Fill Out Your Medical Lift Chair Form
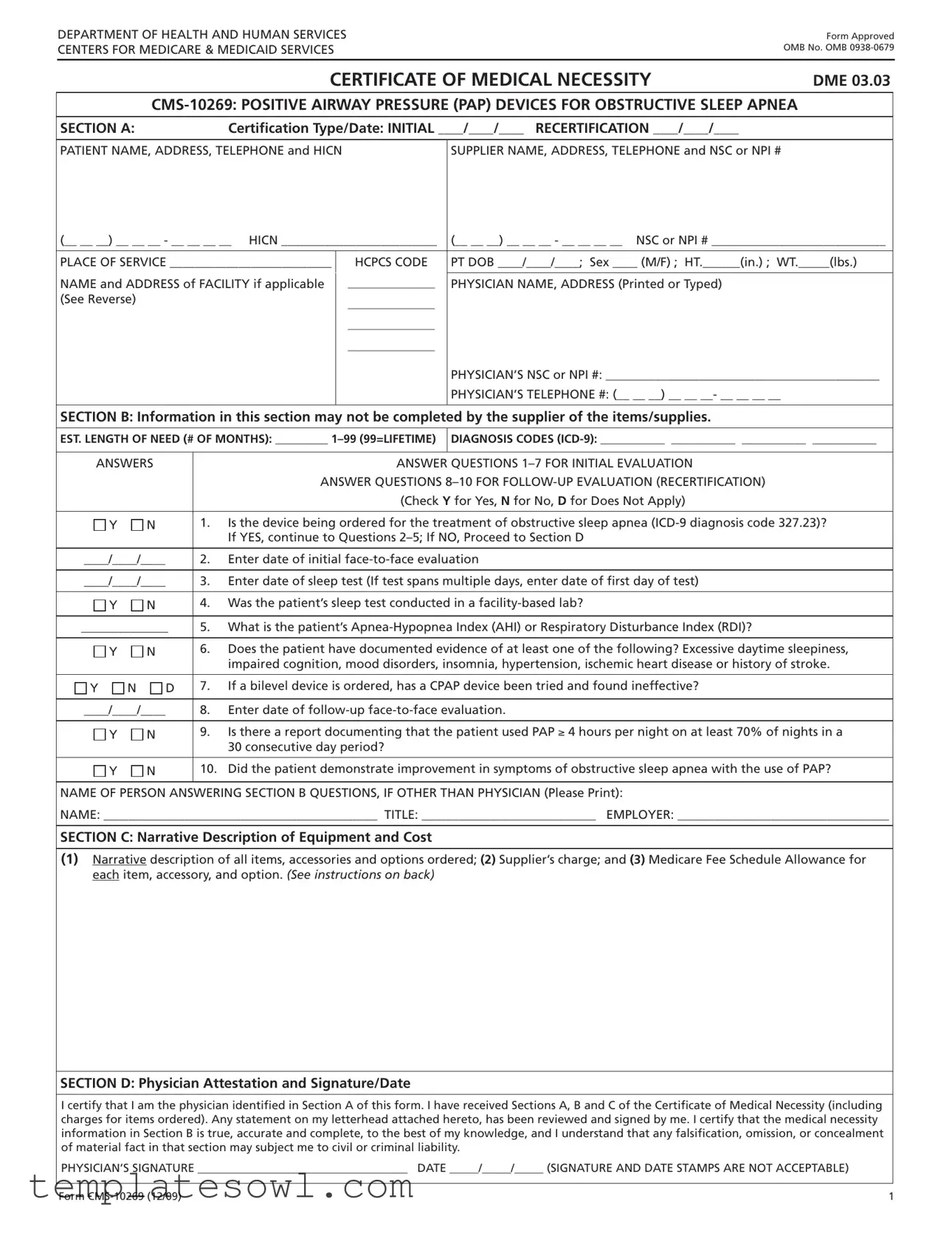
The Medical Lift Chair form is a critical component utilized within the healthcare system to establish the necessity for requesting durable medical equipment (DME) for patients in need. This certification process is framed by specific requirements outlined by the Centers for Medicare & Medicaid Services (CMS). The form serves not only as a request but also as a certification that verifies the medical necessity of a lift chair for patients who require assistance with mobility due to medical conditions. Essential information such as patient identification, supplier details, and the physician’s credentials must be meticulously filled out in Sections A and C of the form, ensuring that all parties involved have accurate data. Section B gathers clinical information that assesses the patient’s medical need, including diagnosing codes and responses to specific evaluation questions. Verification of this information comes through the physician's signature in Section D, attesting to the truthfulness and completeness of the details submitted. It is crucial that healthcare providers understand the importance of accurately completing this form to facilitate appropriate patient care and compliance with Medicare requirements.
