Fill Out Your Minnesota Accident Report Form
Completing the Minnesota Accident Report form is essential for drivers involved in motor vehicle accidents. This form, known as PS 32001, is required for any crash that results in at least $1,000 worth of property damage, or involves injuries or fatalities. All drivers involved must fill out and submit the report to Driver and Vehicle Services within 10 days of the accident. Failure to do so can lead to misdemeanor charges under Minnesota Statute 169.09, subdivision 7. The report gathers important information regarding the time and location of the accident, driver and vehicle details, and insurance information. In addition, it collects descriptions of the type of incident, including collision details and environmental conditions at the time. Passengers’ information and a detailed narrative of the accident are also included to ensure a complete account of what occurred. Each section must be filled accurately to provide a clear picture of the incident and its aftermath. Remember, the information within this document is critical for road safety, and maintaining accurate records helps in analyzing traffic patterns and improving Minnesota's road infrastructure.
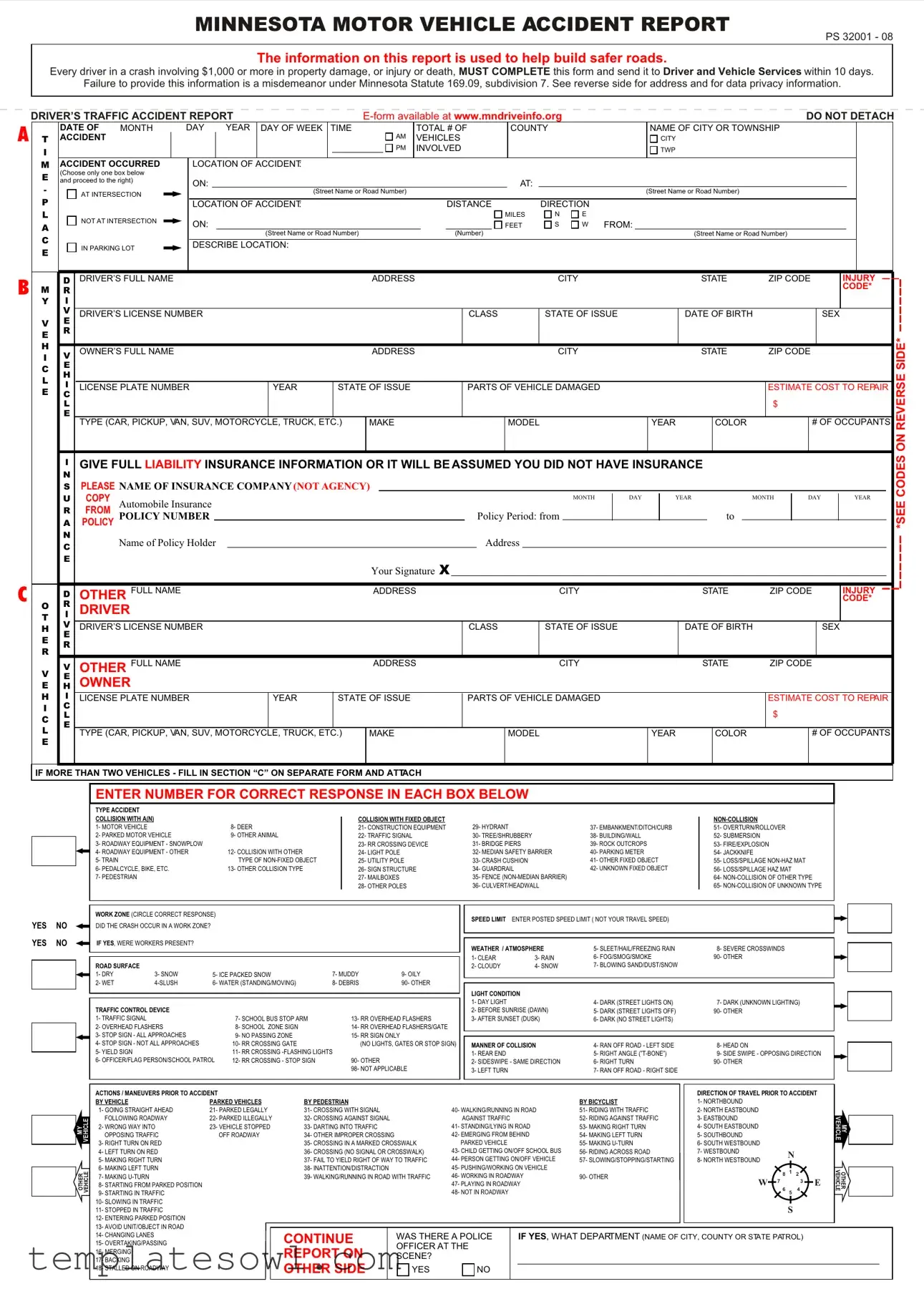
Minnesota Accident Report Example
MINNESOTA MOTOR VEHICLE ACCIDENT REPORT
PS 32001 - 08
The information on this report is used to help build safer roads.
