Fill Out Your Michigan Dhs 4574 Form
The Michigan DHS 4574 form plays a critical role in providing health care coverage for individuals residing in nursing facilities. This application is designed for patients who require assistance in navigating the often complex process of obtaining health care benefits. Completing the form accurately is essential, as the information provided will determine eligibility for coverage. The Michigan Department of Health and Human Services (MDHHS) is committed to ensuring that individuals receive help in filling out the application if needed. The form also includes sections for beneficiaries to declare their assets, a key component in assessing financial eligibility. Understanding the nuances of this application can make a significant difference in securing vital health care resources. It is important to remember that assistance is available; individuals can contact their case specialists or the MDHHS office for support. Additionally, language barriers are addressed, as the department can provide interpreters at no cost, ensuring that all applicants have the opportunity to communicate their needs effectively. Ultimately, the DHS 4574 form serves as a gateway to essential health services for nursing facility patients, making its proper completion a priority for those seeking assistance.
Michigan Dhs 4574 Example

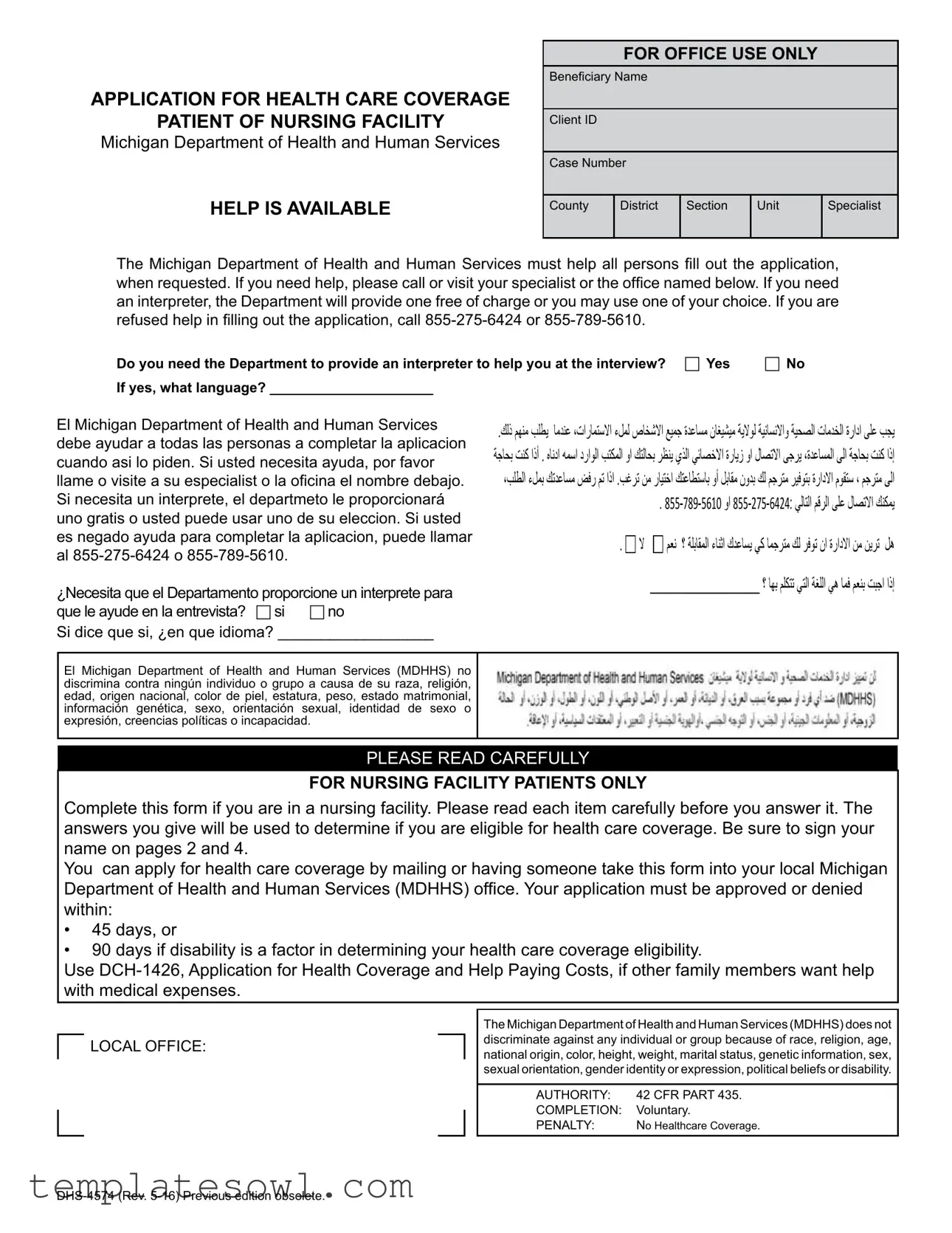
APPLICATION FOR HEALTH CARE COVERAGE
PATIENT OF NURSING FACILITY
Michigan Department of Health and Human Services
HELP IS AVAILABLE
FOR OFFICE USE ONLY
Beneiciary Name
Client ID
Case Number
County |
District |
Section |
Unit |
Specialist |
|
|
|
|
|
The Michigan Department of Health and Human Services must help all persons ill out the application, when requested. If you need help, please call or visit your specialist or the ofice named below. If you need an interpreter, the Department will provide one free of charge or you may use one of your choice. If you are refused help in illing out the application, call
Do you need the Department to provide an interpreter to help you at the interview? c Yes |
c No |
If yes, what language? _____________________ |
|