Medical Lift Chair Example
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES
Form Approved OMB No. OMB
|
CERTIFICATE OF MEDICAL NECESSITY |
DME 03.03 |
|
|
|
||
SECTION A: |
Certification Type/Date: INITIAL ____/____/____ RECERTIFICATION ____/____/____ |
|
|
|
|
|
|
PATIENT NAME, ADDRESS, TELEPHONE and HICN |
SUPPLIER NAME, ADDRESS, TELEPHONE and NSC or NPI # |
|
|
(__ __ __) __ __ __ - __ __ __ __ HICN _________________________ |
(__ __ __) __ __ __ - __ __ __ __ NSC or NPI # ____________________________ |
|
|
|
|
PLACE OF SERVICE __________________________ |
HCPCS CODE |
PT DOB ____/____/____; Sex ____ (M/F) ; HT.______(in.) ; WT._____(lbs.) |
NAME and ADDRESS of FACILITY if applicable |
________________ |
PHYSICIAN NAME, ADDRESS (Printed or Typed) |
(See Reverse) |
________________ |
|
|
|
|
|
________________ |
|
|
________________ |
|
|
|
PHYSICIAN’S NSC or NPI #: ____________________________________________ |
|
|
PHYSICIAN’S TELEPHONE #: (__ __ __) __ __ __- __ __ __ __ |
|
|
|
SECTION B: Information in this section may not be completed by the supplier of the items/supplies.
EST. LENGTH OF NEED (# OF MONTHS): _________
DIAGNOSIS CODES
ANSWERS |
|
|
ANSWER QUESTIONS |
|
|
|
|
|
ANSWER QUESTIONS |
|
|
|
|
(Check Y for Yes, N for No, D for Does Not Apply) |
|
|
|
|
|
Y |
N |
|
1. |
Is the device being ordered for the treatment of obstructive sleep apnea |
|
|
|
|
If YES, continue to Questions |
____/____/____ |
|
2. |
Enter date of initial |
|
|
|
|
|
|
____/____/____ |
|
3. |
Enter date of sleep test (If test spans multiple days, enter date of first day of test) |
|
|
|
|
|
|
Y |
N |
|
4. |
Was the patient’s sleep test conducted in a |
|
|
|
||
______________ |
5. |
What is the patient’s |
||
|
|
|
|
|
Y |
N |
|
6. |
Does the patient have documented evidence of at least one of the following? Excessive daytime sleepiness, |
|
|
|
|
impaired cognition, mood disorders, insomnia, hypertension, ischemic heart disease or history of stroke. |
Y |
N |
D |
7. |
If a bilevel device is ordered, has a CPAP device been tried and found ineffective? |
|
|
|
|
|
____/____/____ |
|
8. |
Enter date of |
|
|
|
|
|
|
Y |
N |
|
9. |
Is there a report documenting that the patient used PAP ≥ 4 hours per night on at least 70% of nights in a |
|
|
|
|
30 consecutive day period? |
Y |
N |
|
10. |
Did the patient demonstrate improvement in symptoms of obstructive sleep apnea with the use of PAP? |
|
|
|
|
|
NAME OF PERSON ANSWERING SECTION B QUESTIONS, IF OTHER THAN PHYSICIAN (Please Print):
NAME: ____________________________________________ TITLE: ____________________________ EMPLOYER: __________________________________
SECTION C: Narrative Description of Equipment and Cost
(1)Narrative description of all items, accessories and options ordered; (2) Supplier’s charge; and (3) Medicare Fee Schedule Allowance for each item, accessory, and option. (See instructions on back)
SECTION D: Physician Attestation and Signature/Date
I certify that I am the physician identified in Section A of this form. I have received Sections A, B and C of the Certificate of Medical Necessity (including charges for items ordered). Any statement on my letterhead attached hereto, has been reviewed and signed by me. I certify that the medical necessity information in Section B is true, accurate and complete, to the best of my knowledge, and I understand that any falsification, omission, or concealment of material fact in that section may subject me to civil or criminal liability.
