Fill Out Your Medical Singapore Form
The Medical Singapore form is a critical document intended for students seeking admission to various courses within Singapore, particularly at the Singapore Polytechnic. Designed to assess each applicant's fitness for their chosen course, the form is divided into two main parts: the first is to be completed by the student and includes personal particulars, medical history, and family and social history details. The second part, which must be filled out by a registered medical practitioner in Singapore, involves a comprehensive medical examination. This examination assesses physical and mental fitness, with specific tests such as vision acuity and blood pressure measuring key health indicators. Students with particular medical conditions are advised against pursuing certain courses, ensuring that their health and safety are prioritized. Confidentiality is strictly maintained throughout the process, with data used solely for assessment purposes. Furthermore, students are required to undergo a medical check-up and possibly an X-ray to meet admission criteria, thereby instilling a sense of responsibility for their health. Understanding the requirements and significance of the Medical Singapore form is essential for prospective students to navigate the admissions landscape effectively.
Medical Singapore Example
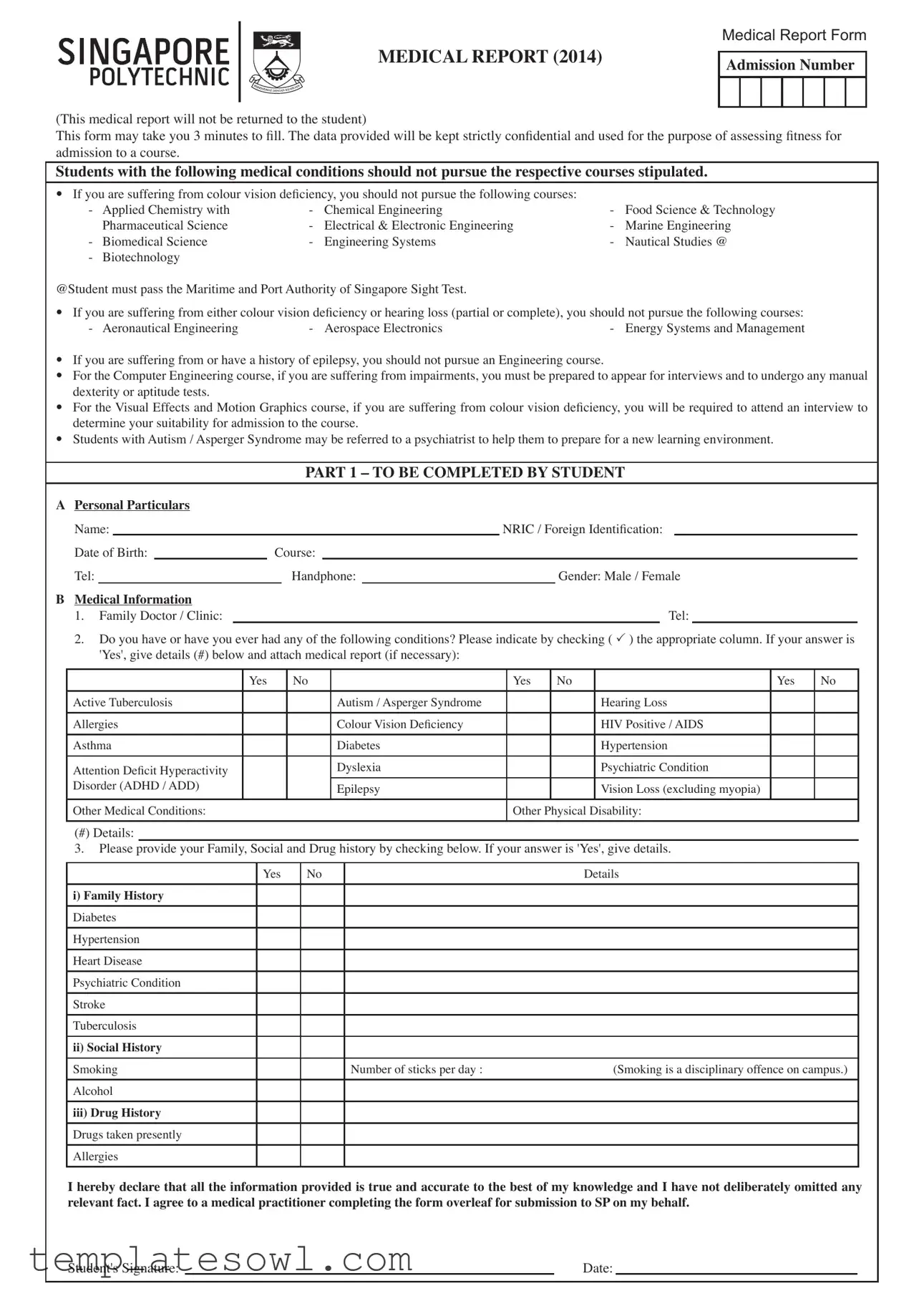
MEDICAL REPORT (2014)
Medical Report Form
Admission Number
(This medical report will not be returned to the student)
This form may take you 3 minutes to ill. The data provided will be kept strictly conidential and used for the purpose of assessing itness for admission to a course.
