Fill Out Your Milburn 875R Form
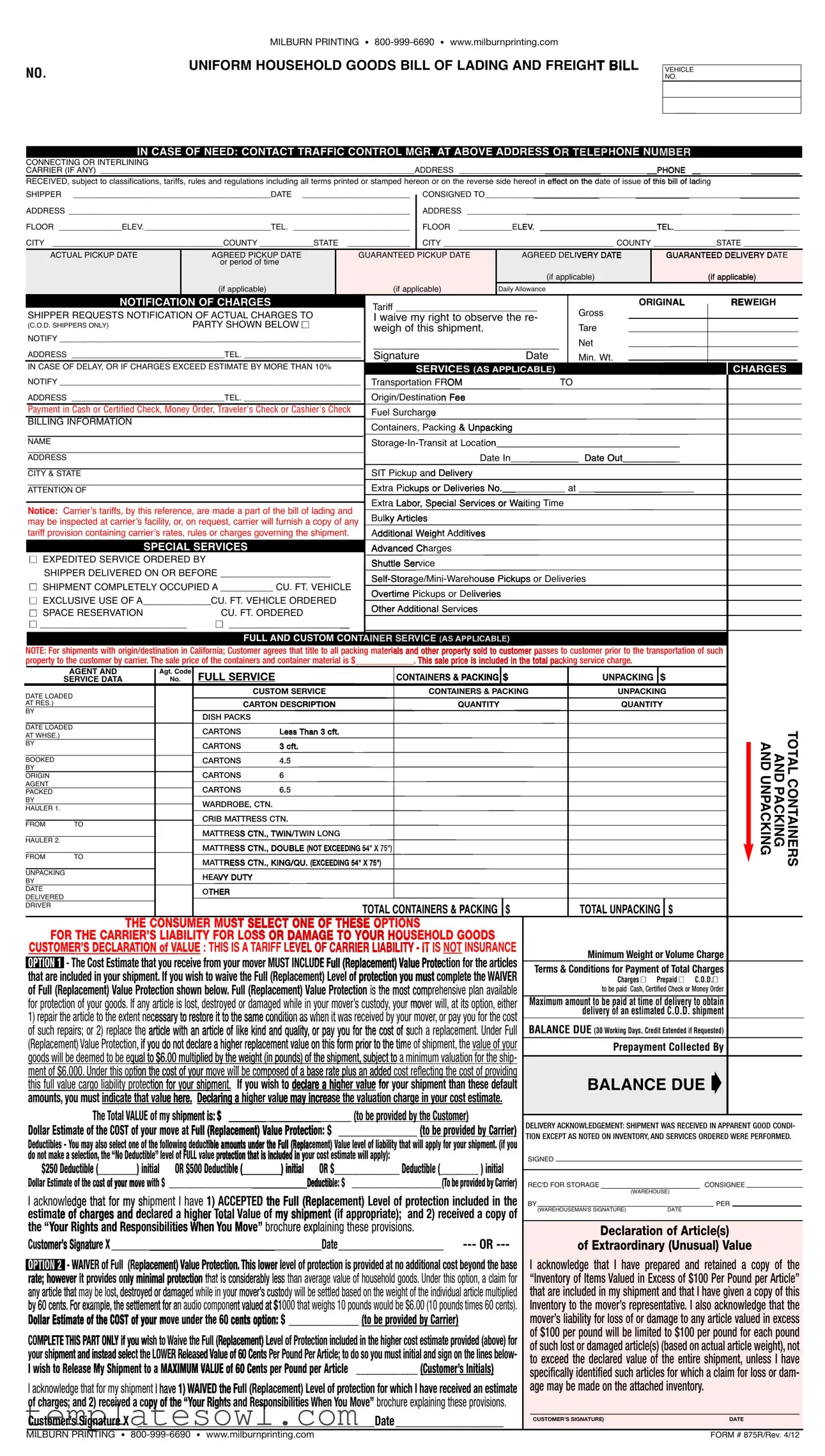
The Milburn 875R form is an essential document used in the moving and trucking industries, ensuring that proper guidelines and protocols are followed during the transportation of household goods. Key components of the form include details about the shipper, such as name and contact information, along with specific dates for pickup and delivery. It outlines important financial aspects, including tariff rates and notification of charges, while also permitting the shipper to waive their right to observe reweighing of the shipment. The form details various services available such as expedited service, storage-in-transit, and any extra labor required, all of which may incur additional charges. Another significant feature is the customer’s declaration of value, which allows individuals to select a level of protection for their goods, thereby clarifying liability in the case of loss or damage. The Milburn 875R form not only serves as a bill of lading but also acts as a contract, incorporating the carrier's tariffs and terms associated with the shipment of goods. By including these comprehensive details, the form protects both the shipper and the carrier, and serves as a vital tool in the industry.
