Fill Out Your Memorial Hermann Release Form
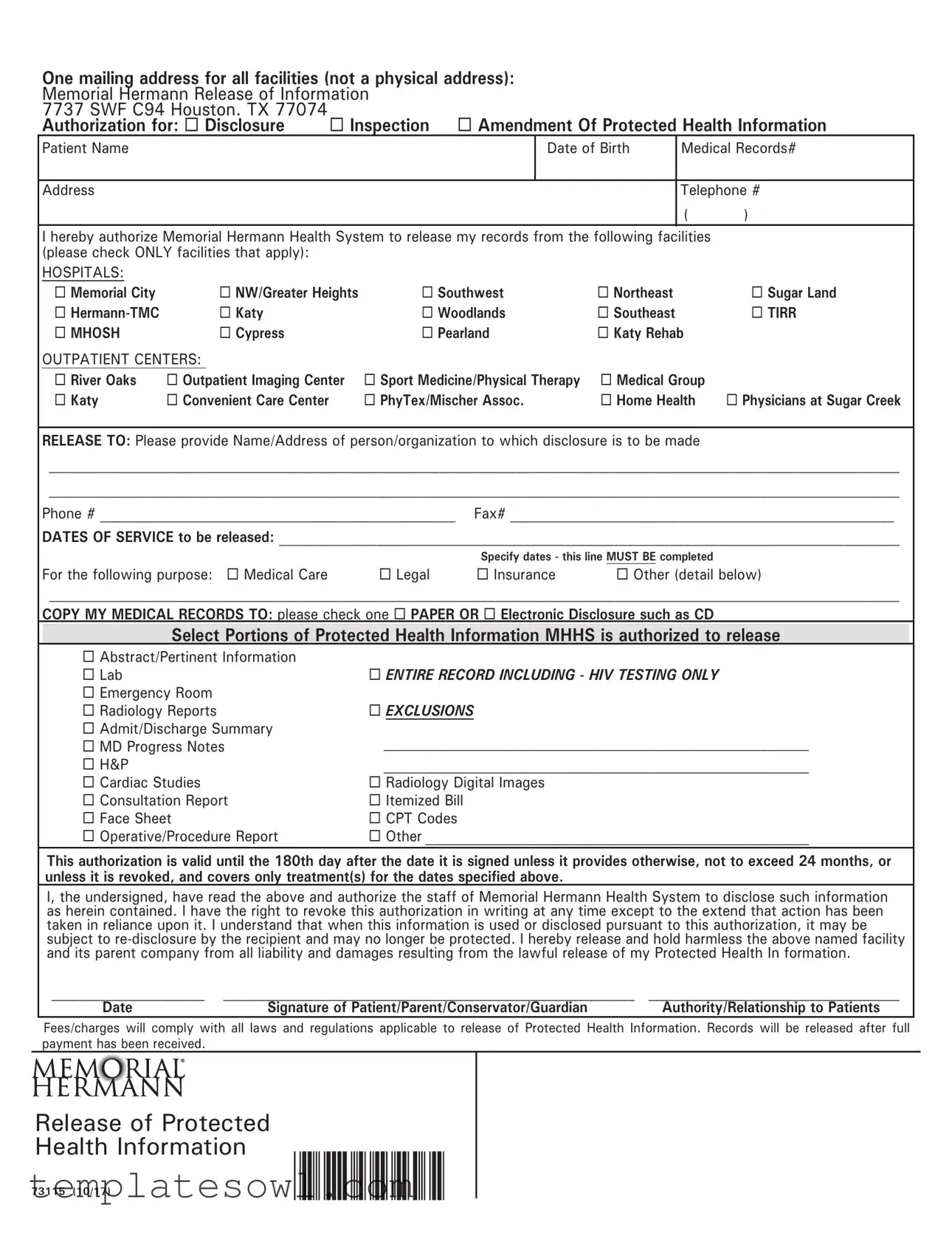
The Memorial Hermann Release form is an essential document that allows patients to authorize the sharing of their medical information with designated individuals or organizations. This form provides various options for patients to specify which records they wish to disclose, such as lab results, progress notes, or entire medical histories, and it includes a list of facilities from which records can be obtained, covering multiple locations within the Memorial Hermann Health System. Patients fill out their personal information, including name, date of birth, and contact details, alongside the specific dates of service relevant to their request. They also have the option to indicate the purpose of the disclosure, whether for medical care, legal reasons, insurance, or other needs. When completing the form, a patient can choose to receive copies of their medical records in either paper format or electronically, such as on a CD. Importantly, the authorization granted through this form remains valid for up to 180 days unless revoked earlier or specified otherwise, ensuring that patients have control over their protected health information. Additionally, the document includes a statement releasing Memorial Hermann from liability related to the lawful release of health information, reinforcing the patient's understanding of the potential risks associated with sharing their medical records.