Students with the following medical conditions should not pursue the respective courses stipulated.
•If you are suffering from colour vision deiciency, you should not pursue the following courses:
- |
Applied Chemistry with |
- |
Chemical Engineering |
- Food Science & Technology |
|
|
Pharmaceutical Science |
- Electrical & Electronic Engineering |
- |
Marine Engineering |
|
- |
Biomedical Science |
- |
Engineering Systems |
- |
Nautical Studies @ |
- |
Biotechnology |
|
|
|
|
@Student must pass the Maritime and Port Authority of Singapore Sight Test.
•If you are suffering from either colour vision deiciency or hearing loss (partial or complete), you should not pursue the following courses:
- Aeronautical Engineering |
- Aerospace Electronics |
- Energy Systems and Management |
•If you are suffering from or have a history of epilepsy, you should not pursue an Engineering course.
•For the Computer Engineering course, if you are suffering from impairments, you must be prepared to appear for interviews and to undergo any manual dexterity or aptitude tests.
•For the Visual Effects and Motion Graphics course, if you are suffering from colour vision deiciency, you will be required to attend an interview to determine your suitability for admission to the course.
•Students with Autism / Asperger Syndrome may be referred to a psychiatrist to help them to prepare for a new learning environment.
PART 1 – TO BE COMPLETED BY STUDENT
APersonal Particulars
Name: |
|
|
|
|
|
|
NRIC / Foreign Identiication: |
|
||
Date of Birth: |
|
Course: |
|
|
|
|
||||
Tel: |
|
|
|
Handphone: |
|
|
Gender: Male / Female |
|||
B Medical Information |
|
1. Family Doctor / Clinic: |
Tel: |
2.Do you have or have you ever had any of the following conditions? Please indicate by checking ( ) the appropriate column. If your answer is 'Yes', give details (#) below and attach medical report (if necessary):
|
Yes |
No |
|
Yes |
No |
|
Yes |
No |
Active Tuberculosis |
|
|
Autism / Asperger Syndrome |
|
|
Hearing Loss |
|
|
Allergies |
|
|
Colour Vision Deiciency |
|
|
HIV Positive / AIDS |
|
|
Asthma |
|
|
Diabetes |
|
|
Hypertension |
|
|
Attention Deicit Hyperactivity |
|
|
Dyslexia |
|
|
Psychiatric Condition |
|
|
Disorder (ADHD / ADD) |
|
|
Epilepsy |
|
|
Vision Loss (excluding myopia) |
|
|
Other Medical Conditions: |
|
|
Other Physical Disability: |
|
|
|||
(#) Details:
3.Please provide your Family, Social and Drug history by checking below. If your answer is 'Yes', give details.
Yes |
No |
Details |
i)Family History
Diabetes Hypertension Heart Disease Psychiatric Condition Stroke Tuberculosis
ii)Social History
Smoking |
Number of sticks per day : |
(Smoking is a disciplinary offence on campus.) |
Alcohol |
|
|
iii)Drug History
Drugs taken presently
Allergies
I hereby declare that all the information provided is true and accurate to the best of my knowledge and I have not deliberately omitted any relevant fact. I agree to a medical practitioner completing the form overleaf for submission to SP on my behalf.