Milburn 875R Example
|
MILBURN PRINTING • |
NO. |
UNIFORM HOUSEHOLD GOODS BILL OF |
|
IN CASE OF NEED: CONTACT TRAFFIC CONTROL MGR.
NO.
CONNECTING OR INTERLINING
CARRIER (IF ANY) ______________________________________________________________________
RECEIVED, subject to classifications, tariffs, rules and regulations including all terms printed or stamped hereon
SHIPPER ____________________________________________DATE ________________________
ADDRESS ____________________________________________________________________________ 
FLOOR ______________ELEV.____________________________TEL. __________________________
CITY ______________________________________COUNTY ____________STATE ______________ CITY ______________________________________ COUNTY ______________STATE ____________
ACTUAL PICKUP DATE
AGREED PICKUP DATE or period of time
(if applicable)
|
AGREED |
DELIVERY DATE |
GUARANTEED DELIVERY DATE |
||
|
(if applicable) |
|
|
|
|
|
(if applicable) |
||||
|
|
|
|
|
|
Daily Allowance
|
NOTIFICATION OF CHARGES |
SHIPPER REQUESTS NOTIFICATION OF ACTUAL CHARGES TO |
|
(C.O.D. SHIPPERS ONLY) |
PARTY SHOWN BELOW n |
NOTIFY ___________________________________________________________________
ADDRESS __________________________________TEL. __________________________
Tariff ___________________________
I waive my right to observe the re- weigh of this shipment.
_______________________________
SignatureDate
ORIGINAL
Gross
Tare
Net
Min. Wt.
REWEIGH
|
IN CASE OF DELAY, OR IF CHARGES EXCEED ESTIMATE BY MORE THAN 10% |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
NOTIFY ___________________________________________________________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TO |
||||||||
|
Transportation FR |
OM |
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Origin/Destinatio |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
ADDRESS __________________________________TEL. __________________________ |
n Fee |
|
|
|
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Payment in Cash or Certified Check, Money Order, Traveler's Check or Cashier's Check |
Fuel Surcharge |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
BILLING INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Containers, Packing & Unpacking |
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NAME |
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
tion___________________________________ |
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ADDRESS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date In_____________ Date Out___________ |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SIT Pickup |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
CITY & STATE |
|
|
|
|
and Delivery |
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Extra |
Pickups or Deliveries No.____________ at ______________________ |
||||||||||||||||||||||||
|
ATTENTION OF |
|
|
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
Extra |
Labor, Special Services or Waiting Time |
||||||||||||||||||||||||
|
Notice: Carrierʼs tariffs, by this reference, are made a part of the bill of lading and |
||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
may be inspected at carrierʼs facility, or, on request, carrier will furnish a copy of any |
Bu |
lky Articles |
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
tariff provision containing carrierʼs rates, rules or charges governing the shipment. |
A |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
dditional Weight Additives |
|
|
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SPECIAL SERVICES |
|
Advanced Ch |
arges |
|
|
|
|
|||||||||||||||||||||||
|
n EXPEDITED SERVICE ORDERED BY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Shuttle Ser |
vice |
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
SHIPPER DELIVERED ON OR BEFORE _____________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
or Deliveries |
||||||||||||||||||||||||||||
|
n SHIPMENT COMPLETELY OCCUPIED A __________ CU. FT. VEHICLE |
|
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
Overtime Pickups or Deliveries |
|
|
|
|
|
|
||||||||||||||||||||||
|
n EXCLUSIVE USE OF A_____________CU. FT. VEHICLE ORDERED |
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
n SPACE RESERVATION |