Every driver in a crash involving $1,000 or more in property damage, or injury or death, MUST COMPLETE this form and send it to Driver and Vehicle Services within 10 days.
Failure to provide this information is a misdemeanor under Minnesota Statute 169.09, subdivision 7. See reverse side for address and for data privacy information.
A
B
C
DRIVER’S TRAFFIC ACCIDENT REPORT |
|
|
|
DO NOT DETACH |
|||||||||||||||||||||||||
|
|
DATE OF |
MONTH |
DAY |
YEAR |
DAY OF WEEK |
TIME |
|
|
TOTAL # OF |
|
COUNTY |
|
|
NAME OF CITY OR TOWNSHIP |
|
|
|
|
||||||||||
T |
|
ACCIDENT |
|
|
|
|
|
|
|
|
|
|
AM |
VEHICLES |
|
|
|
|
|
CITY |
|
|
|
|
|
||||
I |
|
|
|
|
|
|
|
|
|
|
|
|
|
PM |
INVOLVED |
|
|
|
|
|
TWP |
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
M |
|
ACCIDENT OCCURRED |
LOCATION OF ACCIDENT: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
E |
|
(Choose only one box below |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
and proceed to the right) |
ON: |
|
|
|
|
|
|
|
|
|
|
|
|
|
AT: |
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
AT INTERSECTION |
|
|
|
|
(Street Name or Road Number) |
|
|
|
|
|
|
|
|
(Street Name or Road Number) |
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
P |
|
|
|
|
|
LOCATION OF ACCIDENT: |
|
|
|
|
DISTANCE |
|
|
DIRECTION |
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
L |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MILES |
N |
E |
|
|
|
|
|
|
|
|
A |
|
|
NOT AT INTERSECTION |
ON: |
|
|
|
|
|
|
|
|
|
|
FEET |
S |
W FROM: |
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
C |
|
|
|
|
|
|
|
|
|
(Street Name or Road Number) |
|
|
|
|
(Number) |
|
|
|
|
|
(Street Name or Road Number) |
|
|
|
|
||||
|
|
IN PARKING LOT |
DESCRIBE LOCATION: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
D DRIVER’S FULL NAME |
|
|
|
|
|
|
|
ADDRESS |
|
|
|
|
|
|
CITY |
|
|
STATE |
ZIP CODE |
|
INJURY |
||||||
M |
|
R |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CODE* |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Y |
|
I |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
V |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DRIVER’S LICENSE NUMBER |
|
|
|
|
|
|
|
|
CLASS |
|
|
STATE OF ISSUE |
|
DATE OF BIRTH |
|
SEX |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
VE
E R
H |
V |
|
OWNER’S FULL NAME |
|
|
ADDRESS |
|
CITY |
|
STATE |
ZIP CODE |
||
I |
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
C |
E |
|
|
|
|
|
|
|
|
|
|
|
|
H |
|
|
|
|
|
|
|
|
|
|
|
|
|
L |
|
|
|
|
|
|
|
|
|
|
|
|
|
I |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LICENSE PLATE NUMBER |
YEAR |
STATE OF ISSUE |
PARTS OF VEHICLE DAMAGED |
|
|
|
ESTIMATE COST TO REPAIR |
||||
E |
C |
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
L |
|
|
|
|
|
|
|
|
|
|
$ |
|
|
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TYPE (CAR, PICKUP, VAN, SUV, MOTORCYCLE, TRUCK, ETC.) |
MAKE |
|
MODEL |
YEAR |
|
COLOR |
|
# OF OCCUPANTS |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
IGIVE FULL LIABILITY INSURANCE INFORMATION OR IT WILL BE ASSUMED YOU DID NOT HAVE INSURANCE
N
SPLEASE NAME OF INSURANCE COMPANY (NOT AGENCY)
|
|
U |
COPY |
Automobile Insurance |
|
|
|
|
|
|
|
|
|
|
|
|
MONTH |
|
DAY |
|
YEAR |
|
|
|
MONTH |
|
DAY |
|
YEAR |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
R |
FROM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
POLICY NUMBER |
|
|
|
|
|
|
|
|
Policy Period: from |
|
|
|
|
|
|
|
|
to |
|
|
|
|
|
|
|
|
|||||||
|
|
A |
POLICY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
C |
|
Name of Policy Holder |