PHYSICIAN’S SIGNATURE ____________________________________ DATE _____/_____/_____ (SIGNATURE AND DATE STAMPS ARE NOT ACCEPTABLE)
Form |
1 |

INSTRUCTIONS FOR COMPLETING THE CERTIFICATE OF MEDICAL NECESSITY
FOR POSITIVE AIRWAY PRESSURE (PAP) DEVICES FOR OBSTRUCTIVE SLEEP APNEA
SECTION A: (May be completed by the supplier)
CERTIFICATION TYPE/DATE: If this is an initial certification for this patient, indicate this by placing date (MM/DD/YY) needed initially in the space marked “INITIAL.” If this is a revised certification (to be completed when the physician changes the order, based on the patient’s changing clinical needs), indicate the initial date needed in the space marked “INITIAL,” and also indicate the recertification date in the space marked “REVISED.” If this is a recertification, indicate the initial date needed in the space marked “INITIAL,” and also indicate the recertification date in the space marked “RECERTIFICATION.” Whether submitting a REVISED or a RECERTIFIED CMN, be sure to always furnish the INITIAL date as well as the REVISED or RECERTIFICATION date.
PATIENT INFORMATION: Indicate the patient’s name, permanent legal address, telephone number and his/her health insurance claim number (HICN) as it appears on his/her Medicare card and on the claim form.
SUPPLIER INFORMATION: Indicate the name of your company (supplier name), address and telephone number along with the National Provider Identification (NPI) number assigned to you by the National Supplier Clearinghouse (NSC).
PLACE OF SERVICE: Indicate the place in which the item is being used, i.e., patient’s home is 12, skilled nursing facility (SNF) is 31, End Stage Renal Disease (ESRD) facility is 65, etc. Refer to the DME MAC supplier manual for a complete list.
FACILITY NAME: If the place of service is a facility, indicate the name and complete address of the facility.
HCPCS CODES: List all HCPCS procedure codes for items ordered that require a CMN. Procedure codes that do not require certification should not be listed on the CMN.
PATIENT DOB, HEIGHT, WEIGHT AND SEX: Indicate patient’s date of birth (MM/DD/YY) and sex (male or female); height in inches and weight in pounds, if requested.
PHYSICIAN NAME, ADDRESS: Indicate the physician’s name and complete mailing address.
NPI: Accurately indicate the ordering physician’s National Provider Identification number (NPI).
PHYSICIAN’S TELEPHONE NO: Indicate the telephone number where the physician can be contacted (preferably where records would be accessible pertaining to this patient) if more information is needed.
SECTION B: (May not be completed by the supplier. While this section may be completed by a
EST. LENGTH OF NEED: Indicate the estimated length of need (the length of time the physician expects the patient to require use of the ordered item) by filling in the appropriate number of months. If the physician expects that the patient will require the item for the duration of his/her life, then enter 99.
DIAGNOSIS CODES: In the first space, list the ICD9 code that represents the primary reason for ordering this item. List any additional ICD9 codes that would further describe the medical need for the item (up to 3 codes).