Memorial Hermann Release Example
One mailing address for all facilities (not a physical address): |
|
|
|
||||
Memorial Hermann Release of Information |
|
|
|
||||
7737 SWF C94 Houston. TX 77074 |
Inspection Amendment Of Protected Health Information |
||||||
Authorization for: Disclosure |
|||||||
Patient Name |
|
|
|
Date of Birth |
Medical Records# |
||
|
|
|
|
|
|
|
|
Address |
|
|
|
|
|
Telephone # |
|
|
|
|
|
|
|
( |
) |
I hereby authorize Memorial Hermann Health System to release my records from the following facilities |
|
||||||
(please check ONLY facilities that apply): |
|
|
|
|
|
|
|
HOSPITALS: |
|
|
|
|
|
|
|
Memorial City |
NW/Greater Heights |
Southwest |
Northeast |
|
Sugar Land |
||
|
Katy |
|
Woodlands |
Southeast |
|
TIRR |
|
MHOSH |
Cypress |
|
Pearland |
Katy Rehab |
|
||
OUTPATIENT CENTERS: |
|
|
|
|
|
|
|
River Oaks |
Outpatient Imaging Center |
Sport Medicine/Physical Therapy |
Medical Group |
|
|||
Katy |
Convenient Care Center |
|
PhyTex/Mischer Assoc. |
Home Health |
Physicians at Sugar Creek |
||
RELEASE TO: Please provide Name/Address of person/organization to which disclosure is to be made
__________________________________________________________________________________________________________________________
__________________________________________________________________________________________________________________________
Phone # ___________________________________________________ Fax# _______________________________________________________
DATES OF SERVICE to be released: _________________________________________________________________________________________
|
|
Specify dates - this line MUST BE completed |
|
For the following purpose: Medical Care |
Legal |
Insurance |
Other (detail below) |
__________________________________________________________________________________________________________________________
COPY MY MEDICAL RECORDS TO: please check one PAPER OR Electronic Disclosure such as CD
Select Portions of Protected Health Information MHHS is authorized to release
Abstract/Pertinent Information |
|
Lab |
ENTIRE RECORD INCLUDING - HIV TESTING ONLY |
Emergency Room |
|
Radiology Reports |
EXCLUSIONS |
Admit/Discharge Summary |
_____________________________________________________________ |
MD Progress Notes |
|
H&P |
_____________________________________________________________ |
Cardiac Studies |
Radiology Digital Images |
Consultation Report |
Itemized Bill |
Face Sheet |
CPT Codes |
Operative/Procedure Report |
Other _______________________________________________________ |
This authorization is valid until the 180th day after the date it is signed unless it provides otherwise, not to exceed 24 months, or
unless it is revoked, and covers only treatment(s) for the dates specified above.
I, the undersigned, have read the above and authorize the staff of Memorial Hermann Health System to disclose such information as herein contained. I have the right to revoke this authorization in writing at any time except to the extend that action has been taken in reliance upon it. I understand that when this information is used or disclosed pursuant to this authorization, it may be subject to
______________________ |
___________________________________________________________ |
____________________________________ |
Date |
Signature of Patient/Parent/Conservator/Guardian |
Authority/Relationship to Patients |
Fees/charges will comply with all laws and regulations applicable to release of Protected Health Information. Records will be released after full payment has been received.