|
|
|
|
|
|
|
Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Your Signature X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
D |
OTHER |
FULL NAME |
|
|
|
ADDRESS |
|
|
|
|
|
CITY |
|
|
|
|
STATE |
ZIP CODE |
|
INJURY |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CODE* |
||||
O |
|
R |
DRIVER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
T |
|
I |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
V |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
H |
|
DRIVER’S LICENSE NUMBER |
|
|
|
|
|
|
CLASS |
|
STATE OF ISSUE |
|
|
|
DATE OF BIRTH |
|
|
|
|
SEX |
|||||||||||||||
|
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
R |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
R |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
V |
|
V |
OTHER FULL NAME |
|
|
|
ADDRESS |
|
|
|
|
|
CITY |
|
|
|
|
STATE |
ZIP CODE |
|
|
|
|||||||||||||
|
HE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
E |
|
OWNER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
H |
|
I |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
LICENSE PLATE NUMBER |
|
YEAR |
STATE OF ISSUE |
|
PARTS OF VEHICLE DAMAGED |
|
|
|
|
|
|
|
|
ESTIMATE COST TO REPAIR |
||||||||||||||||||||
I |
|
C |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
$ |
|
|
|
|
|
|
|
C |
|
L |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
L |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TYPE (CAR, PICKUP, VAN, SUV, MOTORCYCLE, TRUCK, ETC.) |
MAKE |
|
|
MODEL |
|
|
|
|
YEAR |
|
|
COLOR |
|
|
# OF OCCUPANTS |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
IF MORE THAN TWO VEHICLES - FILL IN SECTION “C” ON SEPARATE FORM AND ATTACH |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
*SEE CODES ON REVERSE SIDE*
ENTER NUMBER FOR CORRECT RESPONSE IN EACH BOX BELOW
|
|
|
|
TYPE ACCIDENT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
COLLISION WITH A(N) |
|
|
|
|
COLLISION WITH FIXED OBJECT |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
1- MOTOR VEHICLE |
|
|
8- DEER |
|
21- CONSTRUCTION EQUIPMENT |
29- HYDRANT |
|
37- EMBANKMENT/DITCH/CURB |
51- OVERTURN/ROLLOVER |
|
|
|
|
|
2- PARKED MOTOR VEHICLE |
|
9- OTHER ANIMAL |
|
22- TRAFFIC SIGNAL |
30- TREE/SHRUBBERY |
|
38- BUILDING/WALL |
52- SUBMERSION |
||
|
|
|
|
3- ROADWAY EQUIPMENT - SNOWPLOW |
|
|
|
23- RR CROSSING DEVICE |
31- BRIDGE PIERS |
|
39- ROCK OUTCROPS |
53- FIRE/EXPLOSION |
||
|
|
|
|
4- ROADWAY EQUIPMENT - OTHER |
|
12- COLLISION WITH OTHER |
|
24- LIGHT POLE |
|
32- MEDIAN SAFETY BARRIER |
40- PARKING METER |
54- JACKKNIFE |
||
|
|
|
|
5- TRAIN |
|
|
TYPE OF |
|
25- UTILITY POLE |
33- CRASH CUSHION |
|
41- OTHER FIXED OBJECT |
55- LOSS/SPILLAGE |
|
|
|
|
|
6- PEDALCYCLE, BIKE, ETC. |
|
13- OTHER COLLISION TYPE |
|
26- SIGN STRUCTURE |
34- GUARDRAIL |
|
42- UNKNOWN FIXED OBJECT |
56- LOSS/SPILLAGE HAZ MAT |
||
|
|
|
|
7- PEDESTRIAN |
|
|
|
|
27- MAILBOXES |
|
35- FENCE |
|
64- |
|
|
|
|
|
|
|
|
|
|
28- OTHER POLES |
36- CULVERT/HEADWALL |
|
65- |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
WORK ZONE (CIRCLE CORRECT RESPONSE) |
|
|
|
|
SPEED LIMIT ENTER POSTED SPEED LIMIT ( NOT YOUR TRAVEL SPEED) |
|
||||
YES |
NO |
|
|
|
|
|
|
|
|
|||||
DID THE CRASH OCCUR IN A WORK ZONE? |
|
|
|
|
|
|
|
|
|
|||||
YES |
NO |
IF YES, WERE WORKERS PRESENT? |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
WEATHER / ATMOSPHERE |
5- SLEET/HAIL/FREEZING RAIN |
8- SEVERE CROSSWINDS |
|||||||
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
1- CLEAR |
3- RAIN |
6- FOG/SMOG/SMOKE |
90- OTHER |
|
|
|
|
ROAD SURFACE |