Student's Signature: |
|
Date: |

Name : |
|
Admission No : |
|
Course : |
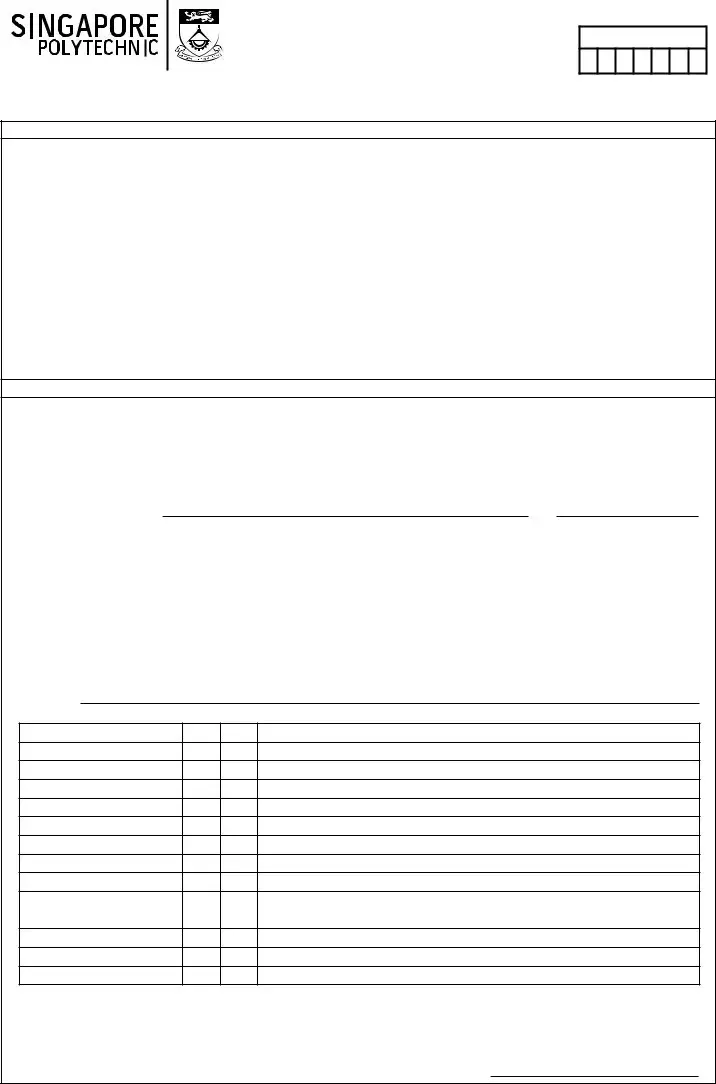
PART 2 – TO BE COMPLETED BY A MEDICAL PRACTITIONER REGISTERED IN SINGAPORE ONLY
|
Height (m) : |
|
|
|
BMI = |
Weight in kg |
|
Urine Analysis: |
Glucose |
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Weight (kg) : |
|
|
|
|
|
(Height in m)2 |
|
|
Protein |
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
If BMI > = 23 (moderate - |
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
BMI : |
|
|
|
|
|
|
|
|
high risk) |
|
|
Blood |
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Acuity of Vision |
|
|
|
|
|
|
|
|
Colour Vision (tick one only) |
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
R |
|
L |
|
Ishihara Test |
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
Without glasses |
|
|
|
|
|
|
|
|
|
|
Normal |
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
With glasses |
|
|
|
|
|
|
|
|
|
Partial: Red / Green deiciency |
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
History of Epilepsy: |
|
Yes |
|
No |
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
||||||||||||
|
If yes, |
|
|
|
|
|
|
|
|
Complete: Red / Green deiciency |
|
|
|
|||||||
|
|
Recovered |
|
|
Still on Medication |
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Chest |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PHYSICAL EXAMINATION |
|
|
|
|
|||
|
Eyes : |
|
|
|
|
|
|
|
|
Blood Pressure : |
|
|
|
|
||||||
|
Ears : |
|
|
|
|
|
|
|
|
Pulse : |
|
|
|
|
||||||
|
Nose : |
|
|
|
|
|
|
|
|
Heart : |
|
|
|
|
||||||
|
Teeth : |
|
|
|
|
|
|
|
|
Abdomen & Pelvis : |
|
|
|
|
||||||
|
Gums : |
|
|
|
|
|
|
|
|
Hernia (Enlarged Rings) : |
|
|
|
|
||||||
|
Tonsils : |
|
|
|
|
|
|
|
|
Skin : |
|
|
|
|
||||||
|
Back / Spine : |
|
|
|
|
|
|
|
|
Mental Disposition : |
|
|
|
|
||||||
|
Injury, Operation, Illness: |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Referrals (All fees are to be borne by the student.)