El Michigan Department of Health and Human Services debe ayudar a todas las personas a completar la aplicacion cuando asi lo piden. Si usted necesita ayuda, por favor llame o visite a su especialist o la oicina el nombre debajo. Si necesita un interprete, el departmeto le proporcionará
uno gratis o usted puede usar uno de su eleccion. Si usted es negado ayuda para completar la aplicacion, puede llamar al
¿Necesita que el Departamento proporcione un interprete para que le ayude en la entrevista? c si c no
Si dice que si, ¿en que idioma? __________________
.ﻚﻟذ ﻢﮭﻨﻣ ﺐﻠﻄﯾ ﺎﻣﺪﻨﻋ ،تارﺎﻤﺘﺳﻻا ءﻞﻤﻟ صﺎﺨﺷﻻا ﻊﯿﻤﺟ ةﺪﻋﺎﺴﻣ نﺎﻐﯿﺸﯿﻣ ﺔﯾﻻﻮﻟ ﺔﯿﻧﺎﺴﻧﻻاو ﺔﯿﺤﺼﻟا تﺎﻣﺪﺨﻟا ةرادا ﻰﻠﻋ ﺐﺠﯾ ﺔﺟﺎﺤﺑ ﺖﻨﻛ اذأ . هﺎﻧدا ﮫﻤﺳا دراﻮﻟا ﺐﺘﻜﻤﻟا وا ﻚﺘﻟﺎﺤﺑ ﺮﻈﻨﯾ يﺬﻟا ﻲﺋﺎﺼﺧﻻا ةرﺎﯾز وا لﺎﺼﺗﻻا ﻰﺟﺮﯾ ،ةﺪﻋﺎﺴﻤﻟا ﻰﻟا ﺔﺟﺎﺤﺑ ﺖﻨﻛ اذإ ،ﺐﻠﻄﻟا ءﻞﻤﺑ ﻚﺗﺪﻋﺎﺴﻣ ﺾﻓر ﻢﺗ اذا .ﺐﻏﺮﺗ ﻦﻣ رﺎﯿﺘﺧا ﻚﺘﻋﺎﻄﺘﺳﺎﺑ وأ ﻞﺑﺎﻘﻣ نوﺪﺑ ﻚﻟ ﻢﺟﺮﺘﻣ ﺮﯿﻓﻮﺘﺑ ةرادﻻا مﻮﻘﺘﺳ ، ﻢﺟﺮﺘﻣ ﻰﻟا
.
. |
|
ﻻ |
|
|
ﻢﻌﻧ ؟ ﺔﻠﺑﺎﻘﻤﻟا ءﺎﻨﺛا كﺪﻋﺎﺴﯾ ﻲﻛ ﺎﻤﺟﺮﺘﻣ ﻚﻟ ﺮﻓﻮﺗ نا ةرادﻻا ﻦﻣ ﻦﯾﺮﺗ ﻞھ |
|
|
|
|||
|
|
|
____________________ ؟ ﺎﮭﺑ ﻢﻠﻜﺘﺗ ﻲﺘﻟا ﺔﻐﻠﻟا ﻲھ ﺎﻤﻓ ﻢﻌﻨﺑ ﺖﺒﺟا اذإ |
||
El Michigan Department of Health and Human Services (MDHHS) no discrimina contra ningún individuo o grupo a causa de su raza, religión, edad, origen nacional, color de piel, estatura, peso, estado matrimonial, información genética, sexo, orientación sexual, identidad de sexo o expresión, creencias políticas o incapacidad.
PLEASE READ CAREFULLY
FOR NURSING FACILITY PATIENTS ONLY
Complete this form if you are in a nursing facility. Please read each item carefully before you answer it. The answers you give will be used to determine if you are eligible for health care coverage. Be sure to sign your name on pages 2 and 4.
You can apply for health care coverage by mailing or having someone take this form into your local Michigan Department of Health and Human Services (MDHHS) ofice. Your application must be approved or denied
within:
•45 days, or
•90 days if disability is a factor in determining your health care coverage eligibility.
Use
LOCAL OFFICE:
The Michigan Department of Health and Human Services (MDHHS) does not discriminate against any individual or group because of race, religion, age, national origin, color, height, weight, marital status, genetic information, sex, sexual orientation, gender identity or expression, political beliefs or disability.
