Fill Out Your Nc Fl2 Form
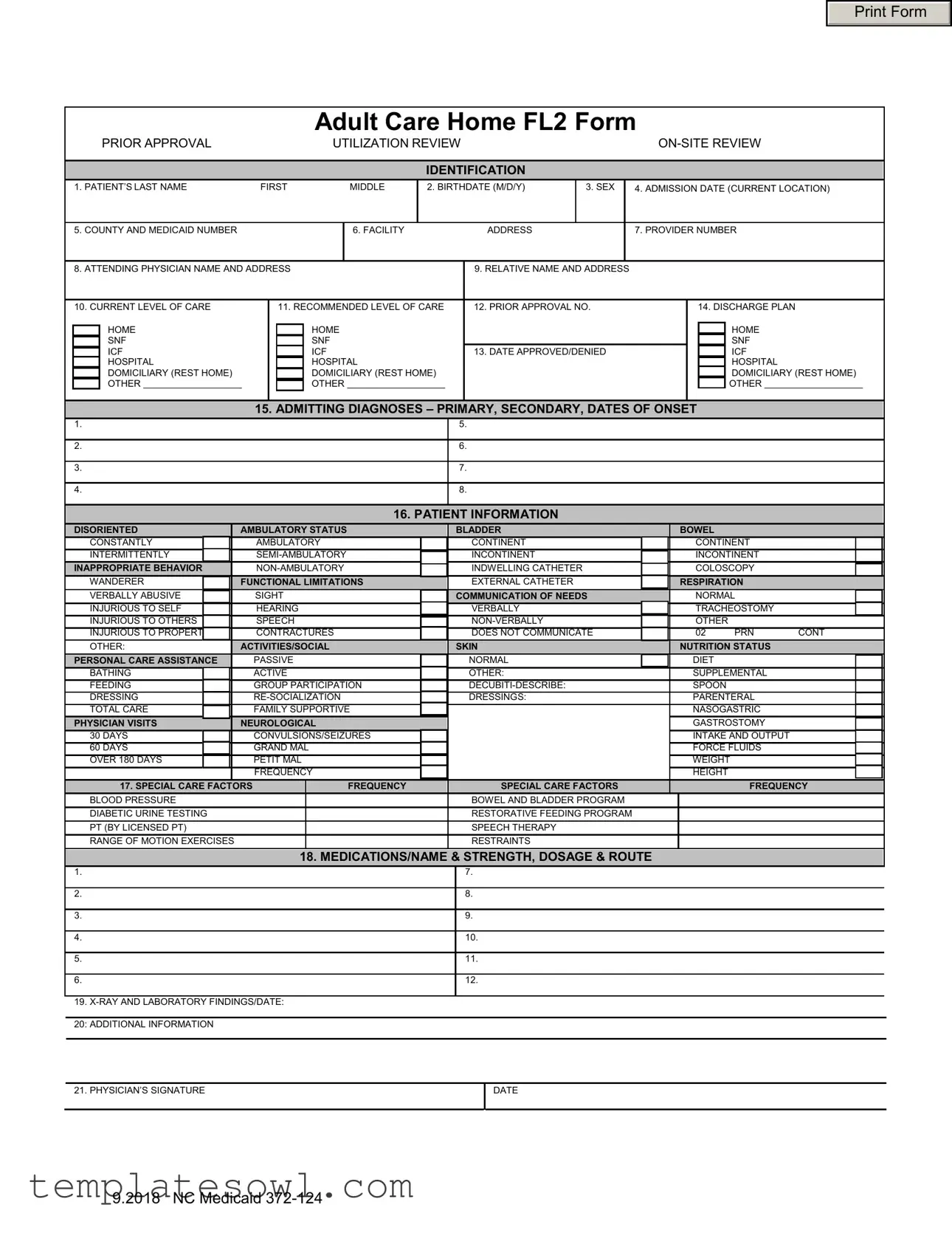
The NC FL2 form is an essential document used in the evaluation and approval process for individuals seeking admission to various adult care facilities within North Carolina. By carefully compiling detailed information about the patient, this form plays a pivotal role in ensuring that the right level of care is provided based on the individual's specific needs. Key sections of the form include the patient's personal information, such as name, date of birth, and Medicaid number, alongside critical data regarding their current and recommended levels of care. Additionally, the form includes areas to note the admitting diagnoses and the patient’s functional capabilities, which are crucial for appropriate placement. Special care factors, medication details, and any relevant X-ray or laboratory findings further contribute to a comprehensive understanding of the patient's health status. Notably, the attending physician’s certification and signature are required to validate the information provided, reinforcing the necessity of professional oversight in the care approval process. Understanding the nuances of the NC FL2 form can significantly impact the quality of care received by individuals transitioning into these facilities.