QUESTION SECTION: This section is used to gather clinical information to determine medical necessity. Answer each question which applies to the items ordered, checking “Y” for yes, “N” for no, or fill in the blank if other information is requested.
NAME OF PERSON ANSWERING SECTION B QUESTIONS: If a clinical professional other than the ordering physician (e.g., home health nurse, physical therapist, dietician) or a physician employee answers the questions of Section B, he/she must print his/her name, give his/her professional title and the name of his/her employer where indicated. If the physician is answering the questions, this space may be left blank.
SECTION C: (To be completed by the supplier)
NARRATIVE DESCRIPTION OF EQUIPMENT & COST: Supplier gives (1) a narrative description of the item(s) ordered, as well as all options, accessories, supplies and drugs; (2) the supplier’s charge for each item, option, accessory, supply and drug; and (3) the Medicare fee schedule allowance for each item/option/accessory/supply/drug, if applicable.
SECTION D: (To be completed by the physician)
PHYSICIAN ATTESTATION: The physician’s signature certifies (1) the CMN which he/she is reviewing includes Sections A, B, C and D; (2) the answers in Section B are correct; and (3) the
PHYSICIAN SIGNATURE AND DATE: After completion and/or review by the physician of Sections A, B and C, the physician must sign and date the CMN in Section D, verifying the Attestation appearing in this Section. The physician’s signature also certifies the items ordered are medically necessary for this patient. Signature and date stamps are not acceptable.
According to the Paperwork Reduction Act of 1995, no persons are required to respond to a collection of information unless it displays a valid OMB control number. The valid OMB control number for this information collection is
15 minutes per response, including the time to review instructions, search existing resources, gather the data needed, and complete and review the information collection. If you have any comments concerning the accuracy of the time estimate or suggestions for improving this form, please write to: CMS, 7500 Security Blvd.,
Form |
2 |
Form Characteristics
| Fact Name | Details |
|---|---|
| Form Title | CERTIFICATE OF MEDICAL NECESSITY DME 03.03 CMS-10269 |
| Approval Info | Form approved by OMB with control number 0938-0679. |
| Primary Purpose | The form certifies medical necessity for Positive Airway Pressure (PAP) devices for obstructive sleep apnea. |
| Certification Type | The form can be used for both initial certifications and recertifications. |
| Required Information | Patient and supplier details must be completed, including HICN, NPI, and place of service. |
| Diagnosis Codes | ICD-9 codes must be provided to document the medical reason for the equipment. |
| Physician's Role | Must review and sign off on the information provided in the form, affirming its accuracy. |
| Medical Necessity | Clinical information must support the necessity of the PAP device for the patient's condition. |
| State-Specific Governing Laws | Varies by state; check local regulations regarding medical necessity and equipment prescriptions. |
Guidelines on Utilizing Medical Lift Chair
Filling out the Medical Lift Chair form might seem overwhelming at first, but breaking it down into steps can make the process straightforward. You'll need personal and medical information, which is essential for obtaining the necessary approval. Keep all relevant documents handy to ensure you complete the form accurately and promptly.
- Begin with Section A. Identify the certification type by marking either "INITIAL" for first-time requests or "RECERTIFICATION" for ongoing needs. Fill in the corresponding date.
- Provide the patient's information. Include the full name, address, phone number, and health insurance claim number (HICN).
- Next, enter the supplier's information. Indicate your company name, address, phone number, and your National Provider Identification (NPI) number.
- In the place of service field, specify where the device will be used. You may need to refer to a specific list for correct codes.
- Complete the fields for patient's date of birth, height, weight, and sex. Ensure accuracy here as these details are important.
- If applicable, provide the facility name where the patient will receive the equipment.
- List the appropriate HCPCS codes for the items being ordered.
- Now fill out Section B. Start with the estimated length of need in months, then enter diagnosis codes, focusing on the primary condition.