CU. FT. ORDERED |
|
Other Additional Services |
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
n ____________________________ |
n _______________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NOTE: For shipments with origin/destination in |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
such |
|
|
property to the customer by carrier. The sale price |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
AGENT AND |
Agt. Code |
FULL SERVICE |
|
CONTAINERS & PACKING $ |
UNPACKING $ |
|
|
|
|
SERVICE DATA |
No. |
|
|
|
|
|
|
|
|
DATE LOADED |
|
|
CUSTOM SERVICE |
CONTAINERS & PACKING |
UNPACKING |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
AT RES.) |
|
|
CARTON DESCRIPTION |
QUANTITY |
QUANTITY |
|
|
|
|
BY |
|
|
DISH PACKS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DATE LOADED |
|
|
CARTONS |
LESS THAN 3 CFT. |
|
|
|
|
TOTAL |
AT WHSE.) |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
||
BY |
|
|
CARTONS |
3 CFT. |
|
|
AND AND |
||
|
|
|
|
|
|||||
AGENT |
|
|
|
|
|
|
|||
BOOKED |
|
|
CARTONS |
4.5 |
|
|
|
|
|
BY |
|
|
|
|
|
|
|
|
|
ORIGIN |
|
|
CARTONS |
6 |
|
|
UNPACKING |
PACKING |
CONTAINERS |
|
|
|
MATTRESS CTN., KING/QU. (EXCEEDING 54" X 75") |
|
|
||||
PACKED |
|
|
CARTONS |
6.5 |
|
|
|
|
|
BY |
|
|
WARDROBE, CTN. |
|
|
|
|
|
|
HAULER 1. |
|
|
|
|
|
|
|
|
|
FROM |
TO |
|
CRIB MATTRESS CTN. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
HAULER 2. |
|
|
MATTRESS CTN., TWIN/TWIN LONG |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MATTRESS CTN., DOUBLE (NOT EXCEEDING 54" X 75") |
|
|
|
|
|
|
FROM |
TO |
|
|
|
|
|
|
|
|
UNPACKING |
|
|
HEAVY DUTY |
|
|
|
|
|
|
BY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DATE |
|
|
OTHER |
|
|
|
|
|
|
DELIVERED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DRIVER |
|
|
|
|
|
TOTAL UNPACKING |
$ |
|
|
|
|
|
|
|
|
|
|
||
THE CONSUMER MUST SELECT ONE OF THESE OPTIONS
|
|
FOR |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
CUSTOMER’S DECLARATION of VALUE : THIS IS A TARIF |
F LEVEL OF CARRIER LIABILITY - IT IS NOT INSURANCE |
|
|
Minimum Weight or Volume Charge |
|
|||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
OPTION 1 |
|
- The Cost Estimate that you receive from your mover MUST INCL |
UDE Full (Replacement) Value Protec |
tion for the articles |
|
Terms & Conditions for Payment of Total Charges |
|
|||||||||||||||||||||||||||||||||||||||||||||
that are |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Charges n |
Prepaid n C.O.D.n |
|
|||||||||||
of Full (Replacement) Value Protection shown below. Full (Replacement) Value Protection |
is the most comp |
rehensive plan available |
|
|
|
|
to be paid Cash, Certified Check or Money Order |
|
|
|||||||||||||||||||||||||||||||||||||||||||
for |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Maximum amount to be paid at time of delivery to obtain |
|
||||||||||||||
1) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
delivery of an estimated C.O.D. shipment |
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
BALANCE DUE (30 Working Days, Credit Extended if Requested) |
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
(Replacement) Value Protection, if you do not declare a higher replacement value on this form prior to the tim |
e of shipment, the value of your |
|
|
|
Prepayment Collected By |
|
||||||||||||||||||||||||||||||||||||||||||||||
goods will be deemed to be |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
minimum valuation for the ship- |
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
ment of $6,000. Under this |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
reflecting the cost of providing |
|
|
|
BALANCE DUE Á |
|
|
|
|
||||||||||||||
this full value cargo liability prote |
|
|
|
|
|
|
|
|
|
|
If you wish t |
|
|
|
|
|
|
|
|
|
|
|
|
default |
|
|
|
|
|
|
||||||||||||||||||||||
ction for your shipment. |
|
|
declare a higher value |
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||
o |
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||
amounts, you must indicate that va |
lue here. |
|
|
|
|
|
|
|
|
|
|
the valuation charge in your cost estimate. |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
|
|
|
|
|
The Total VALUE of my s |
|
|
|
|
|
|
|
|
|
|