AUTHORITY: |
42 CFR PART 435. |
COMPLETION: |
Voluntary. |
PENALTY: |
No Healthcare Coverage. |
FOR OFFICE USE ONLY
NOTES
FOR OFFICE USE ONLY
NOTES
FOR OFFICE USE ONLY
NOTES
ASSETS DECLARATION
PATIENT AND SPOUSE
Michigan Department of Health and Human Services
(Skip if no spouse)
FOR OFFICE USE ONLY
Beneiciary Name
Client ID
Case Number
County |
District |
Section |
Unit |
Specialist |
|
|
|
|
|
PLEASE PRINT
Patient’s Name (First, Middle, Last) |
Phone No. of Nursing Home |
Spouse’s Name (First, Middle, Last) |
Spouse’s Phone No. |
|||
|
|
|
|
|
|
|
Address of Nursing Home (Number, Street, Rural Route) |
|
Spouse’s Address (Number, Street, Rural Route) |
|
|||
|
|
|
|
|
|
|
City |
State |
|
Zip Code |
City |
State |
Zip Code |
|
|
|
|
|
|
|
Patient’s Birthdate (Mo/Day/Yr) |
Patient’s Social Security |
Spouse’s Birthdate (Mo/Day/Yr |
Spouse’s Social Security* |
|||
|
|
|
|
|
|
|
This form asks questions about the property or assets owned by you and/or your spouse. This information is needed to determine your eligibility for Healthcare Coverage and the amount of assets that can be protected for the beneit of your spouse. Answer the following questions by providing information about all assets owned by you and/or your spouse as of _________________________.
Include assets you or your spouse own jointly with family or other persons.
ASSETS
1. Do you and/or your spouse have any assets (include assets held jointly)? |
|
|
c Yes |
4Check all types of assets your household has and complete the table |
c No |
c c c
Checking/draft account Certiicates of Deposit (CD)
Case on hand or in safe deposit
c c c
Money market accounts Christmas club accounts
Savings, bonds, stocks or mutual funds
c c c
Savings/share accounts
Patient trust fund
IRA, KEOGH, 401K or Deferred
Compensation account(s)
c Trust or Annuity |
c Land contract, mortgage or other |
|
notes payable to household member |
cReal estate (including place you live)
c c c
Life estate/life lease |
|
c Burial plot(s), casket, etc. |
|
c Tools, equipment, livestock or crops |
||||
Life insurance |
|
c Other Assets ___________________ |
c Health Savings Account |
|||||
Burial trust/funeral contract(s) |
|
|
|
|
|
|
|
|
|
Type(s) |
|
|
Name and address |
|
Account/policy |
||
Owner(s) |
|
|
Balance |
|
||||
of asset(s) |
|
of Asset(s) |
|
amount of value |
(bank, insurance company, etc.) |
|
number, etc. |
|
|
|
|
|
|
|
|
|
|
|
|
The Michigan Department of Health and Human Services (MDHHS) does not |
AUTHORITY: |
42 CFR Part 435. |
discriminate against any individual or group because of race, religion, age, |
COMPLETION: |
Voluntary. |
national origin, color, height, weight, marital status, genetic information, sex, |
PENALTY: |
No Healthcare Coverage. |
sexual orientation, gender identity or expression, political beliefs or disability. |
*Optional if the community spouse is not requesting assistance.
1 |
ASSETS
2. Does anyone in your household have any vehicles?
c Yes |
4Check all types of assets your household has and complete the table |
c No |
c Car |
c Truck c Boat |
Owner(s)
(As shown on vehicle title
or registration)
c Camper/trailer |
c Motorcycle |
c RV |
c Other Vehicle |
Year |
Make/Model |
Amount Owed |
|
|
|
3. Has anyone in your household:
•sold or given away property, land, vehicles, stocks, bonds, savings, cash, checking, income, etc., closed any accounts or removed or added a name on any asset within the last 60 months?
•iled a pending lawsuit which may bring money, property, etc.?
•received a
•or has anyone acting for any household member, ever put any money, lawsuit settlement, income or assets in a trust, annuity or similar legal device?
c Yes 4Who:
cNo
cYes 4Who:
cNo
cYes 4Who:
cNo
cYes 4Who:
cNo
AFFIDAVIT
I swear or afirm that all the information that I have written on this form or told to a specialist is true. I understand that I can be prosecuted for perjury if I have intentionally given false information. I also know that I may be asked to show proof of any information I have given. I also know that if I have intentionally left out any information or if I have given false information, which causes me to receive assistance I am not entitled to or more assistance than I am entitled to, I can be prosecuted for fraud.
Estate Recovery. I understand that upon my death the Michigan Department of Health and Human Services (MDHHS) has the legal right to seek recovery from my estate for services paid by Healthcare Coverage. This means that some or all of my estate may be recovered. MDHHS will not seek to recover against the estate while there is a legal surviving spouse or a legal surviving child who is under the age of 21, blind, or disabled. An estate consists of real and personal property. If you have received an asset disregard due to a
Signature (Patient or Representative)
Date (Month, Day, Year)
Two Witnesses Only If Signed by Mark X
Signature of First Witness
Signature of Second Witness
NOTE: If you signed this application on behalf of someone else, complete the information below.