- Answer the questions 1-7 related to initial evaluation. Use "Y" for yes, "N" for no, or "D" for does not apply where indicated.
- If filling out for a follow-up evaluation, answer questions 8-10 accordingly.
- Insert the name of the person answering Section B questions if it's not the physician.
- Moving to Section C, provide a narrative description of the equipment being requested, its cost, and associated Medicare fees.
- In Section D, the physician must sign and date the form. This confirms their agreement with the provided information.
- Finally, double-check all sections for accuracy before submitting the form to ensure completeness.
What You Should Know About This Form
What is a Medical Lift Chair form?
The Medical Lift Chair form is a document required for patients who need medical lift chairs due to health conditions. This form certifies the necessity of the lift chair for the patient’s treatment and provides necessary information for Medicare and Medicaid services to process claims for reimbursement.
Who needs to fill out the Medical Lift Chair form?
The form must be completed by the ordering physician, detailing the medical necessity of the lift chair. Additionally, suppliers will provide information about the equipment and costs associated with it. Accurate completion is essential for processing the claim effectively.
What information is required in Section A of the form?
Section A requests certification details, including the patient’s name, address, telephone number, and Health Insurance Claim Number (HICN). The supplier's information, including their address and National Supplier Clearinghouse (NSC) number, must also be provided. Details about the patient's medical condition, height, weight, and physician information are also included in this section.
What does Section B of the form involve?
Section B contains clinical questions regarding the patient's condition. This section assesses whether the lift chair is required for the treatment of a specific medical diagnosis. Information about evaluations, test dates, and evidence of symptoms such as excessive daytime sleepiness must be documented here. This section must only be completed by qualified medical staff under the physician's supervision.
Why is the estimated length of need important?
The estimated length of need must be indicated, as it informs the supplier and insurers about how long the lift chair is expected to be necessary for the patient. This can range from 1 to 99 months, with 99 indicating a lifetime need.
What is included in Section C?
In Section C, the supplier provides a narrative description of the lift chair, including any accessories or options ordered. They must also include their charge and the Medicare fee schedule allowance for each item. This section details the financial aspect of the request.
What does the physician need to certify in Section D?
In Section D, the physician must sign and date the form, certifying that the information provided in Sections A, B, and C is accurate and complete. This signature confirms the medical necessity of the lift chair for the patient.
How does the form impact Medicare coverage?
The Medical Lift Chair form is critical for Medicare coverage as it establishes the medical necessity of the equipment. Properly completed forms help ensure that claims for the lift chair are approved, allowing patients to receive the necessary assistance in their homes.
What should I do if I have questions about the form?
If there are questions about completing the form or understanding its requirements, contacting the supplier or the physician’s office can provide clarification. Resources from the Centers for Medicare & Medicaid Services can also offer guidance on completing the Medical Lift Chair form accurately.
Common mistakes
Filling out the Medical Lift Chair form may appear straightforward, but several common mistakes can lead to delays or denials. These errors can affect the patient’s access to necessary medical equipment. Awareness of these pitfalls can help ensure proper submission of the form and ultimately secure the required services.
One frequent mistake is failing to provide complete patient information. Names, addresses, telephone numbers, and the Health Insurance Claim Number (HICN) must be filled out precisely. Any missing detail may result in delays. Accurate and complete information is crucial for processing the request without complications.
Another error involves inaccurately identifying the type of certification. Individuals may mark the wrong box for either "INITIAL" or "RECERTIFICATION." This nuance is vital, as each type has specific requirements. Submitting the wrong certification type can cause significant setbacks.
The estimated length of need is often overlooked or improperly filled in. The form requires an exact number of months. Some might simply leave this section blank or use vague terms like “lifetime” instead. Not specifying the number of months can lead to automatic denials.
When detailing diagnostic codes, many struggle. Not providing sufficient ICD-9 codes for the medical necessity of the item can hinder approval. It is essential to include both the primary and any additional codes relevant to the patient’s condition.