_______ (to be provided by the Customer) |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
hipment is: $ _____________________ |
|
DELIVERY ACKNOWLEDGEMENT: SHIPMENT WAS RECEIVED IN APPARENT GOOD CONDI- |
|
|||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
Dollar Estimate of the COST of your move at |
Full (Replacement) Value Protectio |
n: $ |
__________________ (to be provided by Carrier) |
|
||||||||||||||||||||||||||||||||||||||||||||||||
TION EXCEPT AS NOTED ON INVENTORY, AND SERVICES ORDERED WERE PERFORMED. |
|
|||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
shipment. (if you |
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
do not make a selection, the “No Deductible” level of FULL value |
protection that is included in yo |
ur cost estimate will apply): |
SIGNED |
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
) initial |
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
provided by Carrier) |
REC'D FOR STORAGE |
|
|
CONSIGNEE |
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(WAREHOUSE) |
|
||||||
I acknowl |
edge that for my sh |
ipment I have |
|
|
|
|
|
|
included in the |
BY |
|
|
|
|
|
PER |
|
|
|
|||||||||||||||||||||||||||||||||
the “ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
” broch |
|
|
|
|
|
|
|
|
|
|
|
|
|
received a copy of |
|
(WAREHOUSEMAN'S SIGNATURE) |
DATE |
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
Your Rights and Responsibilities When You Move |
ure expl |
aining these provisions. |
|
|
|
Declaration of Article(s) |
|
|||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
of Extraordinary (Unusual) Value |
|
|||||||||||
|
|
|
|
- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
additional cost beyond the base |
I acknowledge that I have prepared and retained a copy of the |
|
|||||||||||||||||
OPTION 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
. Under this option, a claim for |
“Inventory of Items Valued in Excess of $100 Per Pound per Article” |
|
||||||||||||||||||||||||||||||||||||||||
rate; however it provides only minimal protection |
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
of the individual article multiplied |
that are included in my shipment and that I have given a copy of this |
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
$6.00 (10 pounds times 60 cents). |
Inventory to the mover’s representative. I also acknowledge that the |
|
||||||||||||||||
|
|
|
|
$ ________________ (to be provided by Carrier) |
mover’s liability for loss of or damage to any article valued in excess |
|
||||||||||||||||||||||||||||||||||||||||||||||
Dollar Estimate of the COST of your move under the 60 cents option: |
|
|||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
higher cost estimate provided (above) for |
of $100 per pound will be limited to $100 per pound for each pound |
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
of such lost or damaged article(s) (based on actual article weight), not |
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
must initial and sign on the lines below- |
to exceed the declared value of the entire shipment, unless I have |
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
______________ (Customer’s Initials) |
specifically identified such articles for which a claim for loss or dam- |
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
I acknowledge that for my shipment |
|
|
|
|
for which I have received an estimate |
age may be made on the attached inventory. |
|
|||||||||||||||||||||||||||||||||||||||||||||
I have |
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Move” brochure explaining these provisions. |
__________________________________________________ |
|
||||||||||||||||||
Customer’s Signature X |
|
____________________________________________Date____________________ |
|
|||||||||||||||||||||||||||||||||||||||||||||||||
|
CUSTOMER’S SIGNATURE) |
|
|
|
DATE |
|
||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MILBURN PRINTING • |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FORM # 875R/Rev. 4/12 |
|
|||||||||||||||||||||||||||||||||||

CONTRACT TERMS
Except when transportation is performed under the provisions of Item 1 tion performed by carrier in addition to all other rules, regulations, rates, and the location(s) specified by the carrier.