Nc Fl2 Example
Print Form
Adult Care Home FL2 Form
|
|
|
PRIOR APPROVAL |
|
|
|
UTILIZATION REVIEW |
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
IDENTIFICATION |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
1. PATIENT’S LAST NAME |
FIRST |
MIDDLE |
2. BIRTHDATE (M/D/Y) |
|
3. SEX |
|
4. ADMISSION DATE (CURRENT LOCATION) |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5. COUNTY AND MEDICAID NUMBER |
|
|
|
|
|
6. FACILITY |
|
|
ADDRESS |
|
|
7. PROVIDER NUMBER |
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
8. ATTENDING PHYSICIAN NAME AND ADDRESS |
|
|
|
9. RELATIVE NAME AND ADDRESS |
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
10. CURRENT LEVEL OF CARE |
|
|
11. RECOMMENDED LEVEL OF CARE |
|
12. PRIOR APPROVAL NO. |
|
|
|
|
14. DISCHARGE PLAN |
|
|
|||||||||||||
|
|
|
HOME |
|
|
|
HOME |
|
|
|
|
|
|
|
|
|
|
|
|
|
HOME |
|
|
||||
|
|
|
SNF |
|
|
|
SNF |
|
|
|
|
|
|
|
|
|
|
|
|
|
SNF |
|
|
||||
|
|
|
ICF |
|
|
|
ICF |
|
|
|
13. DATE APPROVED/DENIED |
|
|
|
|
|
|
ICF |
|
|
|||||||
|
|
|
HOSPITAL |
|
|
|
HOSPITAL |
|
|
|
|
|
|
|
|
|
|
|
|
HOSPITAL |
|
|
|||||
|
|
|
DOMICILIARY (REST HOME) |
|
|
|
DOMICILIARY (REST HOME) |
|
|
|
|
|
|
|
|
|
|
|
DOMICILIARY (REST HOME) |
||||||||
|
|
|
OTHER |
|
|
|
|
OTHER |
|
|
|
|
|
|
|
|
|
|
|
|
|
OTHER |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
15. ADMITTING DIAGNOSES – PRIMARY, SECONDARY, DATES OF ONSET |
|
|
|
|
|||||||||||||||||
|
1. |
|
|
|
|
|
|
|
|
|
|
5. |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
2. |
|
|
|
|
|
|
|
|
|
|
6. |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
3. |
|
|
|
|
|
|
|
|
|
|
7. |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
4. |
|
|
|
|
|
|
|
|
|
|
8. |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
16. PATIENT INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
DISORIENTED |
|
AMBULATORY STATUS |
|
|
BLADDER |
|
|
|
|
BOWEL |
|
|
|
|
|||||||||||
|
|
CONSTANTLY |
|
AMBULATORY |
|
|
|
CONTINENT |
|
|
|
|
|
CONTINENT |
|
|
|||||||||||
|
|
INTERMITTENTLY |
|
|
|
|
INCONTINENT |
|
|
|
|
|
INCONTINENT |
|
|
||||||||||||
|
|
INAPPROPRIATE BEHAVIOR |
|
|
|
|
INDWELLING CATHETER |
|
|
|
|
|
COLOSCOPY |
|
|
||||||||||||
|
|
WANDERER |
|
FUNCTIONAL LIMITATIONS |
|
|
EXTERNAL CATHETER |
|
|
|
|
RESPIRATION |
|
|
|||||||||||||
|
|
VERBALLY ABUSIVE |
|
SIGHT |
|
|
COMMUNICATION OF NEEDS |
|
|
|
NORMAL |
|
|
||||||||||||||
|
|
INJURIOUS TO SELF |
|
HEARING |
|
|
|
VERBALLY |
|
|
|
|
|
TRACHEOSTOMY |
|
|
|||||||||||
|
|
INJURIOUS TO OTHERS |
|
SPEECH |
|
|
|
|
|
|
|
|
OTHER |
|
|
|
|
||||||||||
|
|
INJURIOUS TO PROPERTY |
|
CONTRACTURES |
|
|
|
DOES NOT COMMUNICATE |
|
02 |
|
PRN |
CONT |
||||||||||||||
|
|
OTHER: |
|
ACTIVITIES/SOCIAL |
|
|
SKIN |
|
|
|
|
NUTRITION STATUS |
|
|
|||||||||||||
|
|
PERSONAL CARE ASSISTANCE |
|
PASSIVE |
|
|
|
NORMAL |
|
|
|
|
|
DIET |
|
|
|
|
|||||||||
|
|
BATHING |
|
ACTIVE |
|
|
|
OTHER: |
|
|
|
|
|
SUPPLEMENTAL |
|
|
|||||||||||
|
|
FEEDING |
|
GROUP PARTICIPATION |
|
|
|
|
|
|
|
SPOON |
|
|
|
|
|||||||||||
|
|
DRESSING |
|
|
|
|
DRESSINGS: |
|
|
|
|
|
PARENTERAL |
|
|
||||||||||||
|
|
TOTAL CARE |
|
FAMILY SUPPORTIVE |
|
|
|
|
|
|
|
|
|
NASOGASTRIC |
|
|
|||||||||||
|
|
PHYSICIAN VISITS |
|
NEUROLOGICAL |
|
|
|
|
|
|
|
|
|
|
GASTROSTOMY |
|
|
||||||||||
|
|
30 DAYS |
|
CONVULSIONS/SEIZURES |
|
|
|
|
|
|
|
|
|
INTAKE AND OUTPUT |
|
|
|||||||||||
