
Fill Out Your Medicare Part B Redetermination Form
Navigating healthcare can be a daunting task, especially when it comes to understanding the myriad of forms and procedures associated with Medicare. One crucial document in the appeals process for Medicare services is the Medicare Part B Redetermination form. This form serves as a pivotal tool for healthcare providers and beneficiaries alike, allowing them to contest decisions made regarding claims. Accuracy is paramount; each section must be meticulously filled out, as incomplete submissions may lead to dismissal of the request. It addresses specific scenarios with clear instructions, particularly for those who have received a notice indicating no appeal rights are applicable. The timeframe for submission is equally important—requests must be lodged within 120 days of the initial claim determination to ensure consideration. The form requires detailed information about the provider and the beneficiary, along with specific identifiers like the Provider Transaction Access Number and the beneficiary’s Medicare Number. Moreover, it offers a pathway to address clerical errors, such as incorrect procedure codes or billing amounts, and allows for the appeal of overpayment determinations. Additional documentation is often required to bolster the appeal. Understanding the nuances of this form can significantly impact one’s ability to secure appropriate coverage and reimbursement, underscoring the necessity of thoroughness and clarity throughout the redetermination process.
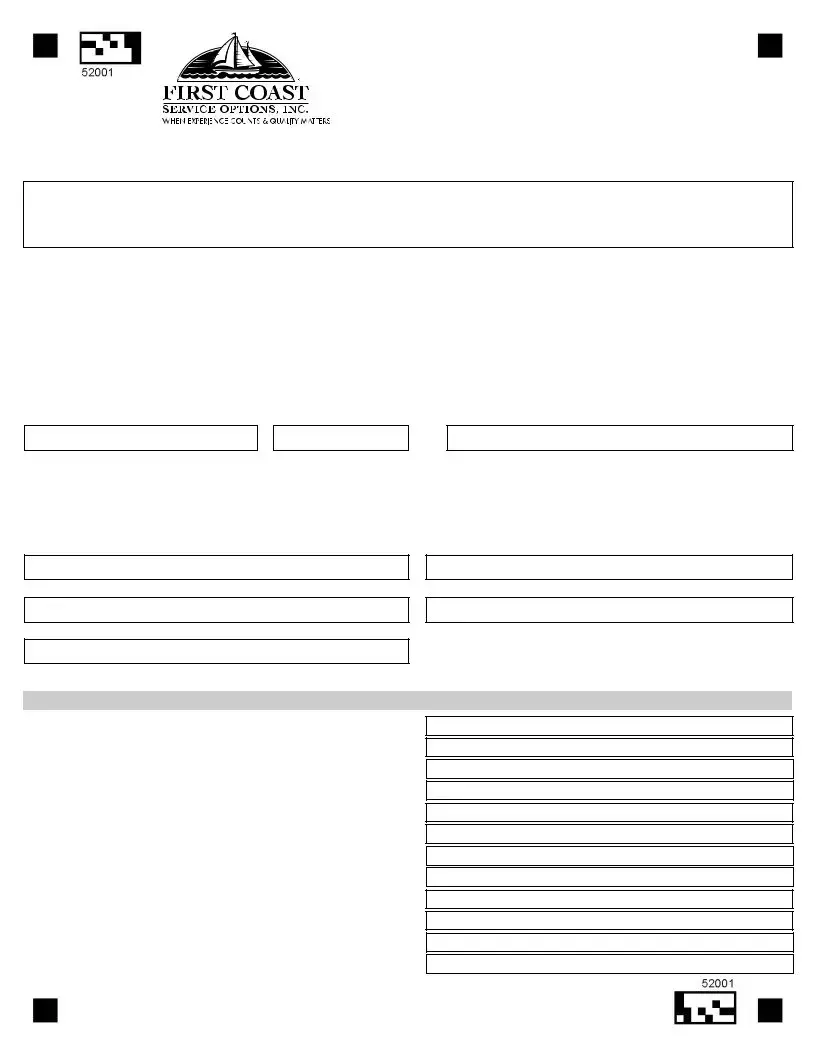
Medicare Part B Redetermination Example
Medicare Part B Redetermination and Clerical Error
Reopening Request Form
Submit Request via Fax:
*EACH FIELD OF THE FORM MUST BE FILLED OUT TO AVOID HAVING YOUR REQUEST DISMISSED
Do not complete this form for the following situation: |
Shade circles like this Not like this |
|
X |
1.If you received a message
NOTE:Requests must be filed within 120 days of original claim determination.
