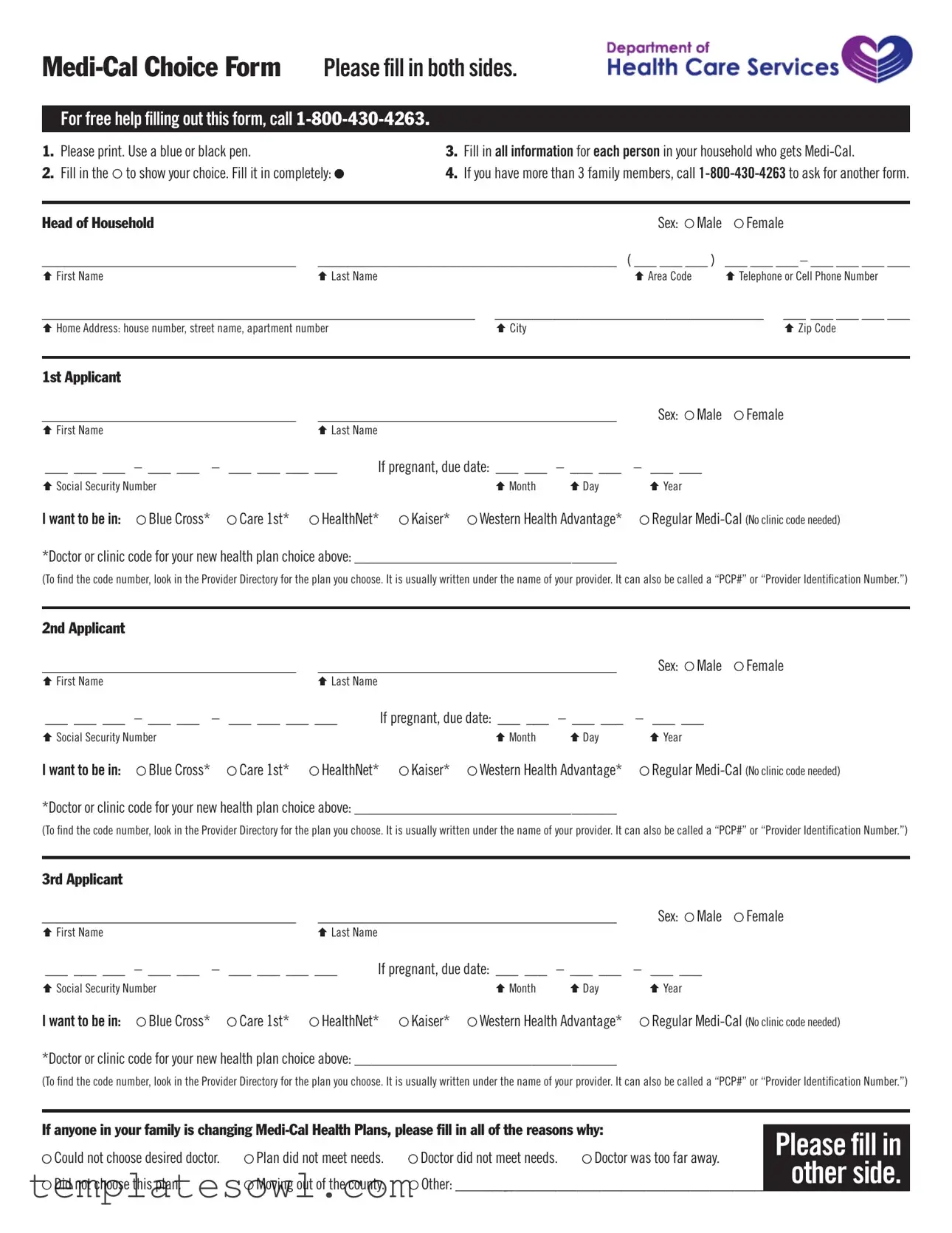
The Medical Choice Form is an essential document for individuals and families enrolled in Medi-Cal, California's Medicaid program. This form allows participants to make informed decisions about their healthcare options, enabling them to select a health plan that best fits their needs. When filling it out, be sure to print clearly and use either a blue or black pen. The form requires details for each member of your household who receives Medi-Cal benefits, including names, social security numbers, and preferences for specific health plans like Blue Cross, HealthNet, or Kaiser. If you have more than three applicants, you should call for an additional form to ensure everyone is included. Not only does the form seek your health plan preference, but it also asks for reasons if anyone in your family is changing plans. Understanding your choices is crucial; thus, the form contains a statement of understanding that outlines what it means to select a Medi-Cal Health Plan. Additionally, the document requires signatures from the head of the household and, if applicable, from guardians for minors. Completing this form accurately is key to receiving the appropriate healthcare services, and assistance is available via a dedicated helpline.