Release of Protected
Health Information
73115 (10/17)
Form Characteristics
| Fact Name | Description |
|---|---|
| Mailing Address | The form can be sent to Memorial Hermann Release of Information, 7737 SWF C94, Houston, TX 77074. |
| Purpose of Release | Patients can authorize the release of their medical records for various purposes, including medical care, legal, and insurance needs. |
| Record Access | Patients can request inspection or amendment of their protected health information through this form. |
| Valid Duration | This authorization lasts for 180 days after signing unless specified otherwise, not exceeding 24 months. |
| Disclosure Options | Patients can choose to receive their medical records on paper or electronically, such as via a CD. |
| Facilities Listed | The form lists various Memorial Hermann facilities where records can be released, including hospitals and outpatient centers. |
| Authorization Revocation | Patients have the right to revoke the authorization in writing, except if action has already been taken based on it. |
| Fees and Charges | All fees for the release comply with applicable laws and regulations and must be paid prior to record release. |
| Liability Release | Patients release Memorial Hermann and its affiliates from any liability associated with the lawful release of information. |
| Protected Health Information | The form allows for selective disclosure of different types of medical records, including lab results and progress notes. |
Guidelines on Utilizing Memorial Hermann Release
Once you have completed the Memorial Hermann Release form, the next step is to submit it to the appropriate mailing address provided in the instructions. Make sure that all fields are filled out accurately to avoid any delays in processing your request.
- Start by filling in your Patient Name at the top of the form.
- Enter your Date of Birth in the designated space.
- Complete the Medical Records # if you have one; otherwise, leave it blank.
- Provide your current Address and Telephone Number.
- Check the appropriate boxes for either Inspection or Amendment of Protected Health Information.
- Select facilities from the list of Hospitals by checking all that apply.
- If applicable, choose any Outpatient Centers by checking the relevant boxes.
- Fill out the Release To section, including the name and address of the person or organization receiving the information.
- Write down their Phone Number and Fax Number if available.
- Specify the DATES OF SERVICE you want to be released.
- Select a purpose for the request by checking the appropriate box: Medical Care, Legal, Insurance, or Other with details.
- Indicate how you want your records to be delivered by checking either PAPER or Electronic.
- Choose which Portions of Protected Health Information you want to be released by checking the relevant boxes.
- Read the authorization statement at the bottom of the form and sign it, providing your Date and Authority/Relationship to Patient if necessary.
What You Should Know About This Form
What is the Memorial Hermann Release form?
The Memorial Hermann Release form is a document that allows patients to authorize the release of their protected health information from the Memorial Hermann Health System. This form is essential for patients who wish to share their medical records with specific individuals or organizations for various purposes, such as medical care, legal reasons, or insurance claims.
How do I fill out the Memorial Hermann Release form?
To complete the form, start by providing your name, date of birth, address, and telephone number. Next, indicate which facilities from the Memorial Hermann network you authorize to release your information. Specify the dates of service for which you are requesting records and indicate the purpose of the disclosure. Finally, select the format in which you would like to receive your records, whether on paper or electronically, and sign the form.
What types of information can be released?
You can authorize the release of various types of medical information, including lab results, progress notes, radiology reports, and entire medical records. You also have the option to specify exclusions if there are particular records you do not wish to be disclosed. Make sure to check the relevant boxes on the form to include only the information you want released.
How long is the authorization valid?
The authorization provided through the Memorial Hermann Release form remains valid for up to 180 days after your signature, unless otherwise specified. It can extend up to 24 months, but you have the right to revoke it at any time in writing. The authorization will only cover treatment received during the specified dates you list on the form.
What should I do if I want to revoke my authorization?
If you decide to revoke your authorization, you must do so in writing. It's essential to understand that revocation will only take effect after the notice is received. Additionally, if any actions have already been taken based on the original authorization, those actions will not be impacted by your revocation.