If this request is due to a
Please select one of the following jurisdictions and select YES or NO to the question below: __________
1. |
Does your appeal involve an overpayment decision? (Provide a copy of the overpayment letter) |
__________ |
||
2. |
Does the claim you are appealing involve Medicare Secondary Payer (MSP)? |
__________ |
||
* The following criteria must be completed in all UPPERCASE letters: |
|
|||
Provider Name |
Provider Address |
|
||
|
|
|
|
|
Provider Transaction Access Number (PTAN) |
|
Tax Identification No (last 5 digits) NPI |
|
|
Beneficiary First Name
Beneficiary Last Name
|
|
|
Beneficiary Medicare Number (11 digits) |
|
Claim Number (13 digits) |
|
|
|
Date(s) of Service
Procedure Code(s) in Question
Requestor’s Name (Printed)
Requestor’s Relationship to Provider
Telephone Number and Extension
*Please include a copy of your remittance advice notice. Request for clerical error reopening
Procedure or diagnostic code submitted incorrectly: |
Originally submitted as |
|
Correction |
Modifier omitted or submitted incorrectly: |
Originally submitted as |
|
Correction |
Provider number submitted incorrectly: |
Originally submitted as |
|
Correction |
Quantity billed submitted incorrectly: |
Originally submitted as |
|
Correction |
Billed amount submitted incorrectly: |
Originally submitted as |
|
Correction |
Zip code submitted incorrectly: |
Originally submitted as |
52001 |
Correction |
|
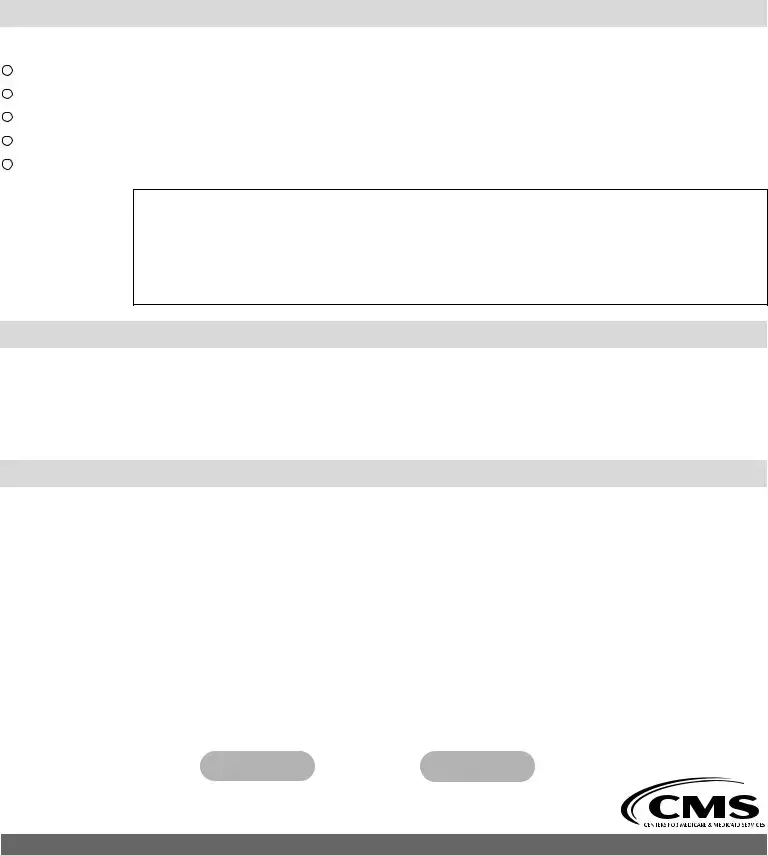
Redetermination request: Dissatisfaction with the original claim determination
The reason I disagree with the initial determination is:
This is an appeal of an overpayment request
The service was medically necessary
The service was denied as a duplicate incorrectly
The service was not overutilized
The service was denied indicating there was other insurance involvement
Additional narrative:
Please attach all pertinent documentation
q Ambulance run sheet |
q History and physical |
q Invoices for unlisted procedures and medication |
q Diagnostic test results |
q Pathology reports |
q Progress notes |
q Other medical records |
|
Improper use of this form and additional guidance
Telephone reopenings can be requested using our interactive voice response system (IVR) at
Unprocessable claims denied with remittance advice message MA130 may not be appealed. Please correct the claim and resubmit.