|
|
|
|
|
|
2- CLOUDY |
4- SNOW |
7- BLOWING SAND/DUST/SNOW |
|
|
|
|
|
1- DRY |
3- SNOW |
5- ICE PACKED SNOW |
7- MUDDY |
9- OILY |
|
|
|
|
||
|
|
|
|
2- WET |
6- WATER (STANDING/MOVING) |
8- DEBRIS |
90- OTHER |
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
LIGHT CONDITION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1- DAY LIGHT |
|
4- DARK (STREET LIGHTS ON) |
7- DARK (UNKNOWN LIGHTING) |
|
|
|
|
TRAFFIC CONTROL DEVICE |
|
|
|
|
|
2- BEFORE SUNRISE (DAWN) |
5- DARK (STREET LIGHTS OFF) |
90- OTHER |
||
|
|
|
|
1- TRAFFIC SIGNAL |
|
|
7- SCHOOL BUS STOP ARM |
|
13- RR OVERHEAD FLASHERS |
3- AFTER SUNSET (DUSK) |
6- DARK (NO STREET LIGHTS) |
|
||
|
|
|
|
2- OVERHEAD FLASHERS |
|
8- SCHOOL ZONE SIGN |
|
14- RR OVERHEAD FLASHERS/GATE |
|
|
|
|
||
|
|
|
|
3- STOP SIGN - ALL APPROACHES |
|
9- NO PASSING ZONE |
|
15- RR SIGN ONLY |
|
|
|
|
|
|
|
|
|
|
4- STOP SIGN - NOT ALL APPROACHES |
|
10- RR CROSSING GATE |
|
(NO LIGHTS, GATES OR STOP SIGN) |
MANNER OF COLLISION |
4- RAN OFF ROAD - LEFT SIDE |
8- HEAD ON |
|||
|
|
|
|
5- YIELD SIGN |
|
|
11- RR CROSSING |
|
1- REAR END |
|
5- RIGHT ANGLE |
9- SIDE SWIPE - OPPOSING DIRECTION |
||
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
6- OFFICER/FLAG PERSON/SCHOOL PATROL |
12- RR CROSSING - STOP SIGN |
|
90- OTHER |
|
2- SIDESWIPE - SAME DIRECTION |
6- RIGHT TURN |
90- OTHER |
|||
|
|
|
|
|
|
|
|
|
98- NOT APPLICABLE |
3- LEFT TURN |
|
7- RAN OFF ROAD - RIGHT SIDE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MY |
VEHICLE |
OTHER |
VEHICLE |
ACTIONS / MANEUVERS PRIOR TO ACCIDENT
BY VEHICLE |
PARKED VEHICLES |
1- GOING STRAIGHT AHEAD |
21- PARKED LEGALLY |
FOLLOWING ROADWAY |
22- PARKED ILLEGALLY |
2- WRONG WAY INTO |
23- VEHICLE STOPPED |
OPPOSING TRAFFIC |
OFF ROADWAY |
3- RIGHT TURN ON RED |
|
4- LEFT TURN ON RED |
|
5- MAKING RIGHT TURN |
|
6- MAKING LEFT TURN |
|
7- MAKING |
|
8- STARTING FROM PARKED POSITION |
|
9- STARTING IN TRAFFIC |
|
10- SLOWING IN TRAFFIC |
|
11- STOPPED IN TRAFFIC |
|
12- ENTERING PARKED POSITION |
|
13- AVOID UNIT/OBJECT IN ROAD |
|
14- CHANGING LANES |
|
15- OVERTAKING/PASSING |
|
16- MERGING |
|
17- BACKING |
|
18- STALLED ON ROADWAY |
|
|
|
|
|
|
|
|
|
|
DIRECTION OF TRAVEL PRIOR TO ACCIDENT |
|||||||
BY PEDESTRIAN |
|
|
|
|
BY BICYCLIST |
1- NORTHBOUND |
|
|
|
|
|
|
|
|
31- CROSSING WITH SIGNAL |
|
40- WALKING/RUNNING IN ROAD |
51- RIDING WITH TRAFFIC |
2- NORTH EASTBOUND |
|
|
|
|
|
|
|
|||
32- CROSSING AGAINST SIGNAL |
|
AGAINST TRAFFIC |
|
52- RIDING AGAINST TRAFFIC |
3- EASTBOUND |
|
|
|
|
|
|
|
||
33- DARTING INTO TRAFFIC |
|
41- STANDING/LYING IN ROAD |
53- MAKING RIGHT TURN |
4- SOUTH EASTBOUND |
|
|
|
|
|
|
|
|||
34- OTHER IMPROPER CROSSING |
|
42- EMERGING FROM BEHIND |
54- MAKING LEFT TURN |
5- SOUTHBOUND |
|
|
|
|
|
|
|
|||
35- CROSSING IN A MARKED CROSSWALK |
PARKED VEHICLE |
|
55- MAKING |
6- SOUTH WESTBOUND |
|
|
|
|
|
|
|
|||
36- CROSSING (NO SIGNAL OR CROSSWALK) |
43- CHILD GETTING ON/OFF SCHOOL BUS |
56- RIDING ACROSS ROAD |
7- WESTBOUND |
|
|
N |
|
|
|
|||||
37- FAIL TO YIELD RIGHT OF WAY TO TRAFFIC |
44- PERSON GETTING ON/OFF VEHICLE |
57- SLOWING/STOPPING/STARTING |
8- NORTH WESTBOUND |
|
|
|
|
|
||||||
38- INATTENTION/DISTRACTION |
|
45- PUSHING/WORKING ON VEHICLE |
|
|
|
|
|
|
|
|
|
|||
|
|
|
8 |
1 |
2 |
|
|
|||||||
39- WALKING/RUNNING IN ROAD WITH TRAFFIC |
46- WORKING IN ROADWAY |
90- OTHER |
|
|
|
|||||||||
|
|
|
|
|
||||||||||
W |
|
7 |
|
|
3 |
|
E |
|||||||
|
|
|
47- PLAYING IN ROADWAY |
|
|
|
|
|
||||||
|
|
|
|
6 |
|
|
4 |
|
||||||
|
|
|
48- NOT IN ROADWAY |
|
|
|