|
|
60 DAYS |
|
GRAND MAL |
|
|
|
|
|
|
|
|
|
|
FORCE FLUIDS |
|
|
||||||||||
|
|
OVER 180 DAYS |
|
PETIT MAL |
|
|
|
|
|
|
|
|
|
|
WEIGHT |
|
|
||||||||||
|
|
|
|
|
|
FREQUENCY |
|
|
|
|
|
|
|
|
|
|
HEIGHT |
|
|
|
|
||||||
|
|
|
17. SPECIAL CARE FACTORS |
|
FREQUENCY |
|
|
SPECIAL CARE FACTORS |
|
|
|
|
|
|
FREQUENCY |
||||||||||||
|
|
BLOOD PRESSURE |
|
|
|
|
|
|
|
|
BOWEL AND BLADDER PROGRAM |
|
|
|
|
|
|
|
|
|
|
||||||
|
|
DIABETIC URINE TESTING |
|
|
|
|
|
|
|
|
RESTORATIVE FEEDING PROGRAM |
|
|
|
|
|
|
|
|
|
|
||||||
|
|
PT (BY LICENSED PT) |
|
|
|
|
|
|
|
|
SPEECH THERAPY |
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
RANGE OF MOTION EXERCISES |
|
|
|
|
|
|
|
|
RESTRAINTS |
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
18. MEDICATIONS/NAME & STRENGTH, DOSAGE & ROUTE |
|
|
|
|
|||||||||||||||
|
1. |
|
|
|
|
|
|
|
|
|
|
7. |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
2. |
|
|
|
|
|
|
|
|
|
|
8. |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
3. |
|
|
|
|
|
|
|
|
|
|
9. |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
4. |
|
|
|
|
|
|
|
|
|
|
10. |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
5. |
|
|
|
|
|
|
|
|
|
|
11. |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
6. |
|
|
|
|
|
|
|
|
|
|
12. |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
19.
21. PHYSICIAN’S SIGNATURE
DATE
9.2018 NC Medicaid
Form Characteristics
| Fact Name | Description |
|---|---|
| Purpose | The NC FL2 form is used for prior approval and utilization review of care levels in adult care homes for patients requiring Medicaid services. |
| Patient Information | This form collects detailed patient information, including demographics, admission details, and current and recommended levels of care. |
| Required Signatures | A physician must complete the form by providing a signature and date, certifying the accuracy of the information presented. |
| Governing Laws | The use and requirements for the NC FL2 form are governed by North Carolina Medicaid regulations and the Department of Health and Human Services guidelines. |
| Submission Process | The completed form must be submitted to the appropriate Medicaid authority for review and approval before services can be rendered. |
Guidelines on Utilizing Nc Fl2
Completing the NC FL2 form requires careful attention to detail. This form facilitates the process of obtaining prior approval for Medicaid services in an adult care home setting. Adequate preparation will ensure that all necessary information is accurately reported. Below are the steps to successfully fill out the form.
- Begin by entering the patient’s last name, first name, and middle initial in the designated fields.
- Provide the birthdate in the format of month, day, and year (M/D/Y).
- Select the sex of the patient.
- Fill in the admission date to the current location.
- Write the county and the Medicaid number assigned to the patient.
- Input the facility address.
- Insert the provider number for the facility.
- Record the name and address of the attending physician.
- Fill in the name and address of a relative or emergency contact.
- Indicate the current level of care and the recommended level of care.
- Document the prior approval number if applicable.
- Note the date approved or denied.
- List the primary and secondary admitting diagnoses, including their dates of onset.