Name (First, Middle, Last)
Phone Number
Relationship to Patient
Street Address
City
State
Zip Code
2 |

Note: This application requests information about the patient in the nursing facility.
The words “You” and “Your” refer to the patient.
1. |
Patient’s Name (First, Middle, Last) |
|
|
|
|
2. |
Name of Nursing Facility |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3. Address of Nursing Facility |
|
|
|
|
|
|
City |
|
State |
Zip Code |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. |
Phone No. of Nursing Facility |
|
5. County |
|
6. |
Birthdate |
7. Sex |
|
8. Social Security Number |
||||
|
|
|
|
|
|
|
|
|
|
|
|
||
9. |
Marital Status: c Never married |
|
c Married |
c Separated c Divorced |
c Widowed |
|
|||||||
10. Date of Nursing Facility Admission |
|
11. Address where you lived before you entered the nursing facility |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
12.If married, tell us about your spouse and all persons living with your spouse. If not married, tell us about your children under age 18 living in your home.
Name |
Date of Birth |
Social Security Number* |
Relationship to you |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
If you have a |
|
|
|||||
|
|
|
|
|
|
||
13. Name of Guardian/Conservator |
|
Phone Number |
|
Do you pay guardian/conservator |
|||
|
|
|
|
|
expenses? |
c YES |
c NO |
|
|
|
|
|
|
|
|
Guardian’s/Conservator’s Address |
|
|
|
City |
State |
Zip Code |
|
|
|
|
|
|
|
|
|
YES NO
14.Have you ever applied for or received
assistance in Michigan? |
c |
c |
15.Have you received money or beneits such
as Medical Assistance from another state in the last 30 days?
c c
21.Do you have unpaid medical expenses for services provided in the last 3 months?
22.Do you pay health insurance premiums?
23.Do you have Medicare Coverage? Do you need help paying premiums?
YES NO
c c
c c
c c
c c
16. |
Are you a U.S. citizen or U.S. national? |
c |
c |
24. |
Are you covered by a health, hospital, or |
17. |
If you are not a U.S. citizen or U.S. national, do you have |
|
|||
|
covered in the last 3 months? |
||||
|
eligible immigration status? If Yes: |
|
|
|
|
|
|
|
25. Has a court ordered anyone to pay your |
||
|
a. Immigration document type ______________ |
|
|||
|
b. Document ID number ___________________ |
|
|
medical expenses or provide health |
|
|
c. Have you lived in the U.S. since 1996? |
c |
c |
|
insurance for you? |
|
d. Are you, or your spouse or parent a veteran or an |
|
26. |
Have you had an accident or |
|
|
c |
c |
|||
|
|
illness or injury resulting in medical costs |
|||
|
e. U.S. entry date ______________________ |
|
|
||
|
|
|
that may be paid by another person or an |
||
18. |
Enter your racial heritage from codes below. If you are |
|
|
insurance company? |
|
|
|
|
|||
|
multiracial, enter all the codes that apply (answering |
|
|
|
|
|
is voluntary) I = American Indian, A = Alaskan Native, |
|
27. |
Have you set up a plan or entered into a |
|
|
S = Asian, B = Black or African American, |
P = Native |
|
||
|
|
|
contract, such as a life care contract, that |
||
|
Hawaiian or Other Paciic Islander, W = White |
|
|
||
|
|
|
will pay for your medical care? |
||
|
_____________________________ |
|
|
|
|
|
|
|
|
|
|
19. |
Check the box if you are Hispanic or |
|
|
28. Is there a plan for you to return home |
|
|
Latino (answering is voluntary). |
c |
|
|
within six months from the date of |
|
|
|
|
|
admittance? |
20. |
Are you a veteran or the spouse, |
c |
c |
|
|
|
dependent or parent of a veteran? |
|
|
||
*Optional if the community spouse and/or children are not applying for Healthcare Coverage.