5 |
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
CONTINUE |
|
WAS THERE A POLICE |
|
IF YES, WHAT DEPARTMENT (NAME OF CITY, COUNTY OR STATE PATROL) |
|
|
||||||||
|
|
|
|
|||||||||||
|
OFFICER AT THE |
|
|
|
|
|
|
|
|
|
|
|
||
REPORT ON |
|
|
|
|
|
|
|
|
|
|
|
|
||
|
SCENE? |
|
|
|
|
|
|
|
|
|
|
|
|
|
OTHER SIDE |
|
YES |
NO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VEHICLE |
MY |
VEHICLE |
OTHER |
As required by Minnesota Data Privacy Act you are hereby informed that the information requested on this form is collected pursuant to statute to provide statistical data on traffic accidents. The time and place of the accident, names of parties involved and insurance information may be disclosed to any person involved in the accident or to others persons as specified by law. This written report cannot be used against you as evidence in any civil or criminal matter and your version of how the accident happened is confidential.
SEAT |
TYPE |
USE |
AIR BAG |
EJECT |
INJURY |
OCCUPANT SEAT POSITION CODES |
SAFETY EQUIPMENT TYPE |
RESTRAINT DEVICE USED |
SAFETY EQUIPMENT USED |
EJECTION CODES |
INJURY CODES |
|
CODES |
CODES |
CODES |
|
|
1- DRIVER |
|
|
|
1- TRAPPED, EXTRICATED |
K- KILLED |
(INCLUDE MOTORCYCLE DRIVER) |
1- NO SAFETY EQUIP IN PLACE |
1- BELTS NOT USED |
1- |
(BY MECHANICAL MEANS) |
A- INCAPACITATING INJURY |
2- FRONT CENTER |
|
2- LAP BELT ONLY USED |
2- |
2- TRAPPED, FREED BY |
B- |
3- FRONT RIGHT |
2- LAP BELT |
3- SHOULDER BELT ONLY USED |
3- |
C- POSSIBLE INJURY |
|
4- SECOND ROW SEAT LEFT |
3- SHOULDER BELT |
4- LAP AND SHOULDER BELT USED |
4- NOT |
3- PARTIALLY EJECTED |
N- NO APPARENT INJURY |
5- SECOND ROW SEAT CENTER |
4- LAP & SHOULDER BELT |
|
5- NOT |
4- EJECTED |
|
6- SECOND ROW SEAT RIGHT |
5- CHILD SAFETY SEAT |
5- CHILD SEAT NOT USED |
6- NOT DEPLOYED- UNKNOWN |
|
|
7- THIRD ROW SEAT LEFT |
6- CHILD BOOSTER SEAT |
6- CHILD SEAT USED IMPROPERLY |
IF SWITCH ON OR OFF |
5- NOT EJECTED OR TRAPPED |
|
8- THIRD ROW SEAT CENTER |
|
7- CHILD SEAT USED PROPERLY |
|
|
|
9- THIRD ROW SEAT RIGHT |
98- NOT APPLICABLE |
8- BOOSTER SEAT NOT USED |
90- OTHER DEPLOYMENTS |
|
|
10- OUTSIDE OF VEHICLE |
(MOTORCYCLE, |
9- BOOSTER SEAT USED IMPROPERLY |
98- NOT APPLICABLE |
|
|
11- TRAILING UNIT |
SNOWMOBILE, ECT.) |
10- BOOSTER SEAT USED PROPERLY |
(MOTORCYCLE, |
|
|
12- PICKUP TRUCK BED |
|
|
SNOWMOBILE, ECT.) |
|
|
13- TRUCK CAB SLEEPER SECTION |
|
11- HELMET NOT USED |
|
|
|
14- PASSENGER IN OTHER POSITION |
|
12- HELMET USED |
|
|
|
(INCLUDE MOTORCYCLE PASSENGER) |
|
|
|
|
|
15- PASSENGER IN UNKNOWN POSITION |
|
|
|
|
|
16- FRONT LEFT |
|
|
|
|
|
MY VEHICLE: DRIVER AND PASSENGERS INFORMATION: |
|
|
|
|
|
|
|
|
|
|
|
|
||
DRIVER >>>>>>>>>>>>>>>>>> |
|
DATE OF BIRTH (OR AGE) |
SEX |
SEAT |
TYPE |
USE |
AIR BAG |
EJECT |
|
|
INJURY |
|||
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PASSENGER NAME |
CITY |
STATE |
|
DATE OF BIRTH (OR AGE) |
SEX |
SEAT |
TYPE |
USE |
AIR BAG |
EJECT |
|
|
INJURY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PASSENGER NAME |
CITY |
STATE |
|
DATE OF BIRTH (OR AGE) |
SEX |
SEAT |
TYPE |
USE |
AIR BAG |
EJECT |
|
|
INJURY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PASSENGER NAME |
CITY |
STATE |
|
DATE OF BIRTH (OR AGE) |
SEX |
SEAT |
TYPE |
USE |
AIR BAG |
EJECT |
|
|
INJURY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DESCRIBE ACCIDENT IN SUFFICIENT DETAIL BELOW TO DISCLOSE CAUSES. |
|
|
|
|
|
|
INDICATE |
|||||||
|
|
|
|
|
|
|
NORTH |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DESCRIBE WHAT HAPPENED: |
|
|