If the service at issue has already received a redetermination decision, do not use this form. Please use the reconsideration request form located at https://medicare.fcso.com/Forms/138073.pdf.
Appeals for durable medical equipment services (DME) must be appealed to the appropriate DME Medicare administrative contractor
Overpayments resulting from billing errors or MSP/Other Payer Involvement should be reported using the overpayment refund form located at https://medicare.fcso.com/Forms/138379.pdf.
NOTICE - Anyone who misrepresents or falsifies essential information requested by this
form may upon conviction be subject to fine and imprisonment under federal Law.
PrintReset
medicare.fcso.com
First Coast Service Options Inc.
52001
Form Characteristics
| Fact Name | Description |
|---|---|
| Submission Method | The Medicare Part B Redetermination form must be submitted via fax to 904-361-0595. |
| Field Completion | All fields of the form must be filled out to prevent dismissal of your request. |
| Claims Requiring New Submission | If you received message MA-130 on your Medicare Remittance Notice, you should submit a new claim instead of an appeal. |
| Time Limit for Requests | Requests must be filed within 120 days of the original claim determination date. |
| Overpayment Appeal Criteria | The request must indicate if it involves an overpayment decision, with a copy of the overpayment letter attached. |
| Uppercase Requirement | All specified fields must be completed in uppercase letters, including provider and beneficiary details. |
| Documentation Required | Attach all pertinent documentation, such as medical records or invoices, to support your appeal. |
| Improper Use | This form should not be used for claims that have already received a redetermination decision. |
| Consequences of Misrepresentation | Misrepresenting or falsifying any information on the form may lead to federal fines or imprisonment. |
Guidelines on Utilizing Medicare Part B Redetermination
Completing the Medicare Part B Redetermination form is an important step in addressing any issues you have with a Medicare claim. Each piece of information you provide is crucial in ensuring your request is processed correctly. Follow these steps carefully to fill out the form accurately.
- Ensure you have the most recent version of the Medicare Part B Redetermination form.
- Fill out all required fields using UPPERCASE letters. This includes the provider’s name and address, Transaction Access Number (PTAN), Tax Identification No (last 5 digits), NPI, beneficiary’s first and last name, Medicare number (11 digits), claim number (13 digits), date(s) of service, procedure code(s), requestor’s name (printed), requestor’s relationship to the provider, and telephone number with extension.
- Indicate if your appeal involves an overpayment decision. If so, provide a copy of the overpayment letter.
- Answer the question regarding whether the claim involves Medicare Secondary Payer (MSP) by selecting YES or NO.
- State the reason for the request clearly. If you are disputing the original claim determination, explain why using information like medical necessity or duplicate service denials.
- Include any pertinent documentation that supports your request. This may include ambulance run sheets, invoices, diagnostic test results, or other medical records.
- Make sure to attach a copy of your remittance advice notice to the form.
- Once complete, submit the form via fax to 904-361-0595.
After submitting the form, you can expect to receive feedback from Medicare about your appeal. Keep an eye on your mail or fax for any correspondence regarding the status of your request. If further information is needed, they will notify you directly.
What You Should Know About This Form
What is the Medicare Part B Redetermination form used for?
The Medicare Part B Redetermination form is a request to appeal an unfavorable decision related to a Medicare claim. Essentially, if you disagree with the determination made about your claim, this form allows you to provide documentation and explanations so that your case can be reviewed again. However, this is only applicable if the claim hasn't previously received a redetermination decision.
How do I properly fill out the Medicare Part B Redetermination form?
Completing the form accurately is crucial. Every single field must be filled out, and important information should be provided in uppercase letters. Make sure to include your provider name, address, transaction access number, tax identification number, National Provider Identifier (NPI), and details of the beneficiary and claim. It’s also necessary to attach a copy of your remittance advice notice as supporting documentation.
What should I do if my claim was denied with MA-130 on the remittance notice?