c c
c c
c c
c c
c c
3 |
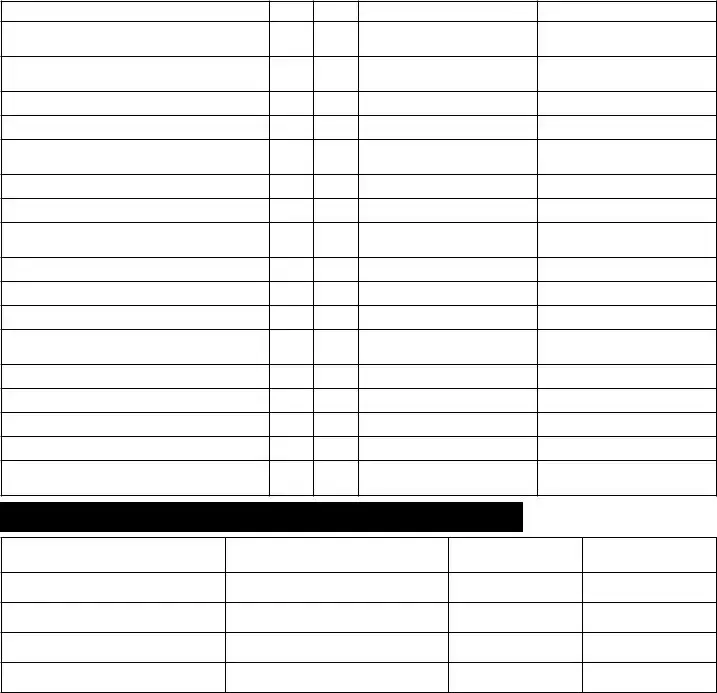
29.Assets: Complete the assets section by providing the requested asset information for you and your spouse. List your assets and your spouse’s assets. Include assets you own jointly with family or other persons, including your spouse. Include assets your spouse owns jointly with you, family or other persons. Each item must be answered YES or NO. If answered
YES, enter amount or current value and owner(s).
Type of Asset |
YES NO |
Amount or Value |
Owner(s) of Asset |
Has anyone in your household received a federal tax refund in the last 12 months?
Cash on hand, in a safety deposit box or
patient trust fund
Home, life estate/life lease
Real estate, not your home
Mortgage, land contract or other notes payable to you
Savings bonds or money market funds
Stocks or mutual funds
Pension, IRA, KEOGH, 401K or deferred
compensation account(s)
Trust funds
Life Insurance
Annuity
Cars, vans, trucks, campers, boats, snow- mobiles, other vehicles
Tools, equipment, livestock, or crops
Funeral contracts
Burial plot, casket, etc.
Health Savings Account
Are there any other assets? (Please Explain)
Checking/Draft Accounts — Savings/Share Accounts — Certiicates of Deposit
Name(s) on the Account
Name and Address of Bank
Credit Union, Savings and Loan
Account Number
Balance
YES NO
30.Have you received a
settlement, lawsuit award, worker’s compensation, lottery winnings, etc.? |
c |
c |
31. Do you have a pending lawsuit that may bring property or money to you? |
c |
c |
32.Within the last 60 months (5 years) have you or a joint owner or other person whose name is also listed on the asset:
• |
sold, given away, or transferred ownership in any asset such as those listed above? |
c |
c |
• |
removed or added a name on any asset such as those listed above? |
c |
c |
33.Have you or someone acting for you ever put any money, income, lawsuit settlement or assets in a
trust, annuity or similar device? |
c |
c |
4 |
34.Income: Include income for yourself and everyone listed in question 12.
Is anyone employed or
|
Persons employed or |
|
Employer name |
|
Wages before |
|
How often paid: weekly, |
||||||
|
|
|
|
|
deductions |
|
every 2 wks, monthly, other |
||||||
|
|
|
|
|
|
$ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
$ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Every item below must be answered YES or NO. |
|
|
|
|
|
|
|
|
|
||||
Type of Income |
|
|
|
YES |
NO |
|
|
Amount |
Whose Income |
||||
|
|
|
|
|
|
|
|
|
|
|
|||
Social Security Beneits (RSDI) Claim # |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|||
Social Security Beneits (RSDI) Claim # |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|||
Supplemental Security Income (SSI) |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|||
Supplemental Security Income (SSI) |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|||
Retirement Beneits |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|||
Veterans Beneits |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|||
Disability Beneits |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|||
Rental Income |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|||
Worker’s Compensation |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|||
Child Support |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|||
Unemployment Compensation |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|||
Military Allotments |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
||||
Gaming Distributions (Casino Proit Sharing) |
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
||||
Is there any other income? (Please explain) |
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
35. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Address where your spouse lives |
|
|
|
|
|
|
|
|
|
Spouse’s Phone Number |
|||
|
|
|
|
|
|
|
|||||||
City |
|
State |
|
|
Zip Code |
County |
|||||||
|
|
|
|
|
|
|
|
|
|
||||
Household Expenses |
Check YES or NO and write in the answer about you and/or your spouse’s home. |
||||||||||||
|
|
|
|
|
|
YES |
|
NO |
|
|
AMOUNT |
HOW OFTEN PAID |
|
|
|
|
|
|
|
|
|
|
|
||||
Do you and/or your spouse have a rent, mortgage or other shelter |
|
|
|
|
|
|
|
|
|
||||
expense? |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|||||||||
Do you and/or your spouse have the following expenses separate from rent or mortgage: |
|
||||||||||||
• |
Renter’s Insurance |
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
||
• |
Property Taxes |
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|||
• Mobile Home Lot Rent |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
||
• |
Special Assessments |
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
||
• |
Homeowner’s Insurance |
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
||
• |
Mortgage Guarantee Insurance |
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|||
• Cooperative or Condominium Fee |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|||
Do you and/or your spouse have an obligation to pay for heat and/ |
|
|
|
|
|
|
|
|
|
||||
or utilities? |
|
|
|
|
|
|
|
|
|
|
|||
5 |
ASSIGNMENT OF BENEFITS
Recovery of Medical Costs. I understand that when the Michigan Department of Health and Human Services
(MDHHS) pays the cost of hospital, surgical, or medical services, any right to recover costs from a third person or public or private contractor, except Medicare, is transferred to the MDHHS. Payment of any recovery under such right is to be made directly to the State of Michigan — MDHHS.