This contract is subject to all the rules, regulations, rates and charges lowing terms and conditions:
SECTION 1: The carrier or party in possession shall be liable for
(a) |
From an act, omission or order of shipper; |
|
(b) |
From defect or inherent vice of the article, including |
|
|
changes therein; |
|
(c) From (1) hostile or warlike action in time of peace or |
|
|
|
ed attack (A) by any government or sovereign |
|
|
or air forces; or (C) by an agent of any such |
|
|
force whether in time of peace or war; (3) |
|
|
hindering, combating, or defending against such |
by |
|
order of any government or public authority; |
|
(d) From terrorist activity, including action in |
regard- |
|
|
less of any other cause or event that contributes |
which |
|
is unlawful under the laws of the United |
conveyance |
|
(including an aircraft, vessel, cab, truck, |
threatening |
|
to kill, injure, or continue to detain, |
abstain from |
|
doing any act as an explicit or implicit |
any (A) bio- |
|
logical agent, chemical agent, or |
for mere per- |
|
sonal monetary gain), with intent |
to property; |
|
or (5) a threat, attempt, or conspiracy |
|
(e) |
From delay caused by strikes, |
in any such occur- |
|
rence or disorder, and from |
the shipment from |
|
such causes, is instructed |
|
(f) |
From Acts of God. |
|
SUBJECT, in addition to the
The carrier’s or the party’s in 
(l)The lump sum value weight of the shipment, in pounds, whichever is greater, or
weight of the shipment, in pounds, whichever is greater, or
(2) The actual loss |
the shipper has waived lump |
sum value liability |
pound per article. |
SECTION 2. The |
lack of capacity of any highway, |
bridge or ferry, or |
of the carrier; nor shall the car- |
rier be bound to |
carrier shall have the right in case of |
physical necessity |
tion. |
SECTION 3. |
|
(a) The |
shipment from carrier, shall be liable, jointly |
and |
including, but not limited to, sums advanced |
or |
for such unpaid charges shall not thereby |
|
been extended shall fail to pay such charges. |
(b) |
explosives or dangerous articles or goods.. |
SECTION 4. |
the face hereof, or at any changed address of which |
carrier |
warehouse selected by it at the point of delivery or at |
other |
|
SECTION 5. |
property fails to receive or claim it within fifteen (15) days |
|
shown on face hereof, or if shipper fails or refuses to pay |
|
option, either (a) upon notice in the manner authorized by |
|
named by carrier, thirty (30) days notice of which sale shall |
|
once a week for two consecutive weeks in a newspaper of gen- |
|
as described in the bill of lading, and the names of the con- |
|
applicable to shipment and toward expenses of notice, adver- |
|
if any shall be paid to owner of property; PROVIDED that any |
|
such notices, if, in the opinion of carrier, such action is necessary to |
prevent deterioration or further deterioration. |
|
SECTION 6. |
or delay, must be filed in writing with carrier within nine (9) months |
|
then within nine (9) months after a reasonable time for delivery has |
|
from the date when notice in writing is given by carrier to the claimant |
|
. Where a claim is not filed or suit is not instituted thereon in accordance |
|
be paid. |
Form Characteristics
| Fact Name | Detail |
|---|---|
| Form Purpose | The Milburn 875R form is a standardized bill of lading specifically for household goods transport. |
| Governing Law | This form is governed by federal regulations and applicable state laws related to household goods transportation. |
| Contact Information | Milburn Printing can be reached at 800-999-6690 or via their website at www.milburnprinting.com. |
| Shipments Included | The form covers various shipment types, including interstate and intrastate household moves. |
| Weight Declaration | A weight declaration is necessary, using terms like Gross, Tare, and Net to establish costs. |
| Valuation Options | Shippers must select a level of liability protection for their goods, with minimum valuations outlined. |
| Delivery Acknowledgment | The recipient must acknowledge receipt of goods in apparent good condition or note any discrepancies. |
| Storage Services | The form allows for the recording of details for storage-in-transit services, if requested. |
| Notifying Charges | Shippers can request notifications of actual charges, which are crucial for C.O.D. shipments. |
Guidelines on Utilizing Milburn 875R
Completing the Milburn 875R form is a straightforward process. This form will require specific information about the shipment, as well as details regarding the shipper and consignee. It is crucial to fill it out accurately to ensure that all terms and requirements are acknowledged. Below are the necessary steps to follow when filling out this form.