If you received a message MA-130 on your remittance notice, it indicates that your claim cannot be appealed or reopened. Instead, you'll need to submit a new claim that addresses the corrections needed. Be sure to review the specific issues that led to the denial to reduce the likelihood of future denials.
What types of errors can be corrected using the redetermination form?
You can request a redetermination for various clerical errors, such as incorrect procedure or diagnostic codes, errors with modifiers, and inaccuracies in billed amounts. When submitting the request, be explicit about the nature of the error and attach all pertinent documentation that supports your claim, such as invoices and medical records.
What are the consequences of misrepresenting information on this form?
It's critical to provide accurate and truthful information when filling out the Medicare Part B Redetermination form. Misrepresentation or falsification of any of the information can lead to serious legal consequences, including fines and possible imprisonment under federal law. It’s always best to be honest and thorough in your submission to avoid these repercussions.
Common mistakes
When filling out the Medicare Part B Redetermination form, it's crucial to avoid common mistakes that could result in the dismissal of your request. One major error is failing to complete every field on the form. Each required entry is vital because your request may be dismissed if even one area is left blank. Ensure that you carefully fill out all sections, such as provider details and beneficiary information, to keep your request valid.
Another mistake that frequently occurs involves the use of lowercase letters. The form explicitly states that certain criteria must be written in UPPERCASE letters. Many people overlook this instruction, erroneously submitting their information in standard text. This simple oversight can lead to unnecessary delays or rejection of the form. Paying close attention to details can make a significant difference in the processing of your request.
Additionally, individuals often neglect to include pertinent documentation alongside their redetermination request. Submitting a request without necessary supporting materials, such as a copy of the remittance advice notice, can weaken your case. Make sure to attach all requested documentation to reinforce the validity of your appeal, ensuring that you provide the necessary evidence for the reason you disagree with the original determination.
Lastly, some individuals misinterpret the conditions under which the redetermination form should be used. If a service has already received a redetermination decision, it’s important to use the reconsideration request form instead. Similarly, claims with a remittance advice message MA130 cannot be appealed; they require a different process. Understanding these guidelines can help avoid unnecessary complications.
Documents used along the form
When dealing with a Medicare Part B appeal, several additional forms and documents are often necessary alongside the Redetermination form. Collectively, these documents help to support your case and provide the necessary information to Medicare. Below is a list of key forms and documents that you may encounter during this process.
- Remittance Advice Notice: This document details the payment decisions made regarding a claim. It provides information about what was paid, denied, or adjusted and is crucial for understanding the basis of the determination.
- Overpayment Refund Form: This form is required if a provider needs to report an overpayment due to billing errors or the existence of other insurance. It serves as a formal request for a refund to Medicare.
- Reconsideration Request Form: If a redetermination has already been decided, this form must be used to further appeal the decision. It allows providers to address any disagreements formally.
- History and Physical Report: This medical document provides an overview of the patient’s medical history and physical examination. It supports claims by detailing the medical necessity of services rendered.
- Diagnostic Test Results: Results from tests performed on the patient can substantiate claims for services. This documentation is critical in demonstrating medical necessity.
- Pathology Reports: These reports are used when laboratory tests are involved. They provide clear evidence of diagnoses, which is often necessary for appeals.
- Progress Notes: Written by healthcare providers during patient visits, these notes document the patient's condition over time and justify the services provided.
- Invoice for Unlisted Procedures: If a service was provided that does not have a specific code, this invoice can offer details about the procedure and associated costs, supporting the claim.
- Ambulance Run Sheet: This record details the circumstances of ambulance service not covered under Medicare. It is useful in appealing the decision not to cover such services.
- Medical Records: Any other relevant medical records that contribute to understanding the patient's treatment and the necessity for the services in question can also be included to strengthen the appeal.
These forms and documents play a significant role in the process of appealing Medicare determinations. Ensuring that all necessary information is collected and submitted can make a substantial difference in the outcome of your appeal.
Similar forms
- Medicare Part A Redetermination Request: Similar to Part B, this form allows individuals to contest a decision made regarding Medicare Part A claims, ensuring proper documentation is submitted.
- Medicare Part B Reconsideration Request: If an initial redetermination has already been made, this form serves as a follow-up option to appeal the decision with additional evidence.