Medical Choice Example
For free help filling out this form, call
1. Please print. Use a blue or black pen. |
|
|
3. Fill in all information for each person in your household who gets |
|||||||
2. Fill in the |
to show your choice. Fill it in completely: |
|
4. If you have more than 3 family members, call |
|||||||
|
|
|
|
|
|
|
|
|
|
|
Head of Household |
|
|
|
|
|
|
Sex: |
Male |
Female |
|
__________________________________ |
________________________________________ |
( ___ ___ ___ ) ___ ___ ___ – ___ ___ ___ ___ |
||||||||
Ç First Name |
|
|
Ç Last Name |
|
|
|
|
Ç Area Code |
|
Ç Telephone or Cell Phone Number |
__________________________________________________________ |
____________________________________ ___ ___ ___ ___ ___ |
|||||||||
Ç Home Address: house number, street name, apartment number |
|
|
Ç City |
|
|
|
Ç Zip Code |
|||
|
|
|
|
|
|
|
|
|
|
|
1st Applicant |
|
|
|
|
|
|
|
|
|
|
__________________________________ |
________________________________________ |
Sex: |
Male |
Female |
||||||
Ç First Name |
|
|
Ç Last Name |
|
|
|
|
|
|
|
___ ___ ___ |
– ___ ___ – |
___ ___ ___ ___ |
If pregnant, due date: ___ ___ |
– ___ ___ |
– ___ ___ |
|
||||
Ç Social Security Number |
|
|
|
|
Ç Month |
Ç Day |
Ç Year |
|
|
|
I want to be in: |
Blue Cross* |
Care 1st* |
HealthNet* |
Kaiser* |
Western Health Advantage* |
Regular |
||||
*Doctor or clinic code for your new health plan choice above: ___________________________________ |
|
|
|
|||||||
(To find the code number, look in the Provider Directory for the plan you choose. It is usually written under the name of your provider. It can also be called a “PCP#” or “Provider Identification Number.”)
2nd Applicant |
|
|
|
|
|
|
|
|
__________________________________ |
________________________________________ |
Sex: Male |
Female |
|||||
Ç First Name |
|
|
Ç Last Name |
|
|
|
|
|
___ ___ ___ |
– ___ ___ – |
___ ___ ___ ___ |
If pregnant, due date: ___ ___ |
– ___ ___ |
– ___ ___ |
|
||
Ç Social Security Number |
|
|
|
Ç Month |
Ç Day |
Ç Year |
|
|
I want to be in: |
Blue Cross* |
Care 1st* |
HealthNet* |
Kaiser* |
Western Health Advantage* |
Regular |
||
*Doctor or clinic code for your new health plan choice above: ___________________________________ |
|
|
||||||
(To find the code number, look in the Provider Directory for the plan you choose. It is usually written under the name of your provider. It can also be called a “PCP#” or “Provider Identification Number.”)
3rd Applicant |
|
|
|
|
|
|
|
|
|
__________________________________ |
________________________________________ |
Sex: Male |
Female |
||||||
Ç First Name |
|
|
Ç Last Name |
|
|
|
|
|
|
___ ___ ___ |
– ___ ___ – |
___ ___ ___ ___ |
If pregnant, due date: ___ ___ |
– ___ ___ |
– ___ ___ |
|
|||
Ç Social Security Number |
|
|
|
|
Ç Month |
Ç Day |
Ç Year |
|
|
I want to be in: |
Blue Cross* |
Care 1st* |
HealthNet* |
Kaiser* |
Western Health Advantage* |
Regular |
|||
*Doctor or clinic code for your new health plan choice above: ___________________________________
(To find the code number, look in the Provider Directory for the plan you choose. It is usually written under the name of your provider. It can also be called a “PCP#” or “Provider Identification Number.”)