- Enter the Shipper's Information: Fill in your name, address, floor number, elevator information, and contact number in the designated fields.
- Complete the Dates: Provide the actual pickup date, agreed pickup date, agreed delivery date, and guaranteed delivery date where applicable.
- Shipping Details: Specify the daily allowance and any notification of charges needed. If applicable, name the party to notify and provide their contact details.
- Weight Information: Fill out sections regarding gross, tare, and net weights, including minimum weight requirements.
- Additional Charges: Identify any extra charges that may apply, such as storage-in-transit, special services, or fuel surcharges.
- Service Data: Detail the types of containers used, packing and unpacking requirements, and any carton descriptions with quantities.
- Value Declaration: Choose your option for the customer’s declaration of value and indicate your shipment’s total value.
- Signature Requirement: Both the shipper's and consignee's signatures are needed. Make sure to sign and date the form to confirm all details.
Once the form is completed, review all entries for accuracy. If any additional clarifications or confirmations about the shipment's conditions are necessary, refer to the guidelines provided or consult with your carrier. It is important that both you and the carrier have a clear understanding of the terms outlined in the form.
What You Should Know About This Form
What is the Milburn 875R form used for?
The Milburn 875R form serves as a Household Goods Bill of Lading. It is a contract between the shipper and the moving company, detailing the shipment of household goods. This form includes important information like pickup and delivery dates, shipper and consignee details, and any additional services requested. It ensures clarity on the terms of transportation and the responsibilities of both parties.
What information do I need to provide on the Milburn 875R form?
When filling out the Milburn 875R form, you must provide specific information such as the names and addresses of both the shipper and the consignee, the actual and agreed pickup and delivery dates, and any notification preferences regarding charges. You will also need to include details about the goods being transported, such as their weight and any special services requested like packing or storage.
What is the 'Declaration of Value' section about?
This section allows you to declare the value of your items being shipped. The form specifies two options: Full (Replacement) Value Protection and a minimal protection option. The declared value affects the liability of the carrier in case of loss or damage during transport. It's crucial to be accurate in this declaration to ensure proper coverage.
What happens if there is a delay in delivery?
If there is a delay, the form includes a provision requiring the carrier to notify the shipper. This includes any delays caused by factors outside the carrier's control. In case charges exceed the estimate by more than 10%, the carrier is obligated to provide notification as well. It ensures transparency and allows shippers to stay informed about their shipments.
Can I waive my right to observe the reweigh of my shipment?
Yes, the Milburn 875R form includes an option for you to waive your right to observe the reweigh of the shipment. By signing this waiver, you agree to accept the weight estimate provided by the carrier without personal verification. This is a choice that should be considered carefully, as it could affect your total charges based on shipment weight.
What are the payment options outlined in the Milburn 875R form?
The form specifies acceptable payment methods which include cash, certified checks, money orders, traveler’s checks, or cashier's checks. Payment must be settled before or upon delivery, depending on the arrangements made. This section aims to clarify any confusion regarding payment at the time of service.
How does the Milburn 875R form protect me as the shipper?
The form offers several protective measures for shippers. It details the carrier's liability in case of loss or damage, specifies the minimum protection levels, and provides clear guidelines regarding claims for delayed shipments. By documenting all agreements and conditions, the form creates accountability and helps protect your rights as a consumer during the moving process.
Common mistakes
Filling out the Milburn 875R form can be straightforward, but several common mistakes can hinder the process. First, one of the biggest errors is neglecting to fill in the shipping address completely. An incomplete address can lead to delivery delays or, in some cases, returns.