Are there any fees associated with the release of my medical records?
Yes, fees may apply when requesting the release of your medical records. These charges will comply with all applicable laws and regulations governing the release of protected health information. Records will be released only after full payment has been received.
What are the risks of disclosing my protected health information?
When you authorize the release of your protected health information, there's a risk that this information may be re-disclosed by the recipient, which means it may lose its protection under federal regulations. You should carefully consider the recipient and purpose of the disclosure before proceeding.
Common mistakes
When filling out the Memorial Hermann Release form, many people inadvertently make errors that can lead to delays or complications in obtaining medical records. Understanding these common mistakes can help ensure a smoother process.
One frequent mistake is failing to specify the dates of service accurately. This section must be completed in detail. Without precise dates, the medical facility may not know which records to release. Be sure to indicate the specific time frame for which you are requesting records. If this line is left blank, the request may not be processed as intended.
Another issue arises when individuals neglect to check all applicable boxes for the facilities from which they are requesting records. It's essential to review the list carefully and select every relevant hospital or outpatient center. Omitting a facility can lead to incomplete records, which may not fully meet your needs.
People often overlook the need to provide detailed information about the person or organization to whom the records will be released. The release to section must include an accurate name and address. This step is crucial, as it directs where the information should be sent. Failing to fill this out or making errors in the contact details can result in an unnecessary back-and-forth with the health system.
Lastly, many who fill out the form underestimate the importance of choosing the correct format for receiving records. There are options for PAPER or Electronic copies. Choosing the format that best suits your needs can save time and ensure you receive the information in a way that is most convenient for you. Choosing a format that doesn't align with your preferences can lead to frustration and potential delays.
Documents used along the form
The Memorial Hermann Release form facilitates the transfer of medical records from various facilities within the Memorial Hermann Health System. However, it is often accompanied by additional documents that support the proper handling of medical information. Each of these forms serves a specific purpose in ensuring that patient data is released securely and in compliance with applicable regulations.
- Patient Authorization Form: This document outlines the patient's consent to share their medical information. It specifies who is permitted to access the records and for what purpose, emphasizing the patient's control over their personal health data.
- Insurance Claim Form: This form is commonly used when patients seek reimbursement from their health insurance providers. It details the medical services received and helps validate the need for treatment under the insurance policy.
- Medical Records Transfer Request: With this document, a patient requests the transfer of their records from one healthcare provider to another. It often includes fields that capture essential patient details and the healthcare providers involved.
- Patient Information Update Form: When patients move or change contact details, this form allows them to update their information in the healthcare provider's system. Accurate information is vital for effective communication and service delivery.
- Notice of Privacy Practices: This document explains how a healthcare provider collects, uses, and protects a patient's medical information. It ensures that patients are aware of their rights concerning their health records.
- Authorization for Release of Mental Health Records: This specialized authorization is necessary when disclosing sensitive mental health information. It reflects the heightened privacy considerations surrounding mental health treatment.
Together, these documents complement the Memorial Hermann Release form, assisting patients in managing their health information effectively. Each form plays an integral role in the broader context of patient rights and information privacy, ensuring that individuals have agency over their medical records.
Similar forms
When looking at the Memorial Hermann Release form, you may find that it shares similarities with several other important documents used in healthcare and legal contexts. Here are four such documents:
- HIPAA Release Form: Much like the Memorial Hermann Release form, the HIPAA release form authorizes the sharing of your protected health information (PHI) with specific individuals or organizations. Both forms require your explicit consent and detail the type of information being shared, ensuring your rights and privacy are respected.
- Medical Records Request Form: This document is similar in that it allows you to request your own medical records. Just as the Memorial Hermann Release form requires you to specify the records you want, a Medical Records Request Form often asks which portions of your health information you wish to access or give consent to share.