If anyone in your family is changing |
Please fill in |
||||
Could not choose desired doctor. |
Plan did not meet needs. |
Doctor did not meet needs. |
Doctor was too far away. |
||
other side. |
|||||
Did not choose this plan. |
Moving out of the county. |
|
|
||
Other: ______________________________________________________________ |
|||||
For free help filling out this form, call
STATEMENT OF UNDERSTANDING: I understand that by filling out and signing this form, I am choosing how to get my
I understand that the Department of Health Care Services will keep the information on this form. They will only use it to enroll or disenroll me from a
If You Chose a
If You Join Kaiser: I understand that Kaiser requires binding arbitration. This means that I give up my right to a jury or court trial for medical malpractice and other disagreements about benefits and services. Instead, I would help choose independent professionals who would make a decision about the problem. I can still ask for a
Please Sign Below: |
|
|
|
Head of Household |
__________________________________________ |
Date: ___ ___ – ___ ___ |
– ___ ___ |
|
Ç Signature |
Ç Month Ç Day |
Ç Year |
1st Applicant |
|
if under 18 years, parent or guardian: __________________________________________ |
Date: |
ÇSignature
2nd Applicant |
|
if under 18 years, parent or guardian: __________________________________________ |
Date: |
ÇSignature
3rd Applicant |
|
if under 18 years, parent or guardian: __________________________________________ |
Date: |
ÇSignature
___ ___ – ___ ___ |
– ___ ___ |
|
Ç Month |
Ç Day |
Ç Year |
___ ___ – ___ ___ |
– ___ ___ |
|
Ç Month |
Ç Day |
Ç Year |
___ ___ – ___ ___ |
– ___ ___ |
|
Ç Month |
Ç Day |
Ç Year |
Mail To:
California Dept. of Health Services |
|
|
Health Care Options |
|
|
Box 989009 |
|
|
Please fill in |
||
West Sacramento, CA |
||
other side. |
||
________________________________________________________________________________________________________________ |
Form Characteristics
| Fact Name | Details |
|---|---|
| Medi-Cal Choice Form | This form is essential for selecting a Medi-Cal health plan in California. |
| Filling Instructions | Participants need to use a blue or black pen and print all information clearly. |
| Household Information | Complete the form for every member in the household receiving Medi-Cal benefits. |
| Contact Information | For assistance in filling out the form, individuals can call 1-800-430-4263. |
| Health Plan Options | Choices include Blue Cross, Care 1st, HealthNet, Kaiser, and Western Health Advantage. |
| PCP Code Requirement | Applicants must provide a doctor or clinic code for their selected health plan when needed. |
| Statement of Understanding | The signer acknowledges understanding of enrollment and information sharing protocols with the Department of Health Care Services. |
| Arbitration Clause | Choosing Kaiser means agreeing to binding arbitration for disputes rather than proceeding to court. |
| Mailing Address | Completed forms should be sent to the California Department of Health Services in West Sacramento. |
Guidelines on Utilizing Medical Choice
Filling out the Medical Choice form is an important step in securing health care coverage through Medi-Cal. Be ready to provide detailed information for each member of your household who will receive Medi-Cal benefits. Once completed, the form will help streamline your enrollment process.
- Obtain the Medical Choice form. Ensure you have both sides of the form available.
- Use a blue or black pen to fill out the form. Print your responses clearly.
- Start by filling in the information for the Head of Household. Include their first and last name, sex (male or female), telephone number, and home address.
- Indicate the sex and the Social Security Number of the Head of Household. If applicable, note the due date if pregnant.
- Select a health plan option for the Head of Household. Choose from options such as Blue Cross, Care 1st, HealthNet, Kaiser, Western Health Advantage, or Regular Medi-Cal. Also, include the doctor or clinic code if needed.
- Repeat steps 3 to 5 for the 2nd and 3rd applicants in the household. Fill in all relevant details including their name, sex, Social Security Number, and health plan selection.
- If any family member is changing Medi-Cal Health Plans, specify the reasons such as "could not choose desired doctor" or "did not choose this plan" in the designated area.
- Finally, read the Statement of Understanding carefully and sign it. Ensure the date is included next to the signature. If any applicants are under 18, a parent or guardian must sign for them.
- Mail the completed form to the California Department of Health Services at the specified address in West Sacramento.
What You Should Know About This Form
What is the purpose of the Medical Choice Form?
The Medical Choice Form allows eligible individuals to select their Medi-Cal health plan. By completing this form, you are indicating your preference for healthcare coverage. It is essential for ensuring that you have access to the services that best meet your needs.