- Medicare Overpayment Refund Form: This form is used to report overpayments as a result of billing errors or other insurance involvement, much like the redetermination process deals with disputes over claims.
- Claim Adjustment Request Form: Similar in process, this document is used to request adjustments to a previously submitted Medicare claim, ensuring all details are revisited.
- Medicare Secondary Payer (MSP) Questionnaire: This form, like the redetermination request, helps gather information on other insurance involvement and can be critical for proper claims handling.
- DME Reconsideration Request: Specifically addressing durable medical equipment services, this form is used to challenge decisions made about DME claims and shares a similar purpose of dispute resolution.
- Request for Clerical Error Reopening: Focused on correcting clerical mistakes, this document shares the intent of the redetermination form by seeking resolution for mistakes that led to incorrect determinations.
Dos and Don'ts
When filling out the Medicare Part B Redetermination form, follow these essential do's and don’ts to ensure your request process goes smoothly.
- Do: Complete every field on the form. Each section requires a response to prevent dismissal.
- Do: Use UPPERCASE letters for specific information like Provider Name and Claim Number.
- Do: Include a copy of your remittance advice notice with your submission.
- Do: Submit your request within 120 days of the original determination.
- Do: Clearly state your reasons for appeal in the designated area.
- Do: Use the appropriate fax number to submit your request: 904-361-0595.
- Do: Attach any relevant supporting documents, such as medical records or invoices.
- Don't: Use this form if your claim has already received a redetermination decision.
- Don't: Attempt to appeal claims denied with the MA130 message; correct and resubmit the claim instead.
- Don't: Forget to include your Tax Identification Number and NPI.
- Don't: Leave any fields blank, as this can lead to a rejection of your request.
- Don't: Use misleading information; misrepresentation can lead to serious legal consequences.
- Don't: Submit requests for durable medical equipment appeals using this form; follow DME-MAC procedures instead.
- Don't: Request telephone reopenings if you can submit a written redetermination request.
Following these guidelines will help streamline your redetermination process and improve your chances of a favorable outcome. Stay organized, and good luck with your appeal!
Misconceptions
Misconceptions about the Medicare Part B Redetermination form can lead to confusion. Here are eight common misunderstandings clarified:
- Filing the form guarantees appeal approval: Submitting the redetermination form does not ensure that the appeal will be accepted or that the initial decision will be overturned.
- Only physicians can submit a redetermination request: Any authorized representative, including billing staff, can submit the form on behalf of the provider.
- The form can be used for any denial: This form is specifically for Medicare Part B claims. It cannot be used for claims denied under other programs or for certain error types.
- Submitting the request late is acceptable: Requests must be filed within 120 days of the original claim determination. Late submissions are typically not considered.
- Information can be submitted in lowercase: All required fields on the form must be filled out in uppercase letters to ensure proper processing.
- Only one reason can be provided for the appeal: Multiple reasons for dissatisfaction can be included in the relevant section of the form.
- All claims can be appealed: Claims with the remittance advice message MA-130 cannot be appealed. They must be corrected and resubmitted as new claims.
- Personal information can be omitted: Failing to provide complete and accurate information, including the provider's and beneficiary's details, may result in dismissal of the request.
Understanding these points can help streamline the redetermination process and mitigate potential errors in submission.
Key takeaways
Understanding the Medicare Part B Redetermination Form is crucial for ensuring that your claims are processed correctly and efficiently. Here are some key takeaways to keep in mind when filling out and submitting this form:
- Make sure all fields of the form are completed. Incomplete submissions can lead to your request being dismissed.
- This form should not be used if you received a message MA-130 on your Medicare Remittance Notice. In such cases, you need to submit a new claim instead.
- Be aware of the 120-day timeframe for filing a request based on the original claim determination. Timeliness is essential for a successful appeal.
- It is necessary to include all relevant documentation, such as remittance advice notices and any other pertinent medical records, to support your claim.
Filing the form correctly and understanding the requirements can significantly influence the outcome of your appeal. Always double-check your entries and ensure that you meet all outlined criteria.
Browse Other Templates
Af422 - Specify whether overseas assignment clearance is appropriate for the patient.
How Much Can I Claim for Child Care Expenses - Provide the mother's occupation for school records.
Da Form 3072-2 - The applicant should ensure all debts and income sources are verifiable.