DIAGRAM WHAT HAPPENED: |
|
|
|
|
|
BY ARROW |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DAMAGE TO PROPERTY OTHER THAN VEHICLES: (MAILBOX, FENCE, SIGNPOST, GUARDRAIL, ETC.)
DESCRIBE |
NAME OF |
PROPERTY |
PROPERTY |
DAMAGED: |
OWNER: |
|
|
ESTIMATE COST OF REPAIR
$
SIGN HERE X
SIGNATURE OF PERSON SUBMITTING REPORT IS REQUIRED
ADDRESS |
DATE OF REPORT |
MAIL THIS REPORT TO:
DVS / ACCIDENT RECORDS
445 MINNESOTA STREET, SUITE 181
ST. PAUL, MN
Form Characteristics
| Fact | Description |
|---|---|
| Governing Law | This form is regulated under Minnesota Statute 169.09, subdivision 7. |
| Property Damage Threshold | The form must be completed for accidents involving $1,000 or more in property damage. |
| Deadline for Submission | Accident reports must be submitted within 10 days of the accident. |
| Misdemeanor Penalty | Failure to submit the report is considered a misdemeanor. |
| Purpose of Information | The data collected helps build safer roads by providing traffic accident statistics. |
| Access to Information | Accident details may be disclosed to persons involved or as required by law. |
| Validity of Report | This report cannot be used against the individual in civil or criminal matters. |
Guidelines on Utilizing Minnesota Accident Report
Filling out the Minnesota Accident Report form takes careful attention to detail. It is important to provide accurate information to ensure compliance with state regulations. This form must be completed if an accident involves significant property damage or injuries. Here are clear steps to guide you through the process.
- Begin by entering the date of the accident, specifying the month, day, and year.
- Indicate the day of the week and the time the accident occurred.
- Specify the total number of vehicles involved in the accident.
- Provide the county name and the name of the city or township where the accident occurred.
- Detail the location of the accident, selecting whether it was on a street, at an intersection, or in a parking lot. Fill in the required additional information based on your selection.
- Fill in your full name, address, city, state, and ZIP code.
- Complete the section regarding your driver's license number, class, state of issue, date of birth, and sex.
- Next, fill in the vehicle owner’s full name, address, city, state, and ZIP code.
- Provide the license plate number, year, and state of issue for the vehicle involved.
- List the parts of your vehicle damaged and the estimated cost to repair them.
- Select the type of vehicle you were driving and provide details about its make, model, year, and color.
- Indicate the number of occupants in your vehicle.
- Provide your full liability insurance information, including the name of the insurance company, policy number, and policy period. Be sure to include the name and address of the policyholder.
- If applicable, fill in the details for other drivers involved in the accident using their full names, addresses, and information regarding their vehicles.
- Answer the questions regarding the type of accident and choose the corresponding codes. Ensure to indicate if there were any injuries and detail the circumstances to the best of your ability.
- Indicate the weather conditions and any traffic control devices present at the time of the accident.
- Describe the accident in a detailed manner. Include a diagram if necessary to explain the incident clearly.
- Lastly, sign the form and include the date of your report.
- Mail the completed form to DVS / Accident Records at the provided address.