RELEASES
Social Security Information. I will allow the Social Security Administration to give to the MDHHS all information necessary to determine my eligibility for beneits under the Healthcare Coverage program until the second month following the expiration of my eligibility based on the current application.
Eligibility Information. I understand that the information I have provided will be used to determine my eligibility for Healthcare Coverage only and for purposes of administering the Healthcare Coverage program.
AFFIDAVIT
Under penalties of perjury, I swear that this application has been examined by or read to me, and, to the best of my knowledge, the facts are true and complete. If I am a third party applying on behalf of another person, I swear that this application has been examined by or read to the applicant, and, to the best of my knowledge, the facts are true and complete.
I certify, under penalty of perjury, that all information that I have written on this form or told to a specialist is true. I understand that I can be prosecuted for perjury if I have intentionally given false information. I also know that I may be asked to show proof of any information I have given. I also know that if I have intentionally left out any information or if I have given false information, which causes me to receive assistance I am not entitled to or more assistance that I am entitled to, I can be prosecuted for fraud. I understand I must report changes in income, assets or health insurance coverage to the department within 10 days of the change.
If you have any questions, contact your specialist or the local MDHHS before signing the application.
I understand that upon my death the Michigan Department of Health and Human Services (MDHHS) has the legal right to seek recovery from my estate for services paid by Healthcare Coverage. This means that some of all of my estate may be recovered. MDHHS will not seek to recover against the estate while there is a legal surviving spouse or a legal surviving child who is under the age of 21, blind, or disabled. An estate consists of real and personal property. If you have received an asset disregard due to a
IMPORTANT: YOU MUST SIGN THE APPLICATION
I certify that I have received and reviewed a copy of the Acknowledgments that explains additional information about applying for and receiving Healthcare Coverage.
Signature (Patient or Representative) |
Date |
Two Witnesses only if signed by X |
Date |
||
|
|
1. |
|
|
|
|
|
2. |
|
|
|
|
|
|
|
||
Signature (Patient or Representative) |
Date |
Two Witnesses only if signed by X |
Date |
||
|
|
1. |
|
|
|
|
|
2. |
|
|
|
|
|
|
|
|
|
If you are signing this application on behalf of someone else, complete the information below.
Name of person completing application |
Phone Number |
Relationship to patient |
|
|
|
|
|
Street Address |
City |
State |
Zip Code |
|
|
|
|
6 |
Form Characteristics
| Fact Name | Description |
|---|---|
| Purpose | The DHS-4574 form is used to apply for health care coverage for patients in nursing facilities in Michigan. |
| Assistance Availability | The Michigan Department of Health and Human Services (MDHHS) must assist individuals in completing the application if requested. |
| Interpreter Service | MDHHS provides free interpreter services if needed during the application process or interview. |
| Application Processing Time | Applications must be approved or denied within 45 days, or 90 days if disability is a factor. |
| Laws Governing the Form | This form is governed by 42 CFR Part 435, outlining regulations for Medicaid eligibility. |
| Non-Discrimination Policy | MDHHS does not discriminate against individuals based on race, religion, age, or several other factors. |
| Voluntary Completion | Completing the DHS-4574 form is voluntary but mandatory for those seeking health care coverage through MDHHS. |
Guidelines on Utilizing Michigan Dhs 4574
Completing the Michigan DHS 4574 form is an important step in the process of applying for health care coverage while residing in a nursing facility. Following these instructions carefully will help ensure that all necessary information is provided correctly. After you fill out this form, it will be submitted to the local Michigan Department of Health and Human Services (MDHHS) office for review. Approval or denial of your application will be communicated within a designated timeframe.
- Begin by printing your full name in the designated section at the top of the form.
- Enter your Client ID, Case Number, County, District, Section, and Unit.
- Indicate if you need an interpreter for assistance during the interview by checking either “Yes” or “No”, and specify the language if applicable.
- Complete questions that require information about your assets and those of your spouse, if relevant. Start with Patient’s Name and their residential address, continuing with the Spouse’s Name and their residential address.
- Input the dates of birth and Social Security numbers for both the patient and spouse.
- Answer the question regarding whether you and/or your spouse have any assets by checking “Yes” or “No”, and if applicable, check the types of assets owned.
- For each asset listed, provide the name and address of the institution, the account or policy number, and the balance or value of the asset.