-Those with or suspected to have psychiatric condition must be referred to a psychiatrist for further assessment.
-Those with epilepsy must be referred to a Designated Workplace Doctor who will assess their itness for courses.
Blood Test (May be required at the discretion of the Medical Practitioner. All fees are to be borne by the student.) Test Result :
Certiication of Fitness
1.I have today completed a medical examination of the person named overleaf and ind this student for admission to be free / not free* from organic and infectious diseases.
2.The student is physically and mentally
•Fit / Unit* to pursue the course indicated.
•Fit / Unit* to pursue Any Other Course / Other Courses*
Remarks (if any) :
* Please delete accordingly. The student is deemed unit unless certiied it.
To be completed by the Medical Practitioner if the student is enrolling for the Diploma in Marine Engineering / Nautical Studies Course only
•Diploma in Marine Engineering Course
The student is it / unit* to be employed on board ship as Cadet Engineer / Engineer Oficer.
•Diploma in Nautical Studies Course
The student is it / unit* to be employed on board ship as a Cadet Deck Oficer.
Name of Registered Medical Practitioner:
Qualiications: |
|
|
|
|
|
(Signature of Doctor) |
(OFFICIAL STAMP) |
||
|
|
|||
Name and Address of Practice: |
|
|
|
|
|
|
Date: |
|
|
Medical
•Successful Applicants of all
•Bring along your SP Medical Report Form to the clinic. You may go to your own family doctor, private or company clinics for the medical
1)or mail in to Admissions Ofice, Singapore Polytechnic, 500 Dover Road, Singapore 139651 as soon as you have received it from your doctor.
•Alternatively, you may go to any one of the clinics listed. Those who go for their medical
•All
•Students will bear all medical charges including any referrals to Designated Workplace Doctors or other Specialists.
•If the doctor has recommended you to undergo a blood test, the cost of this blood test is additional. Initial blood test is estimated at S$20.00.
Please inform the Admissions Ofice immediately should you have a medical condition that prohibits you from pursuing the offered course (e.g. colour vision deiciency). SP will need to arrange for a course transfer.
Call
Clinics |
Opening Hours |
|
|
SATA CommHealth
You may wish to avoid the peak periods: weekday mornings and Saturdays as waiting times can be stretched. Rate:
• Singaporean / Permanent Resident: S$30.00 (inclusive of 7% GST)
• International Student: S$49.00 (inclusive of 7% GST)
SATA Uttamram Medical Centre |
Monday To Friday |
8.30 am to 5.00 pm |
|
351 Chai Chee Street |
|
Singapore 468982 |
Saturday |
Tel: |
8.30 am to 1.00 pm |
MRT Station: Bedok |
Weekend Surcharge: S$8.00 |
Bus Service: |
|
222 (from Bedok MRT Station, in front of Blk 27, New Upper Changi Road) |
Closed on Sundays & Public Holidays |
|
|
SATA Jurong Medical Centre |
Monday To Friday |
8.30 am to 5.00 pm |
|
Blk 135 Jurong Gateway Road |
|
Saturday |
|
Singapore 600135 |
8.30 am to 1.00 pm |
Tel: |
Weekend Surcharge: S$8.00 |
MRT Station: Jurong East |
|
Bus Service: |
Closed on Sundays & Public Holidays |
51, 66, 78, 79, 97, 98, 105, 197, 331 |
|
|
|
SATA Woodlands Medical Centre |
Monday To Friday |
8.30 am to 5.00 pm |
|
900 South Woodlands Drive |
|
Saturday |
|
Singapore 730900 |
8.30 am to 1.00 pm |
Tel: |
Weekend Surcharge: S$8.00 |
MRT Station: Woodlands |
|
Bus Interchange: |
Closed on Sundays & Public Holidays |
161, 168, 169, 178, 187, 856, 858, 900, 900A, 901, 902, 903, 911, 912, 913, 925, |
|
926, 950, 960, 961, 962, 963, 963E, 964, 965, 966, 967, 968, 969, 970, 971 |
|
|
|