- Provide detailed information about the patient’s functional status, such as ambulation and communication abilities.
- Describe the patient's personal care assistance needs and any special activities they require.
- Indicate any special care factors relevant to the patient’s medical condition.
- List all medications the patient is currently taking, including their strengths, dosages, and routes of administration.
- Document any pertinent x-ray and laboratory findings, along with the respective dates.
- Add any additional information that may be necessary for the review.
- Finally, obtain the physician’s signature and date the form.
What You Should Know About This Form
What is the purpose of the NC FL2 form?
The NC FL2 form is used to request prior approval for Medicaid reimbursement for adult care home services. It captures essential patient information, medical needs, and the recommended level of care. It ensures that the services provided align with Medicaid guidelines for coverage.
Who needs to complete the NC FL2 form?
The form must be completed by the attending physician. It requires detailed patient information and must be submitted to Medicaid for approval before providing specific adult care home services. Family members or facility staff may assist in gathering information, but the physician’s input is crucial.
What information is required on the NC FL2 form?
You'll need to provide the patient's full name, birthdate, admission date, Medicaid number, and the facility's address. Additionally, you'll have to disclose medical diagnoses, current and recommended levels of care, medications, and any special care factors. Detailed information enhances the chance of approval and ensures appropriate care is requested.
How is the NC FL2 form submitted?
The completed form should be submitted to the appropriate Medicaid authority, typically either online or via mail. It's essential to follow up to ensure it's been received and is in process. Keeping a copy of the form for your records is also advisable.
What happens after the NC FL2 form is submitted?
Once submitted, Medicaid will conduct a utilization review to assess the need for the requested services. You will receive a notification indicating whether the prior approval was granted or denied. This process can take some time, so be patient and follow up if you haven't received a response.
Can the NC FL2 form be appealed if denied?
Yes, if the request is denied, there is an appeal process. You can request a review by Medicaid by following the specific procedures outlined in the denial notice. Make sure to provide additional information or documentation to strengthen your case during the appeal.
Common mistakes
Filling out the NC FL2 form can be a daunting task, and mistakes often occur. One common mistake is the failure to provide accurate personal information. This includes the patient's last name, first name, and middle name. If any of this information is incorrect or missing, it can delay the approval process significantly. Always double-check these details.
Another frequent error is in the admission date. Individuals often enter the wrong date or fail to keep it updated if there are adjustments to the admission process. This detail is crucial as it sets the timeline for care and facilities involved. Ensure that this information is correct before submitting the form.
Many tend to overlook the section on medical diagnoses. It is essential to fill this out completely. Listing both primary and secondary diagnoses gives healthcare providers a comprehensive picture of the patient's needs. Incomplete or vague information in this area can hinder the review and potentially lead to a denied request for care.
Lastly, individuals commonly neglect to include the physician’s signature on the form. This is a crucial step. Without it, the form may be returned or rejected. Ensure that the attending physician reviews the form and provides their signature on the designated line. Omitting this can lead to unnecessary delays in receiving the necessary care.
Documents used along the form
The NC FL2 form serves as a pivotal document in the long-term care approval process. When navigating this often complex system, several other forms play vital roles in supporting the assessment for Medicaid services. Below is a brief overview of additional documents frequently used alongside the NC FL2 form.
- NC Medicaid Application Form: This form is essential for individuals seeking Medicaid benefits. It collects personal and financial information to determine eligibility for various healthcare services, including long-term care solutions.
- Patient Certification of Need (PCON): The PCON form is used to assess an individual's need for skilled nursing care. It requires detailed medical information, evaluations, and the specific level of care required by the patient to qualify for Medicaid-supported services.
- Prior Authorization Request: This document is necessary for obtaining pre-approval for certain medical services or procedures. It helps ensure that the requested care aligns with Medicaid rules, thus facilitating the funding process for the patient’s care needs.
- Medical History and Physical Examination Form: This form provides a comprehensive review of a patient's medical background and current health status. It is crucial for understanding the patient's overall health and assists in determining the appropriate level of care in conjunction with the NC FL2 form.
Each of these documents helps streamline processes, making it easier for patients to secure the services they need. Understanding these forms can lead to better preparation and ultimately, a smoother journey through the Medicaid approval process.
Similar forms
The NC FL2 form is essential for documenting various aspects of patient care in adult care homes. Below is a list of nine other documents that share similarities with the NC FL2 form, detailing how they are alike in purpose or content.
- CMS-1500 Form: This form is used for billing Medicare and Medicaid. Like the NC FL2, it requires patient and provider information, diagnosis details, and treatment plans.