- Sign and date the form in the appropriate sections on pages 2 and 4 to validate your application.
- After completing the form, review it for accuracy and completeness.
- Submit the form by mailing it or hand-delivering it to your local MDHHS office.
What You Should Know About This Form
What is the Michigan DHS 4574 form used for?
The Michigan DHS 4574 form is an application designed specifically for individuals who reside in nursing facilities and are seeking health care coverage. This form collects important information regarding the patient’s financial situation and personal details to determine eligibility for assistance. It is crucial for ensuring that those who need healthcare services receive the support they require.
How do I submit the Michigan DHS 4574 form?
You can submit the Michigan DHS 4574 form in a couple of ways. You may choose to either mail the completed form to your local Michigan Department of Health and Human Services (MDHHS) office or have someone deliver it for you. Make sure that the form is filled out completely and accurately to prevent any delays in processing your application.
What should I do if I need assistance completing the form?
If you need help filling out the Michigan DHS 4574 form, you are encouraged to contact your specialist or visit the office listed on the application. Assistance is available, and the Michigan Department of Health and Human Services is prepared to provide an interpreter at no cost, should you require one. It’s important to advocate for yourself if you encounter any refusal for help; you can reach out to the support line at 855-275-6424 or 855-789-5610 for assistance.
What happens after I submit my application?
Once you submit the Michigan DHS 4574 form, the department has specific timelines within which they must respond. Generally, your application will be approved or denied within 45 days. However, if determining your eligibility involves assessing disability, this period can extend up to 90 days. Patience is key during this process, as eligibility evaluations can take time to ensure accuracy.
Who is eligible to use the Michigan DHS 4574 form?
This form is intended for individuals who are patients in nursing facilities and wish to apply for health care coverage. If you are seeking assistance for other family members regarding medical expenses, a different application, known as DCH-1426, should be utilized instead. Understanding which form to use is fundamental to a smooth application process.
What information is required on the form?
The Michigan DHS 4574 form requires detailed information about both the patient and their spouse, if applicable. This includes names, social security numbers, financial assets like bank accounts and property holdings, and personal identification details. Providing complete and accurate information is essential for determining eligibility for health care coverage.
Common mistakes
Filling out the Michigan DHS 4574 form can be straightforward, but errors often occur. One common mistake is not providing accurate information regarding personal details. Individuals sometimes fail to double-check the spelling of names or inputting incorrect Social Security numbers. These inaccuracies could lead to delays or denials in coverage.
Another frequent mistake is neglecting to sign required pages. The form specifically asks for signatures on pages 2 and 4. Omitting these signatures might result in the application being incomplete and subsequently rejected.
People often forget to provide comprehensive details about their assets. When listing assets, respondents should include all types of properties, bank accounts, and other financial holdings. Leaving out information could lead to an incorrect assessment of eligibility.
A lack of clarity in responses can also be problematic. Some applicants may choose to answer questions with vague descriptions. Instead, specific information helps the review process and ensures faster decisions regarding eligibility.
Furthermore, applicants may miss deadlines for submission. It is essential to understand that the application must be processed within a specified timeframe. Failure to submit the form on time can have negative consequences for healthcare coverage.
Another issue arises from not answering all questions. Some applicants may skip questions believing they are not applicable. Every item on the form contributes to understanding the applicant’s circumstances, and skipped questions can hinder the evaluation process.
Using the wrong form is another mistake to avoid. There can be confusion between the DHS 4574 and other application forms. It’s critical to ensure that the correct form is used, as each serves different purposes.
Moreover, applicants sometimes submit the application without supporting documentation. Providing required proof of income and assets is vital. Incomplete submissions can lead to unnecessary delays in processing.
Finally, not asking for help can prove to be a significant error. Many individuals shy away from seeking assistance due to embarrassment or confusion. Utilizing available resources, such as local offices or interpreters, can clarify the application process and help prevent potential mistakes.
Documents used along the form
The Michigan DHS 4574 form is essential for individuals applying for health care coverage as nursing facility patients. However, several other forms and documents may be needed to support the application process. Here are some of the key documents often used alongside the 4574 form.
- DCH-1426: This application is for health coverage and assistance with medical costs for family members who are not in a nursing facility. It allows for additional dependents to seek support.
- DHS-4574-B: This supplementary form is used to declare the assets of both the patient and their spouse. It is critical for determining eligibility for health care coverage.
- Asset Verification Document: In some cases, supporting documents may be required to verify the assets declared. This could include bank statements, property deeds, or investment account statements.
- Authorization for Release of Information: This document allows the Michigan Department of Health and Human Services (MDHHS) to access personal information from third parties, ensuring they have all necessary data to process the application.
- Income Documentation: Individuals may need to provide proof of income, such as pay stubs, tax returns, or social security statements, to assess their eligibility for coverage.
- Medicare Card: If applicable, a copy of the Medicare card may be required to determine the applicant's current health coverage status.