SATA Ang Mo Kio Medical Centre |
Monday To Friday |
8.30 am to 5.00 pm |
|
Blk 715 Ang Mo Kio Avenue 6 |
Evening Clinic |
Singapore 560715 |
6.00 pm to 9.00 pm |
Tel: |
Surcharge: S$5.00 |
MRT Station: Ang Mo Kio |
|
Bus Interchange: |
Saturday |
13, 86, 138, 162, 851, 852, 853 |
8.30 am to 1.00 pm |
|
Weekend Surcharge: S$8.00 |
|
Closed on Sundays & Public Holidays |
|
|
• Singaporean / Permanent Resident: S$28.00 (inclusive of 7% GST) |
|
• International Student: S$47.50 (inclusive of 7% GST) |
|
|
|
Ang Mo Kio – Thye Hua Kwan Hospital |
Monday To Thursday |
17 Ang Mo Kio Avenue 9 |
8.45 am to 3.30 pm |
Singapore 569766 |
Lunch (Closed):12.00 noon to 2.00 pm |
Tel: |
|
MRT Station: Yio Chu Kang |
Friday and Saturday |
Bus Service: |
8.45 am to 12.00 noon |
76, 265, 268 |
|
|
Closed on Sundays & Public Holidays |
|
Last appointment for AM session is at 11am |
|
Last appointment for PM session is at 3 pm |
|
|
Form Characteristics
| Fact Name | Details |
|---|---|
| Purpose of the Form | This Medical Report Form is designed to assess fitness for admission to a course. |
| Confidentiality | The information provided will be kept strictly confidential and used only for assessment purposes. |
| Duration to Complete | Students may take approximately 3 minutes to fill out the form. |
| Eligibility Restrictions | Students with specific medical conditions, like color vision deficiency or epilepsy, may not pursue certain courses. |
| Medical Practitioner Requirement | A registered medical practitioner in Singapore must complete Part 2 of the form. |
| Course-Specific Requirements | Some courses require interviews or further assessments based on the applicant’s medical history. |
| Family and Social History | Applicants must disclose family health history, personal habits, and any drug use. |
| Submission Method | Medical reports can be submitted in person or mailed to the Admissions Office at Singapore Polytechnic. |
| Medical Charges | Students are responsible for all medical fees, including any required tests or referrals. |
Guidelines on Utilizing Medical Singapore
Completing the Medical Singapore form is essential for assessing your fitness for course admission. Follow the steps carefully to ensure accurate and complete submission.
- Gather all necessary personal information, including your name, NRIC or Foreign Identification, date of birth, course, telephone number, handphone number, and gender.
- In Part 1, section A, fill in your personal particulars as indicated.
- In section B, provide information about your family doctor or clinic and their contact number.
- Answer the medical history questions by checking 'Yes' or 'No' for each listed condition. If you respond 'Yes,' provide details in the space provided and attach any necessary medical reports.
- Fill out your family, social, and drug history clearly, including any relevant details if applicable.
- Sign and date the declaration at the bottom of Part 1, confirming the truthfulness of the information provided.
- Part 2 must be completed by a registered medical practitioner in Singapore. Arrange for a medical examination with a doctor.
- Provide your height and weight so the doctor can calculate your BMI and complete the urine analysis.
- Respond to any tests the medical practitioner may perform, including visual acuity and colour vision assessments.
- Have the doctor certify your fitness for the course by filling out the certification of fitness section. Ensure they include their name, qualifications, signature, and official stamp.
- Submit the completed form to the Student Service Centre or mail it to admissions as specified.