Another frequent mistake involves the selection of the pickup and delivery dates. It's crucial to provide accurate dates or a specific time frame. Not doing so could cause scheduling conflicts with the carrier.
People often fail to understand the notification of charges section. It is essential that shippers note who should be contacted about any actual charges, particularly for collect-on-delivery shipments. Leaving this blank can lead to confusion and unforeseen expenses.
Additionally, many overlook the signature and date line. Without a signature, the form is not valid. It's a simple step that can easily be forgotten but is necessary to move the process forward.
Inaccuracies in the total weight and charges can also complicate the shipment. Double-checking amounts before submitting the form is crucial to ensure the proper billing of services rendered.
An often-missed detail is the declaration of value. Shippers must either select their coverage option or explicitly state their chosen value. If this section is left unchecked, default terms may apply, which may not align with the shipper’s expectations.
Some individuals write in their own modifications in sections, which may lead to misunderstandings. It's best to stick to the options provided on the form, as deviations could cause discrepancies or delays.
Another pitfall is misunderstanding the tariff information. Any tariffs mentioned become a part of the contract and should always be reviewed carefully before signing off.
Finally, a common mistake is ignoring the special services and provisions section. This area often contains important information relevant to the shipment, specifically if there are any additional requirements or fees.
By avoiding these mistakes, you can ensure a smoother experience when submitting the Milburn 875R form.
Documents used along the form
The Milburn 875R form is an essential document in the transportation of household goods, particularly in moving-related transactions. Along with this form, several other documents may be required to ensure a smooth moving process and compliance with legal regulations. Below is a list of six commonly associated forms and documents that facilitate the transportation of goods.
- Bill of Lading: This document serves as a contract between the shipper and the carrier for the transportation of goods. It outlines the terms and conditions of the shipment, including the responsibilities of both parties. It is also a receipt for the goods, indicating that the carrier has taken possession of them.
- Inventory List: The inventory list is a detailed enumeration of all items being shipped. This list helps verify the contents of the shipment and assists in handling claims for lost or damaged goods. Shippers should keep a copy for their records as well.
- Delivery Receipt: Upon delivery of the goods, the delivery receipt is signed by the recipient to confirm that they have received the shipment in good condition. This document acts as proof of delivery and may be useful for future reference or claims.
- Insurance Declaration: If the shipper opts for additional insurance coverage, an insurance declaration form may be required. This document specifies the value of the goods and what coverage is provided in case of loss or damage during transit.
- Change of Address Form: For individuals moving to a new home, a change of address form can ensure that the postal service reroutes mail efficiently. This is an important step that ensures no important correspondence goes missing after the move.
- Service Agreement: This formalizes the terms under which the moving services are provided. It details the services agreed upon, costs, and any special provisions, ensuring that both parties are clear on their obligations throughout the moving process.
When preparing for a move, understanding and organizing these additional documents can help facilitate the transition. By ensuring all necessary paperwork is completed and accessible, shippers can reduce potential complications and enhance the overall efficiency of the moving process.
Similar forms
- BILL OF LADING: Similar to the Milburn 875R form, a Bill of Lading serves as a contract and receipt for the transportation of goods. It outlines the responsibilities of the carrier and the shipper and provides crucial shipment details.
- Freight Bill: This document details the charges for transporting freight. Like the Milburn 875R, it confirms shipment specifics, including departure and destination, while also noting any additional charges that may apply.
- USDA Shipping Permit: Much like the Milburn 875R form, this permit is necessary for certain types of goods, facilitating their safe transport in compliance with federal regulations.
- Delivery Receipt: Upon receiving goods, a delivery receipt acknowledges their receipt in apparent good condition. This mirrors the Milburn’s delivery acknowledgment section, serving as proof of delivery.
- Shipping Manifest: This document lists all items included in a shipment. Similar to the Milburn 875R, it helps in tracking and managing shipment contents and timelines effectively.
- Customs Declaration: Used for international shipping, this document declares the contents of a shipment to customs authorities, sharing similarities with the Milburn form in clear documentation of what is being shipped.