Who needs to fill out the Medical Choice Form?
Every person in your household who receives Medi-Cal benefits should be listed on the form. Ensure that all required information is filled out for each individual receiving assistance. If you have more than three family members, you can call for additional forms.
How do I complete the form correctly?
To fill out the form, use a blue or black pen and print clearly. Be sure to provide full names, Social Security numbers, and contact details. Select your chosen health plan and input any required clinic codes associated with your provider.
What do I do if I encounter difficulties filling out the form?
If you need assistance, you can call 1-800-430-4263. Free help is available for anyone needing guidance in completing the Medical Choice Form.
What health plans can I choose from?
The available plans include Blue Cross, Care 1st, HealthNet, Kaiser, Western Health Advantage, and Regular Medi-Cal. Review each plan's details to find the one that aligns best with your healthcare needs.
What if I want to change my Medi-Cal health plan?
If you or any family member needs to change plans, complete the form and specify the reasons for the change. Indicate details such as choosing a preferred doctor or issues with your current plan. Your feedback is crucial in the selection process.
What happens to my information submitted on the form?
The information on your Medical Choice Form is securely retained by the Department of Health Care Services. It will be used solely for the purpose of enrolling or disenrolling you from your chosen Medi-Cal Health Plan. Other authorized agencies may access it when needed.
What does the statement of understanding mean?
The statement of understanding signifies that you are aware of how your choices will impact your Medi-Cal health care. It explains rights concerning your information, including your ability to review your Medi-Cal file unless it is involved in an investigation.
How do I submit the completed Medical Choice Form?
After filling out both sides of the form, mail it to the California Department of Health Services at Health Care Options, Box 989009, West Sacramento, CA 95798-9850. Ensure that all signatures are in place before submission.
Common mistakes
Filling out the Medi-Cal Choice Form can be straightforward, but many people make mistakes that can cause delays or complications. One common error is not filling in all required sections. If you skip a section or fail to provide information for each family member, it may delay the processing of your application. All family members receiving Medi-Cal must be included; don't leave anyone out.
Another frequent mistake involves incomplete contact information. It’s crucial that your phone number and address are filled out accurately, as this is how the health plan will reach you. If any part of your address or phone number is incorrect or missing, you risk missing important communication about your healthcare.
People often forget to use blue or black ink, as specified in the instructions. Using a different color can lead to your form being rejected or delayed. It may seem minor, but following instructions can save time and frustration. Make sure to use a pen and print legibly, so your information is clear to those processing it.
Finally, many applicants neglect to review their selections before submitting the form. Double-check that you’ve chosen the correct health plan and provided the necessary clinic code if applicable. Mistakes here can mean you are enrolled in a plan that doesn’t fit your needs. Take a moment to review everything before you send it off to ensure a smoother enrollment process.
Documents used along the form
The Medical Choice Form is a vital document for families accessing Medi-Cal services, helping to declare their healthcare plan preferences. However, it is not used in isolation. Several other forms and documents often accompany it to ensure a smooth enrollment process and adherence to legal requirements. Here are five essential documents to be aware of:
- Medi-Cal Application for Benefits: This application serves as the initial request for Medi-Cal benefits. It collects personal information, financial details, and household status to determine eligibility. Filling it out thoroughly is crucial to avoid delays in receiving necessary healthcare coverage.
- Pre-Enrollment Form: Designed for potential Medi-Cal participants, this form helps gather preliminary information. It assists in assessing eligibility before the formal application process begins, thereby streamlining the enrollment experience for applicants.
- Proof of Income Verification: Individuals must submit documents such as pay stubs, tax returns, or bank statements. This verification is required to validate income claims made in the application, ensuring that applicants meet the income criteria for Medi-Cal eligibility.
- Identity Verification Documentation: Applicants are often required to provide identification documents, such as a driver's license or social security card. This ensures proper identification and prevents fraud within the program.
- Plan Change Request Form: When beneficiaries wish to change their Medi-Cal health plan, this form details their reasons for the switch. It can help clarify issues with current plans and facilitate a transition to a new healthcare provider more suited to their needs.
Understanding these documents can significantly enhance the Medi-Cal application and enrollment process. Timely submission and accurate completion of these forms can alleviate unnecessary complications, ensuring that individuals and families have access to the medical care they require. Acting promptly is essential in navigating this process effectively.