- Narrative Summary Form: Similar in format, this document outlines a patient’s medical history and care recommendations, ensuring that all relevant details are covered.
- Patient Care Assessment Tool: This tool collects patient data to evaluate care needs. Both the NC FL2 and the assessment tool aim to determine appropriate levels of care.
- Medicaid Pre-Authorization Form: Used for seeking approval for certain services, this form includes detailed patient information like the NC FL2 to justify care requests.
- Long-Term Care Assessment Form: This document assesses eligibility for long-term care services. It includes similar patient demographics and medical information as the NC FL2.
- Discharge Planning Form: Focused on patient discharge, this form contains details about ongoing care needs and plans, akin to the discharge plan section in the NC FL2.
- Clinical Assessment Form: It provides a review of a patient's clinical status and needs, paralleling the NC FL2’s focus on assessing care requirements.
- Therapeutic Care Plan: This plan encompasses treatment goals and methods tailored to the patient’s needs, similar to the recommended level of care listed in the NC FL2.
- Personal Care Plan: This document outlines daily assistance needs for patients, echoing the personal care assistance section of the NC FL2.
Dos and Don'ts
When filling out the NC FL2 form, there are key practices to follow and avoid. Below is a list of dos and don'ts to ensure an accurate and effective submission.
- Do check all patient information for accuracy before submitting.
- Do include admission dates and diagnoses clearly.
- Do ensure all relevant signatures are included at the end of the form.
- Do provide any additional information that can clarify patient needs.
- Don't leave any fields blank unless explicitly stated.
- Don't use abbreviations that could confuse the reviewer.
- Don't submit the form without confirming compliance with all guidelines.
- Don't forget to keep a copy of the completed form for your records.
Misconceptions
Many people hold misconceptions regarding the NC FL2 form, which can lead to confusion or mistakes in the process of patient care and Medicaid services. Here are eight common misconceptions along with clarifications to enhance understanding.
- The NC FL2 form is only for nursing facility admissions. Some believe this form is exclusive to nursing homes. In reality, this form is used for various levels of care including intermediate care facilities and domiciliary care units.
- You don’t need a physician’s signature. Many might think that the form can be submitted without a doctor's approval. However, a physician's signature is mandatory as the form reflects medical necessity for the recommended level of care.
- The form is optional if the patient is already receiving care. Some individuals think that once a patient is admitted, they can bypass the FL2 form. This is incorrect; the form must still be completed to ensure proper Medicaid coverage and compliance.
- Filling out the FL2 form is straightforward and easy. While the form may seem like a simple document, it requires detailed medical and personal information regarding the patient’s condition and care needs, which can complicate the completion process.
- All nursing homes have the same requirements for the FL2 form. This is misleading. Each facility may have specific requirements or preferences for how the form should be completed or submitted, so it's vital to check with the facility beforehand.
- Once submitted, the FL2 form guarantees approval for services. It is a common belief that filling out the form will automatically result in Medicaid approval. However, the form initiates a review process, and approval is subject to Medicaid guidelines and eligibility criteria.
- You only need to submit the FL2 form at the time of admission. Some assume the form is required only during the initial admission. In fact, it may need to be resubmitted or updated regularly based on changes in patient condition or care level.
- All pieces of information on the form are equally important. While every section has its place, some individuals might underestimate the significance of specific details, such as medical diagnoses or care recommendations, which are crucial for determining eligibility.
Understanding these misconceptions can help individuals approach the NC FL2 form with a clearer perspective, ensuring a smoother process in securing necessary care for patients.
Key takeaways
Here are some key takeaways for filling out and using the NC FL2 form:
- Complete All Sections: Ensure that every section of the form is filled out completely. Missing information can lead to delays in approval.
- Patient Identification: Begin with accurate patient details like name, birthdate, and Medicaid number. This information is critical for processing.
- Medical History: List all admitting diagnoses, including primary and secondary conditions. Dates of onset are also necessary.
- Current and Recommended Levels of Care: Clearly indicate the patient's current level of care and the level that is being recommended.
- Medication Details: Provide extensive details about all medications the patient is taking, including name, strength, dosage, and route.
- Special Care Factors: Note any special care needs and frequency. This helps assess the required level of support for the patient.
- Signature Requirement: Don't forget that a physician's signature and date are required at the end of the form for it to be valid.
Following these points carefully will help ensure that the form functions as intended and supports the patient's care needs effectively.
Browse Other Templates
Jps Connection Application Form - Specific timelines regarding residence can influence eligibility.
Ucda Bill of Sale - The appraisal date needs to be clearly marked as January 1st.
Parent Sample Letter to Judge for Child Custody - Digital submissions may require electronic signatures on this form.