- Warehouse Receipt: Issued by a warehouse upon receiving goods for storage, it acts like the Milburn 875R by formalizing the receipt and condition of stored items.
- Insurance Policy: This document details the coverage for goods while in transit. The Milburn 875R form parallels this by outlining liability options for the shipment's value, ensuring protection against potential loss or damage.
Dos and Don'ts
- Do: Read the instructions carefully before starting to fill out the form.
- Do: Provide accurate and complete information in all sections of the form.
- Do: Make sure to sign and date the form where indicated.
- Do: Double-check all phone numbers and contact details for correctness.
- Do: Clearly state any special service requests or delivery instructions.
- Don't: Leave any required fields blank, as this may delay processing.
- Don't: Attempt to alter any printed information on the form.
- Don't: Forget to keep a copy of the completed form for your records.
- Don't: Use abbreviations or shorthand that may lead to misunderstandings.
- Don't: Submit the form without confirming all charges and declarations of value.
Misconceptions
- Misconception 1: The Milburn 875R form is only for residential moves.
- Misconception 2: All shipping companies use the Milburn 875R form.
- Misconception 3: Signing the Milburn 875R form means I can't change my mind.
- Misconception 4: The form is not legally binding.
- Misconception 5: Delivery dates are always guaranteed.
- Misconception 6: I won't be charged if my shipment is delayed.
- Misconception 7: The Milburn 875R form covers insurance for my belongings.
- Misconception 8: I can ignore the "Notification of Charges" section.
- Misconception 9: I can request changes to services after signing the form at any time.
- Misconception 10: The Milburn 875R form is self-explanatory and does not require any legal advice.
This form is applicable for both residential and commercial shipments, making it versatile for various moving needs.
While it is a common form, not all carriers or moving companies may use this specific document. Each company may have its own standardized paperwork.
Signing the form indicates agreement to the terms of shipment, but it does not prevent you from discussing changes with the carrier before the move takes place.
The Milburn 875R form serves as a legal document outlining the terms of the shipment, and it is generally considered binding once signed by both parties.
While the form may include agreed delivery dates, these dates can be affected by various factors outside the carrier's control, and guarantees may vary.
Even in the event of a delay, certain fees may still apply, depending on the terms laid out in the form and the carrier's policies.
The form includes options for liability and valuation protection but does not equate to traditional insurance coverage. Additional insurance may be advisable.
This section is important as it specifies how and when you will be informed about any actual charges incurred during the shipment process.
Changes typically must be agreed upon by both parties and should be addressed promptly to avoid complications.
While many people may understand the form, seeking clarification or legal advice is advisable when dealing with any significant move or shipment.
Key takeaways
When filling out and using the Milburn 875R form, it’s important to keep several key points in mind:
- Accurate Information: Always ensure the shipper's name, address, and other contact details are filled out correctly.
- Pickup and Delivery Dates: Clearly specify the actual pickup date, the agreed pickup date, and the desired delivery date.
- Notification of Charges: C.O.D. shippers must provide a notification request for actual charges.
- Weight and Charges: Record all relevant weight information including gross, tare, and net weight for accuracy.
- Service Options: Indicate any special services requested, such as expedited service or storage-in-transit.
- Declaration of Value: Select a customer’s declaration of value, which affects liability. Know your options!
- Signature Required: Ensure both the shipper’s and consignee’s signatures are obtained on the form for validation.
- Retain Copies: Keep a copy of the completed form for your records, as it is vital in case of any disputes.
- Understand Charges: Be familiar with specific charges, such as fuel surcharges, to avoid surprises later.
- Timeliness in Claims: In case of any damage or loss, claims need to be filed in writing within nine months of the incident.
By following these guidelines, you can ensure that your use of the Milburn 875R form goes smoothly. This preparation can save time, reduce errors, and lead to a more efficient moving experience.
Browse Other Templates
Where Can I Get My Edd Disability Form - A thorough review of the instructions can help avoid common mistakes.
Notice of Right to Cure Default - It helps protect borrowers' rights while also maintaining lenders’ interests.
Irs 1099 C - The IRS offers a variety of methods to obtain further assistance and guidance through various channels.