Once you have completed these steps, make sure to follow up if necessary, especially if your medical history requires further assessment or if the practitioner advises additional tests. Prompt submission is key to ensuring your admission process continues smoothly.
What You Should Know About This Form
What is the purpose of the Medical Singapore form?
The Medical Singapore form is used to assess a student's fitness for admission to certain courses. The completed form helps identify any medical conditions that may prevent a student from pursuing specific fields of study. It is essential for ensuring that students are aware of the physical and psychological requirements of their chosen courses.
Who is required to complete this form?
All students intending to enroll in certain courses at Singapore Polytechnic must complete the Medical Singapore form. This includes prospective students with or without pre-existing medical conditions. Additionally, the form must be verified by a medical practitioner registered in Singapore.
What happens if a student has a medical condition listed in the form?
If a student has a medical condition listed, they may be advised against pursuing their intended course. For example, those with color vision deficiency should avoid courses in fields like Chemical Engineering or Applied Chemistry. The institution may also suggest course transfers if a medical condition precludes them from successfully completing a program.
Are there any costs associated with medical examinations?
Yes, students are responsible for all medical fees, including check-ups, blood tests, and consultations with specialists if referred. The cost for the initial blood test is estimated at around S$20.00. It is crucial for students to budget for these expenses before beginning the admission process.
Can a student pursue studies if they have a history of epilepsy?
Students with a history of epilepsy are generally advised not to pursue engineering courses. Depending on individual cases, further assessments may be required to determine their eligibility for other programs. It’s recommended to communicate any medical condition that might affect course selection to the admissions office promptly.
What should international students know about medical check-ups?
All full-time international students must undergo a medical check-up, including HIV testing, as mandated by the Immigration & Checkpoints Authority (ICA). Make sure to bring both the SP Medical Report Form and the ICA Medical Examination Report Form to the clinic. Students need to collect the ICA report directly from the clinic once ready.
Common mistakes
Filling out the Medical Singapore form requires careful attention to detail. One common mistake people make is incomplete personal information. Students often forget to include all necessary details such as their NRIC or Foreign Identification number. Missing this information can lead to delays in processing the form, impacting admission timelines.
Another frequent error relates to the medical history section. Individuals may answer 'No' to some conditions when they actually have a history of them. It is crucial to provide accurate information about past medical conditions, including conditions that may seem minor. This oversight could affect eligibility for certain courses and lead to complications later.
People also tend to overlook the requirement for supporting documents. If a participant indicates they have certain medical conditions, such as Autism or Epilepsy, they need to attach relevant medical reports. Failing to do so may result in rejection of the application or additional hurdles in the admission process.
Lastly, the signature and date sections are often neglected. It is essential to sign the declaration and include the date to confirm the accuracy of the provided information. Missing a signature can render the form invalid, causing further delays in obtaining admission.
Documents used along the form
The Medical Singapore form is an essential document for students seeking admission to courses that may have specific health requirements. Along with this form, several other documents are often needed to ensure a comprehensive assessment of a student's medical fitness for their chosen course. Below is a list of these commonly used forms and documents.
- Medical Examination Report: This document provides details of the medical check-up conducted by a licensed practitioner. It includes findings from physical examinations and any recommendations regarding the student’s fitness for the course.
- HIV Medical Examination Report: Required for international students, this report confirms the results of the HIV test conducted as part of the medical check-up. It's important to fulfill the regulations set by the Immigration & Checkpoints Authority.
- Referral Letters: If a student has specific medical issues such as epilepsy or a psychiatric condition, a referral letter from a medical professional is necessary. This letter outlines the condition and the proposed follow-up actions.
- Family Medical History Form: This form collects information about the student’s family health background. It helps assess any hereditary conditions that might affect the student's health and suitability for the chosen course.
- Consent for Medical Examination: This document is signed by the student, authorizing the medical practitioner to conduct the examination and share results necessary for course admission. It ensures compliance with privacy regulations.
Having all the required documents in order not only streamlines the enrollment process but also helps ensure that students are placed in programs suited to their health needs. Always check with the admissions office for specific requirements tied to your course.