- Power of Attorney for Healthcare: This document grants someone else the authority to make healthcare decisions on your behalf. In both cases, the individual (or agent) needs to be specified. The Memorial Hermann form allows you to designate who can receive your records, while a Power of Attorney outlines who can make decisions regarding your medical care.
- Informed Consent Form: Often used before medical procedures, this form ensures that patients understand what they are agreeing to when receiving treatment. Like the Memorial Hermann Release form, it typically requires a signature and indicates that the patient has been informed about what information is being shared and what implications it may have.
Understanding how these documents relate to the Memorial Hermann Release form can empower you to make informed decisions regarding your health information. Each serves a specific purpose but centers on ensuring your rights are maintained while facilitating necessary communication in the healthcare system.
Dos and Don'ts
When filling out the Memorial Hermann Release form, accuracy and attention to detail are crucial. Here are some important dos and don'ts to keep in mind:
- Do use the correct mailing address:
- Do fill in all required fields:
- Do specify the purpose of the record release:
- Do indicate the dates of service:
- Do choose the format for receiving records:
- Don't leave any sections blank:
- Don't check multiple facilities without clarity:
- Don't overlook the expiration date of the authorization:
- Don't forget your signature:
Ensure you send the form to Memorial Hermann Release of Information at 7737 SWF C94 Houston, TX 77074.
Provide your name, date of birth, and contact information to avoid delays in processing.
Select the appropriate reason, such as medical care or legal needs.
Be sure to specify the dates for which you want records released. This is a mandatory field.
Select whether you prefer your records in paper or electronic format.
Incomplete forms can lead to processing delays. Make sure every section is filled out.
Only check the facilities from which you want records, and ensure it’s clearly marked.
Remember that the authorization is valid for 180 days unless otherwise stated.
Ensure the form is signed by you or your legal representative to confirm authorization.
By following these guidelines, you can ensure your experience with the Memorial Hermann Release form goes smoothly.
Misconceptions
Below are eight common misconceptions about the Memorial Hermann Release form:
- Anyone can request records. Only the patient or authorized representatives can request medical records with this form.
- All facilities are automatically included. Patients must specifically check which facilities’ records they wish to release.
- The authorization lasts indefinitely. The authorization is valid for up to 180 days and does not exceed 24 months unless specified.
- Fees for records are a surprise. Patients are informed that fees will comply with laws and regulations prior to the release.
- Records can be sent anywhere. Patients must fill out the recipient’s name and address to direct where records are sent.
- All medical information will be released. Patients can choose specific portions of their health information to disclose.
- Revoking authorization is impossible. Patients have the right to revoke authorization in writing, except when action has already been taken.
- Disclosures are secure. While protections exist, patients should be aware that information could be re-disclosed by the recipient.
Key takeaways
Here are some important points to consider when filling out and using the Memorial Hermann Release form:
- Single Mailing Address: Use the designated mailing address: Memorial Hermann Release of Information, 7737 SWF C94, Houston, TX 77074, for all facilities.
- Choose Your Purpose: Clearly indicate your purpose for the release, such as Medical Care, Legal, or Insurance.
- Fill in Required Information: Provide your name, date of birth, and contact information accurately for proper identification.
- Select Applicable Facilities: Check only the facilities from which you want your medical records released.
- Specify Dates of Service: Fill in the specific dates for which you are requesting records.
- Define the Recipient: Clearly write the name and address of the person or organization that will receive your records.
- Formatting of Disclosure: Choose whether you want the records in paper or electronic format.
- Portions of Records: Decide which portions of your health information you want released, including any exclusions if necessary.
- Authorization Validity: Remember, the authorization is valid for 180 days unless otherwise specified, not to exceed 24 months.
- Right to Revoke: You have the right to revoke this authorization at any time in writing.
Follow these guidelines carefully to ensure that your medical records are released without complications.
Browse Other Templates
Who Has the Right to Change a Life Insurance Policy's Beneficiary - Using precise language when naming beneficiaries can prevent potential confusion during claims.
Ftios - Utilizing this form can aid in avoiding unnecessary penalties or taxes during transfers.