Once you have thoroughly completed the form, it's critical to submit it within the 10-day deadline to avoid potential penalties. Proper completion ensures that the information you provide will assist in future road safety measures.
What You Should Know About This Form
What is the Minnesota Accident Report form?
The Minnesota Accident Report form is a document used to report any motor vehicle accident involving $1,000 or more in property damage, or injury or death. It helps authorities gather the necessary information to improve road safety and determine liability in accidents.
Who is required to complete this form?
All drivers involved in a crash that meets the specified damage or injury thresholds must complete the form. This is mandatory under Minnesota law, and failure to do so can result in misdemeanor charges.
When must the form be submitted?
The completed Minnesota Accident Report form must be submitted within 10 days of the accident. Delays can lead to legal consequences, so it is important to act quickly.
Where do I send the completed form?
Submit the completed form to the Driver and Vehicle Services at the following address: DVS / Accident Records, 445 Minnesota Street, Suite 181, St. Paul, MN 55101-5181.
How can I access the form?
The Minnesota Accident Report form can be obtained online at www.mndriveinfo.org. You may also physically obtain it from your local Driver and Vehicle Services office.
What information do I need to provide on the form?
The form requires details such as the date and time of the accident, location, vehicle information, driver information, insurance details, and descriptions of the events leading up to the accident. Be thorough and accurate to ensure proper processing.
What happens if I don’t have insurance?
If insurance information is not provided on the form, it will be assumed that you did not have insurance at the time of
Common mistakes
Completing the Minnesota Accident Report form can be a straightforward process, but many individuals make mistakes that can complicate matters. One common error is neglecting to submit the report within the mandated timeframe. According to the instructions, this form must be sent to Driver and Vehicle Services within **10 days** of the accident. Failing to do so can lead to legal consequences. Ensure that you keep track of the timeline to avoid this mistake.
Another frequent issue is incorrect or incomplete information. Filling out the form requires specific details about the accident location, the vehicles involved, and the parties' information. Leaving out critical elements, such as the **license plate numbers** or the **insurance information**, can hinder the processing of the report. Every section needs attention to detail, so double-check to ensure all necessary data is present and accurate.
People often forget to sign the form before submission, which can lead to delays in processing. Your signature is not just a formality; it’s a confirmation of the information provided. Without it, the report may be considered invalid. Always remember to sign and date the form before you mail it.
Many accidents involve multiple vehicles, yet individuals sometimes fail to report all parties involved. If you're in a multi-vehicle crash, it is essential to include every driver's information and the relevant insurance details. Omitting a driver or vehicle from the report could complicate matters and potentially lead to disputes over liability.
Providing vague descriptions of the incident can also be a pitfall. The section that requires a description of the accident must be filled with sufficient detail about what transpired. Using specific language and mentioning actions taken prior to the accident will provide a clearer picture and support any claims. Avoid ambiguity and focus on factual statements.
Lastly, confusion over terminology or codes can lead to mistakes in choosing options on the form. For example, selecting the wrong type of accident or misunderstanding the various classifications can distort the report’s accuracy. Familiarizing yourself with the terms used can help avoid this common error, ensuring that you select the appropriate responses for your situation.
Documents used along the form
When involved in an accident in Minnesota, completing the Minnesota Accident Report form is just one step in addressing the incident. There are several other documents and forms that may be needed to ensure a comprehensive approach to managing the aftermath of the accident. Below is a list of commonly associated forms.
- Insurance Claim Form: This document is submitted to your insurance company to seek compensation for damages or injuries sustained during the accident.
- Police Report: A report generated by law enforcement detailing the accident scene, contributing factors, and parties involved. It can be crucial for insurance claims.
- Medical Records: Documentation of diagnoses, treatments, and costs associated with any injuries suffered in the accident. These records help substantiate claims for medical expenses.
- Witness Statements: Written accounts from individuals who saw the accident can provide critical evidence. These statements can clarify the circumstances surrounding the accident.
- Release of Liability Form: This form is often used to relinquish the right to claim further damages after an agreement has been reached, particularly in cases of settlements.
- Vehicle Repair Estimates: Quotes or assessments from auto repair shops detailing the costs to fix damage to the vehicle involved in the accident, important for insurance processes.
- Release of Medical Information Form: This form allows insurance companies or other involved parties to obtain your medical records related to the accident, ensuring transparency in claims.
Proper handling of these documents can significantly influence the outcome of claims and legal matters following an accident. Always keep copies for your records and provide any required information promptly.
Similar forms
Florida Traffic Crash Report - Similar to the Minnesota Accident Report, this document must be completed after vehicle crashes resulting in damage or injury. It gathers essential details about the accident and involved parties, helping authorities assess the situation effectively.
California Accident Report - This form requires drivers involved in accidents to provide comprehensive information. Like the Minnesota form, it focuses on determining the circumstances surrounding the accident for better road safety and enforcement.