Similar forms
-
Universal Health History Form: This document, similar to the Medical Singapore form, collects a comprehensive overview of an individual's health history. Both forms inquire about medical conditions, family health history, and current medications, ensuring that essential health information is documented for proper evaluation.
-
Pre-Employment Medical Examination Form: Much like the Medical Singapore form, this document assesses a candidate's fitness for a specific role. It includes questions about medical history, physical examinations, and necessary test results that may be required by employers, especially for physically demanding positions.
-
College Athlete Medical Clearance Form: This form is also designed to gauge an individual's health before participation in sports. Similar to the Medical Singapore form, it necessitates information regarding past medical conditions, fitness assessments, and potential restrictions related to physical activities.
-
School Health Questionnaire: This document shares similarities with the Medical Singapore form in that it collects health information for students. It focuses on medical history, current health issues, and any disabilities that might affect learning or participation in school activities.
Dos and Don'ts
Things to Do When Filling Out the Medical Singapore Form:
- Read the entire form carefully before starting to fill it out.
- Provide accurate personal information including your name, NRIC or foreign identification, and contact details.
- Clearly indicate any current or past medical conditions by checking the appropriate boxes and providing details where required.
- Make sure to attach any necessary medical reports if prompted to do so.
Things to Avoid When Filling Out the Medical Singapore Form:
- Do not leave any required fields blank; ensure all sections are filled out.
- Do not provide false or misleading information as this can affect your application.
- Avoid using abbreviations or shorthand that may confuse the reader.
- Do not forget to sign and date the form; an unsigned form may not be processed.
Misconceptions
- Misconception 1: The Medical Singapore form can be reused or returned to the student.
- Misconception 2: All medical conditions disqualify a student from any course.
- Misconception 3: Disclosing a medical condition will lead to automatic denial of admission.
- Misconception 4: A student's family history is not relevant to the Medical Report.
- Misconception 5: There are no specific tests required for certain courses.
- Misconception 6: The medical check-up can only be done at specific clinics listed.
This form is a one-time document that will not be returned to the student. Once submitted, it remains with the institution for their records and assessment purposes.
While some specific medical conditions may lead to recommendations against pursuing certain courses, others do not automatically disqualify you. Each student's situation is evaluated based on the condition and the course requirements.
Providing honest information is crucial. Admission decisions are made based on the overall evaluation of a student's medical fitness in accordance with the course requirements, not solely based on disclosing a condition.
The form explicitly requests family medical history as it can help assess the student's potential health risks. Context about family health can be important in understanding an individual's medical background.
Some courses may require additional evaluations, such as sight or aptitude tests, particularly for students with disabilities. Students must be prepared for extra assessments relevant to their course of interest.
While students can choose clinics from the provided list, they also have the option to visit their preferred family doctor or any private clinic. It is essential that the medical report is submitted to the institution in a timely manner regardless of the choice of clinic.
Key takeaways
Filling out and using the Medical Singapore form is crucial for a smooth admission process. Here are some key takeaways to consider:
- Time Commitment: Expect to spend around 3 minutes completing the form.
- Confidentiality: Your information will be kept strictly confidential, only used to assess your fitness for the chosen course.
- Course Restrictions: Certain medical conditions, such as colour vision deficiency or epilepsy, may disqualify you from specific courses.
- Medical Practitioner’s Role: A registered medical practitioner in Singapore must complete part of the form, evaluating your overall health and fitness for the course.
- Interview Requirement: If you have colour vision deficiency, interviews may be necessary before admission into particular courses.
- Location of Check-ups: You can choose to go to your family doctor or to any listed clinics for your medical check-up.
- Cost Involvement: Be prepared to cover all medical charges, including any required tests and consultations with specialists.
- Important Notification: If you discover any medical issues that prevent you from pursuing your chosen course, it’s essential to notify the Admissions Office immediately.
By considering these points, you can navigate the Medical Singapore form process more effectively and ensure you meet the necessary requirements for your desired course.
Browse Other Templates
Oklahoma Ui Tax Account Number - Understand the implications of penalties for delays, which could affect overall business finances.
Ppvt-5 Score Interpretation - Feedback from this test can guide future language interventions or supports.