- Proof of Residence: This could include utility bills, rental agreements, or other documents that confirm the applicant’s current address.
- Medical History Documentation: Providing a summary or detailed records of medical conditions may help in evaluating the need for specific health care services.
- Interpreter Request Form: If the applicant requires language assistance, this form ensures that appropriate resources are available during the application process.
Organizing these documents can streamline the application process and help ensure that individuals receive the assistance they need promptly. Support is always available, so do not hesitate to reach out if you need further guidance.
Similar forms
- Michigan DHS-1426 Form: This form, known as the Application for Health Coverage and Help Paying Costs, is similar as it also serves to assess eligibility for health care coverage. While the DHS-4574 is specific to nursing facility patients, the DHS-1426 is used for family members who require assistance with medical expenses.
- Michigan Medicaid Application Form: Like the DHS-4574, this application is utilized to determine Medicaid eligibility. Both forms collect personal and financial information, but the Medicaid Application can encompass a wider range of potential applicants beyond just nursing facility residents.
- MI Bridges Application: The MI Bridges application allows for access to health care, food assistance, and other benefits. Similar to the DHS-4574, it evaluates an applicant's needs based on their specific circumstances and financial status, supporting comprehensive care options.
- Community Health Assessment Form: This form focuses on evaluating the overall health needs of individuals within the community. Both the Community Health Assessment and DHS-4574 collect details to help determine eligibility for health benefits. However, the Community Health Assessment aims to address broader public health initiatives.
Dos and Don'ts
When filling out the Michigan DHS 4574 form for health care coverage as a patient in a nursing facility, it's important to be thorough and accurate. Here are seven things to keep in mind:
- DO read each item carefully before responding.
- DO provide complete and accurate information about your assets and personal details.
- DO sign your name where indicated on the form (pages 2 and 4).
- DO seek help from the Michigan Department of Health and Human Services if needed.
- DON'T leave any fields blank unless instructed to do so.
- DON'T provide false or misleading information, as this can delay your application.
- DON'T forget to check whether you or your spouse have any joint assets that need disclosing.
Following these guidelines will ensure a smoother application process and help you receive the assistance you need.
Misconceptions
Misconceptions about the Michigan DHS 4574 form can lead to confusion and delays in processing applications for health care coverage. Here’s a closer look at some common myths:
- Only Nursing Home Patients Can Apply: Many believe that only those currently residing in nursing facilities can use this form. However, the application is intended for individuals seeking health care coverage, not solely limited to nursing home patients.
- You Must Be Low-Income to Use the Form: While income is a factor in determining eligibility, it's a misconception that only low-income individuals qualify. This form is designed to assess various factors and can accommodate different financial situations.
- You Cannot Get Help Filling Out the Form: Some people think they have to complete the form solely on their own. In reality, assistance is available. The Michigan Department of Health and Human Services encourages applicants to seek help if needed, including free interpretation services.
- Submitting the Form Guarantees Coverage: A common misunderstanding is that simply turning in the form guarantees health care coverage. The application must be reviewed, and eligibility must be determined based on several criteria.
- Your Assets Are Irrelevant: Some applicants overlook the importance of asset disclosure, assuming their assets won't be considered. In truth, the form requires a detailed account of both the applicant's and their spouse's assets, as this information plays a crucial role in evaluating eligibility.
Understanding these points can help applicants navigate the application process more effectively and reduce any stress associated with completing the Michigan DHS 4574 form.
Key takeaways
Completing the Michigan DHS 4574 form is essential for individuals in nursing facilities seeking healthcare coverage. Here are key takeaways about the process and usage of this form:
- Eligibility Determination: This form is specifically designed to assess eligibility for health care coverage for patients currently residing in a nursing facility.
- Assistance Availability: Help is available for individuals filling out this form. You can contact your specialist for assistance or to obtain an interpreter at no cost.
- Timeframe for Response: The Michigan Department of Health and Human Services (MDHHS) will either approve or deny the application within 45 days. If disability is a factor, this may extend to 90 days.
- Information on Assets: The form collects information regarding the assets owned by the patient and their spouse, as asset status influences health care coverage eligibility.
- Multiple Signatures Required: It is crucial to sign your name on pages 2 and 4 of the form to ensure the application is valid.
- Alternative Application: Should other family members need assistance with medical expenses, they should complete the DCH-1426 form instead.
- Non-Discrimination Policy: MDHHS adheres to a non-discrimination policy, ensuring all individuals receive fair treatment regardless of various personal characteristics.
- Collect Necessary Information: Before completing the form, gather all needed financial and personal information, including social security numbers and asset values.
- Submit Form Appropriately: Applications can be submitted via mail or delivered in person to your local MDHHS office for processing.
Browse Other Templates
University of Richmond Transfer - Parents must act promptly to ensure their transfer request is received in a timely manner.
Runsheet - Enhance team collaboration with clear responsibilities.
Clinical Forms - Revising treatment plans based on feedback can improve service delivery.