Perspective on follow-up evaluations is also key. Individuals sometimes skip answering questions related to follow-up evaluations. Questions that check for the patient's use of the medical equipment and changes in symptoms are critical for establishing ongoing medical necessity. Failure to answer these questions adequately can incur additional scrutiny.
Documentation from the sleep test often gets ignored. Many forms are submitted without confirming whether the test was conducted in a facility-based lab. This information is crucial to substantiate the medical necessity for the lift chair.
If a bilevel device is needed, confirming that a CPAP device was previously tried is essential. Some might neglect this question entirely, jeopardizing their application. It is important to ensure all required steps are documented and detailed in the form.
A common mistake involves the physician attestation section. Some individuals do not have the physician's signature dated correctly. The absence of a signature or a date stamp will lead to immediate rejection of the form.
Lastly, failure to provide a clear narrative description of the equipment and associated costs is another error. This section should list every item requested, including accessories and their respective costs. A vague or incomplete description may prompt delays in processing.
In summary, awareness of these prevalent mistakes can make a significant difference in the effectiveness of filling out the Medical Lift Chair form. Precise attention to detail not only expedites the process but also ensures patients receive the essential medical equipment they require.
Documents used along the form
The Medical Lift Chair form is a vital document in the healthcare process, particularly for patients requiring medical equipment. Along with this form, there are several other documents that often accompany it. These documents help to ensure that patients receive the necessary equipment and care they require from their healthcare providers.
- Certificate of Medical Necessity (CMN): This document confirms that a medical item is essential for a patient's treatment. It provides detailed information about the patient's health condition and why a specific piece of equipment is needed.
- Prescription Form: This form is signed by the physician to formally request a specific medical device for a patient. It includes medication dosages, device specifications, and instructions for use.
- Insurance Authorization Form: This document is submitted to the patient's insurance provider for approval before the device can be purchased. It outlines the patient's medical necessity and cost estimates for the lifting chair.
- Patient's Medical History: This record contains comprehensive information about the patient’s past and present health conditions. It is crucial for establishing the need for a medical lift chair.
- Detailed Product Information: This documentation provides specifications, user guidelines, and functional details about the medical lift chair being requested.
- Payment Agreement Form: This document details the payment terms and responsibilities between the patient and supplier. It helps clarify co-pays, deductibles, and other associated costs.
- Follow-up Assessment Form: After receiving the lift chair, this form is used to evaluate the patient's ongoing need for the equipment. It may include observations about how well the device meets the patient’s needs.
These documents work together to support the patient's journey in securing a medical lift chair. Each piece plays a unique role in ensuring that patients get the right care and equipment they require to improve their quality of life.
Similar forms
The Medical Lift Chair form is closely related to several other documents, each serving important roles in the medical and insurance processes. Below are documents that share similarities with the Medical Lift Chair form, along with explanations of how they are alike:
- Certificate of Medical Necessity (CMN) for Durable Medical Equipment (DME): Like the Medical Lift Chair form, this document is used to certify that a medical device is necessary for a patient's care, ensuring insurance coverage for the equipment.
- Prescription for Durable Medical Equipment: Both documents require a physician's signature to confirm that the patient needs a specific medical device, making them essential for facilitating insurance claims.
- Prior Authorization Request: Similar to the Medical Lift Chair form, this document is submitted to insurers to seek approval for a particular medical service or device before it is provided to the patient.
- Home Health Care Plan: This document outlines the medical care that a patient will receive at home. It is similar in that it may detail the need for assistive devices, just like the Medical Lift Chair form details the need for a lift chair.
- Equipment Rental Agreement: This agreement is related as both documents may involve the rental or purchase of equipment. It formalizes the terms under which the medical device is provided.
- Diagnosis Codes (ICD-10) Documentation: Both documents require accurate coding to specify medical conditions. The Medical Lift Chair form includes diagnosis codes to justify the medical need for the chair.