Similar forms
- Medicare Enrollment Form: Like the Medical Choice form, this document allows individuals to select health plans under Medicare. It requires personal information for applicants and permits selection of preferred providers, ensuring that specific health care needs are addressed.
- Health Insurance Marketplace Application: This form helps individuals apply for health coverage through the Health Insurance Marketplace. Similar to the Medical Choice form, it collects household information and preferences regarding health plan choices, ensuring that each applicant understands their available options.
- Employer Health Insurance Enrollment Form: Employees typically fill out this form to enroll in health insurance offered by their employer. It shares similarities with the Medical Choice form in that it requires personal and dependent information while allowing selections of preferred coverage options.
- Medicaid Application Form: This form is designed to determine eligibility for Medicaid. Both it and the Medical Choice form require detailed applicant information and enable selection of health coverage preferences, making it essential for accessing necessary healthcare services.
- Supplemental Health Insurance Enrollment Form: Individuals use this form to add supplemental insurance to existing coverage. It has a similar structure to the Medical Choice form by requesting personal details and providing options for additional health benefits that may suit individual needs.
- Long-Term Care Insurance Application: This document allows individuals to apply for long-term care insurance coverage. Both the Long-Term Care Insurance Application and the Medical Choice form guide individuals in providing personal information while allowing them to select the coverage that best fits their situation.
- Children's Health Insurance Program (CHIP) Application: This application is for families needing health insurance for children. Much like the Medical Choice form, it gathers extensive information about the family and preferences for coverage, facilitating access to essential health services for children in need.
Dos and Don'ts
When filling out the Medical Choice form, it's essential to be meticulous to ensure your application is processed smoothly. Here are seven tips about what to do and what to avoid:
- Do use a blue or black pen to fill out the form.
- Do print clearly to ensure all your details are legible.
- Do provide complete information for every individual in your household receiving Medi-Cal.
- Do include your choice of health plan and fill in the corresponding code completely.
- Don't leave any required sections blank; this can delay your application.
- Don't submit the form without reviewing it for accuracy.
- Don't forget to sign the form, as your signature is necessary for processing.
Misconceptions
Misconception 1: The Medical Choice Form is only for people who are new to Medi-Cal.
This is not true. Existing Medi-Cal recipients may also need to fill out this form if they want to change their health plan or if their circumstances change, such as moving or having a new family member apply for coverage.
Misconception 2: You must complete the entire form in one sitting, or it will be discarded.
This is a common concern, but it’s not the case. You can take your time filling out the Medical Choice Form. Just make sure to complete it before mailing it to ensure your choices are reflected accurately in your health care plan.
Misconception 3: My personal information will not be kept safe.
In reality, the Department of Health Care Services takes privacy seriously. The information you provide is used only for enrollment purposes and is protected under confidentiality guidelines.
Misconception 4: Filling out the form is too complicated and has to be done perfectly.
While the form does require specific information, help is available. You can call 1-800-430-4263 for assistance, and it’s okay to ask questions if you feel uncertain about any part.
Misconception 5: Once you submit the form, there’s no way to change your mind about your health plan.
Incorrect. If you realize that you've made a mistake or want to opt for a different plan after submitting, you usually have options to make changes. It's important to check with Medi-Cal regarding deadlines and procedures for making updates to your choice.
Key takeaways
Understanding the process of filling out the Medical Choice form is crucial for ensuring that individuals receive the correct Medi-Cal benefits. Here are some key takeaways:
- Complete Both Sides: Ensure that both sides of the form are filled out completely. Incomplete forms may lead to delays in processing or incorrect enrollments.
- Information Accuracy: Use a blue or black pen to print legibly. Be sure to include all required information for each household member enrolled in Medi-Cal.
- Health Plan Selection: Carefully choose a health plan from the listed options. If you decide on a specific plan, enter the corresponding doctor or clinic code as detailed in the Provider Directory.
- Extra Family Members: If there are more than three family members in your household who require coverage, call 1-800-430-4263 for an additional form.
- Submission Process: After filling out the form, mail it to the designated address: California Dept. of Health Services, Health Care Options, Box 989009, West Sacramento, CA 95798-9850.
Browse Other Templates
How to Write a Letter Requesting Donations - Highlight your organization’s achievements to demonstrate your capability to use donations effectively.
Mdm Monthly Report Format - Regular updates through this form help identify challenges and solutions promptly.