Texas Motor Vehicle Accident Report - This Texas report serves a similar purpose as its Minnesota counterpart. It collects information post-accident, emphasizing accountability from drivers involved in collisions.
Illinois Crash Report - Comparable to Minnesota’s document, the Illinois Crash Report captures crucial data about traffic accidents to support law enforcement in evaluating causes and responsibilities.
New York State Motor Vehicle Accident Report - This report requires submission by drivers involved in specific accidents. It shares similarities with the Minnesota form in its emphasis on reporting and documenting incidents for regulatory compliance.
Ohio Motor Vehicle Accident Report - Ohio's report is designed for collecting detailed information about accidents and aligning with similar objectives of determining liability, much like the Minnesota Accident Report.
Pennsylvania Accident Report - Similar to the Minnesota form, this Pennsylvania document plays a critical role in accident documentation, requiring driver input for effective assessment and follow-up by authorities.
Michigan Traffic Crash Report - This report collects vital information about accidents, aiming to inform state authorities and improve roadway conditions, mirroring the goals of Minnesota’s report.
Georgia Uniform Motor Vehicle Accident Report - Like the Minnesota form, this document must be completed for vehicle crashes resulting in certain damage or injuries. It assists in understanding traffic incidents thoroughly.
Virginia Crash Report - This form serves a similar purpose of gathering information about traffic collisions. It aids law enforcement and insurance companies alike, just as the Minnesota Accident Report does.
Dos and Don'ts
- Do ensure that you fill out the form accurately and completely. Mistakes or omissions could lead to complications.
- Don't delay in submitting the report. You must send it within 10 days of the accident to avoid penalties.
- Do provide all necessary personal information, including names, addresses, and insurance details of all parties involved.
- Don't forget to include the location details of the accident. Specify the exact place where the incident occurred.
- Do describe the accident thoroughly—details can aid in understanding what happened and determining liability.
- Don't make any assumptions or place blame when describing the accident; stick to the facts.
- Do keep a copy of the completed report for your own records after mailing it.
- Don't forget to sign the report. An unsigned report may be considered invalid.
Misconceptions
Understanding the Minnesota Accident Report form can be challenging due to various misconceptions. Here are some common myths and the truths behind them:
- Only serious accidents require a report. This is false. Any crash with over $1,000 in damages, or any injury or death, must be reported.
- The form can be submitted anytime. You must submit the form within 10 days following the accident.
- Filing the report is optional. It is mandatory. Failure to do so can lead to misdemeanor charges.
- Only police can fill out the form. Any driver involved in the accident can complete the report.
- The information is public and can be accessed by anyone. Certain details, like your exact fault in the accident, are kept confidential.
- You can ignore the insurance requirement on the form. Providing insurance details is necessary; otherwise, it will be assumed you have no coverage.
- The form is for police use only. This form is for the Minnesota Department of Driver and Vehicle Services and helps with road safety statistics.
- Once submitted, you cannot make changes. If you notice a mistake after sending the form, you can submit a corrected version.
- You need to get a police report to complete the form. While helpful, a police report is not a requirement to submit the accident report.
- The accident report is used against you in court. Your version of the accident is confidential and cannot be used as evidence.
By understanding these misconceptions, you can navigate the Minnesota Accident Report form more confidently.
Key takeaways
Filing a Minnesota Accident Report is crucial following a motor vehicle crash. Here are nine key takeaways to consider:
- Mandatory Submission: The report must be completed if the accident involves $1,000 or more in property damage, or if there are injuries or fatalities.
- Time Limit: The form must be submitted to Driver and Vehicle Services within 10 days of the accident.
- Legal Consequences: Failing to submit the report is classified as a misdemeanor under Minnesota law.
- Complete Accuracy: Ensure all information is accurate and complete, including personal details, location, and circumstances of the accident.
- Insurance Details: Include full liability insurance information; otherwise, it may be assumed no insurance was held.
- Information Privacy: The report is confidential and cannot be used against you in civil or criminal matters.
- Accident Description: Provide a clear and detailed description of the accident to aid in understanding the causes.
- Diagram Use: Utilize diagrams to illustrate the accident scene, highlighting all relevant details and directions.
- Mailing Instructions: Send the completed report to the specified address: DVS/Accident Records, 445 Minnesota Street, Suite 181, St. Paul, MN 55101-5181.
Understanding these key aspects can help ensure compliance and provide clarity in the aftermath of an accident.
Browse Other Templates
How Do I Find My Medicare Ptan Number - Clear guidelines ensure that all necessary data is collected for optimal processing.
Insurance Tracking as Your Interested Party - The coverage applies solely to the acts or omissions of the named insured or their representatives.
Xpo Bill of Lading Pdf - The document must be signed by authorized personnel from both the shipper and the carrier.