- Medicare Claims Form (CMS-1500): This form is used to bill Medicare directly for medical services and related equipment. Like the Medical Lift Chair form, it includes vital patient and provider information necessary for processing claims.
- Patient Evaluation Form: This form captures clinical assessments performed by healthcare providers. Similar to the Medical Lift Chair form, it documents justification for the need for medical equipment based on a patient’s condition.
Dos and Don'ts
Do:
- Fill in all required fields completely to avoid delays in processing.
- Double-check the patient's health insurance claim number before submitting.
- Clearly indicate the type of certification: initial or recertification.
- Provide accurate diagnosis codes to support medical necessity.
- Ensure the physician's signature is included and dated correctly.
Don't:
- Do not leave any mandatory sections blank; incomplete forms may be returned.
- Avoid using stamps for the physician's signature; hand sign only.
- Do not submit without verifying the patient's personal information.
- Do not confuse the estimated length of need with the recertification dates.
- Never falsify or omit information, as this may lead to legal issues.
Misconceptions
1. Medical Lift Chairs are only for elderly patients. While many elderly individuals benefit from lift chairs, they can serve people of any age who struggle with mobility issues or have medical conditions that affect their ability to stand or sit independently.
2. Lift Chairs are not covered by insurance. Many insurance plans, including Medicare, may cover lift chairs when they are deemed medically necessary. It is essential to check with your insurance provider for specific coverage details.
3. All lift chairs are the same. Lift chairs come in various designs, styles, and functions, including different sizes, reclining angles, and lifting capabilities. Selecting the right one for an individual's needs is crucial for comfort and effectiveness.
4. Using a lift chair reduces independence. In reality, a lift chair promotes independence by aiding users in standing or sitting without the assistance of others. This can lead to increased confidence and self-sufficiency.
5. Lift chairs are difficult to move and transport. Most lift chairs have features that allow them to be easily moved. Some are designed to fit through standard doorways and can be disassembled for easier transport.
6. Lift chairs are strictly for indoor use. While they are generally designed for home use, some models are portable and suitable for outdoor use in sheltered areas, allowing people to enjoy fresh air and outdoor environments comfortably.
7. Lift chairs are not customizable. Many lift chairs offer various configurations and accessories, such as heated seats, massage features, and different fabrics, allowing users to customize them to their preferences and needs.
8. Once ordered, lift chairs cannot be returned. Most retailers offer return policies on lift chairs, provided they are in original condition. Always review the return policy before making a purchase to ensure satisfactory purchasing experience.
9. Lift chairs are only beneficial for people with chronic pain. While those suffering from chronic pain often find relief using these chairs, they can also assist people recovering from surgery, injury, or temporary disabilities.
Key takeaways
Understanding the nuances of filling out and using the Medical Lift Chair form is crucial for both healthcare providers and patients. Here are six key takeaways that can help streamline the process:
- Certification Clarity: Clearly indicate whether the form is an initial certification or a recertification. This distinction is important for accurate processing.
- Accurate Patient Information: Ensure that the patient's name, contact details, and health insurance claim number are accurately recorded. This ensures proper identification and less likelihood of processing errors.
- Detailed Narrative: When describing the equipment in Section C, include all necessary details such as types of items ordered, their costs, and Medicare fee schedule allowances. This transparency aids in the review process.
- Physician's Signature: The physician must personally sign Section D to validate the information in the form. Remember, stamped signatures are not acceptable.
- Diagnostic Codes: Complete the diagnosis codes section with precision. These codes help establish medical necessity and influence whether Medicare will approve coverage.
- Review and Verification: Before submission, ensure that Sections A, B, and C have been thoroughly reviewed. A complete and accurate form reduces the risk of delays in obtaining necessary equipment.
Browse Other Templates
What Is a Tax Organizer - Maintain an organized record of your financial documents for tax filing efficiency.
A Health Risk Assessment Should Be Completed - Your health assessment answers help inform future healthcare decisions.