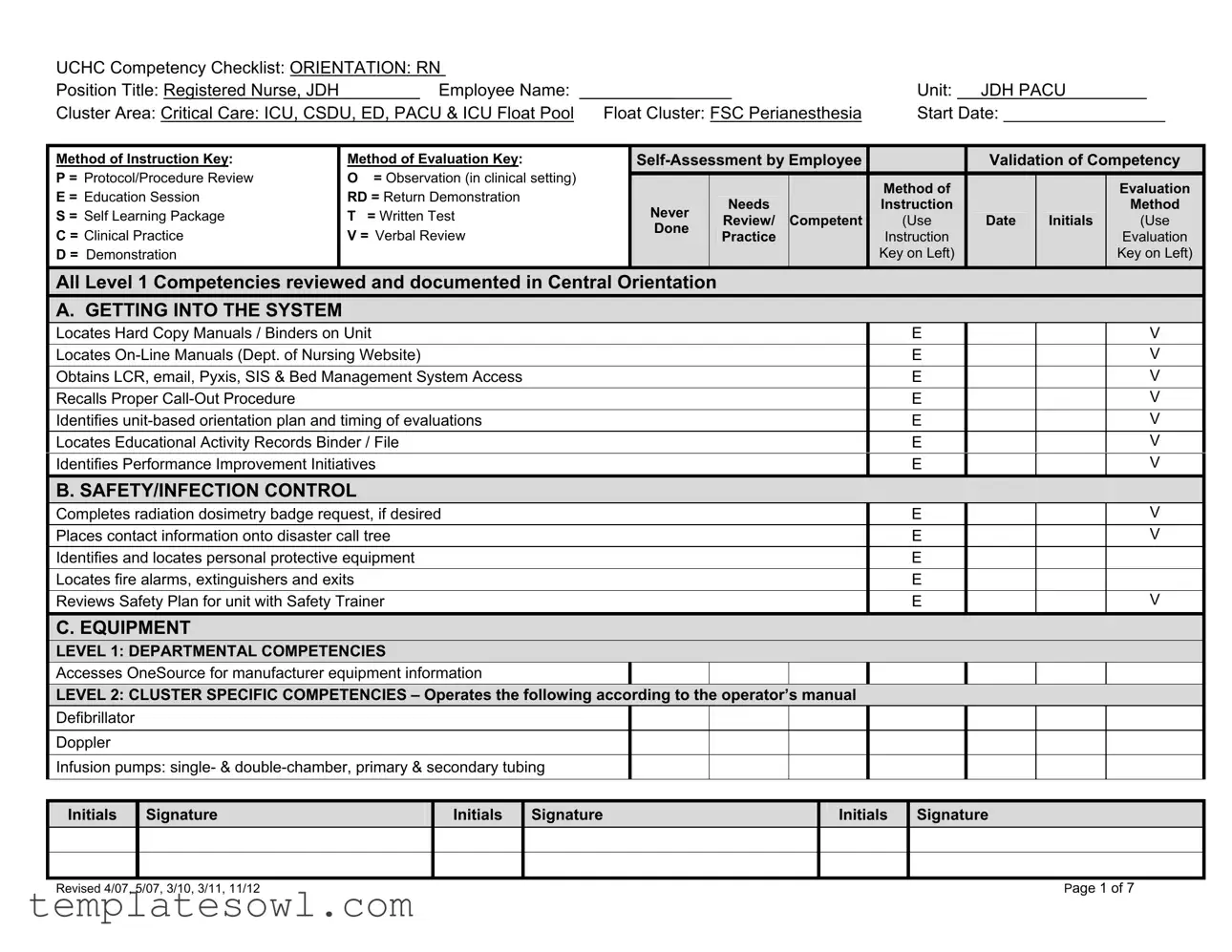
Fill Out Your Nursing Competency Checklist Form
The Nursing Competency Checklist is an essential tool designed to ensure that registered nurses meet the necessary skills and knowledge required in critical care settings. This comprehensive form provides a structured framework for evaluating nursing competencies across various dimensions, including orientation, safety, equipment operation, documentation, and providing care. It allows nursing staff to assess their proficiency in locating vital resources such as manuals, electronic systems, and emergency procedures. Safety protocols and infection control measures are also prioritized within the checklist, ensuring that all staff members are well-prepared for potential health hazards. Furthermore, the checklist evaluates the operation of critical equipment, emphasizing the importance of adhering to manufacturer guidelines. Documentation and communication skills are thoroughly addressed, enabling nurses to manage patient information accurately and effectively. Finally, specific care protocols relevant to the unit are included, ensuring that nurses understand and comply with best practices in patient care. Overall, this checklist not only assists in individual assessments but also contributes to improving the quality of care provided in the healthcare environment.
Nursing Competency Checklist Example
|
UCHC Competency Checklist: ORIENTATION: RN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
Position Title: Registered Nurse, JDH |
|
|
Employee Name: ________________ |
|
|
Unit: |
|
|
JDH PACU |
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Cluster Area: Critical Care: ICU, CSDU, ED, PACU & ICU Float Pool |
Float Cluster: FSC Perianesthesia |
|
|
Start Date: _________________ |
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
Method of Instruction Key: |
|
Method of Evaluation Key: |
|
|
|
|
|
|
Validation of Competency |
||||||||||||||||||||||
|
P = Protocol/Procedure Review |
|
O = Observation (in clinical setting) |
|
|
|
|
|
|
|
|
|
|
|
Method of |
|
|
|
|
|
|
|
|
Evaluation |
|
|||||||
|
E = Education Session |
|
RD = Return Demonstration |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
Never |
|
|
Needs |
|
|
|
|
|
Instruction |
|
|
|
|
|
|
|
|
Method |
|
|||||||||
|
S = Self Learning Package |
|
T = Written Test |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
Review/ |
|
C |
ompetent |
|
(Use |
|
|
Date |
|
|
Initials |
|
|
(Use |
|
|||||||||||
|
|
|
|
Done |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
C = Clinical Practice |
|
V = Verbal Review |
|
|
|
|
Practice |
|
|
|
|
|
Instruction |
|
|
|
|
|
|
|
|
Evaluation |
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
D = Demonstration |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Key on Left) |
|
|
|
|
|
|
|
|
Key on Left) |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
All Level 1 Competencies reviewed and documented in Central Orientation |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
A. GETTING INTO THE SYSTEM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Locates Hard Copy Manuals / Binders on Unit |
|
|
|
|
|
|
|
|
|
|
|
|
E |
|
|
|
|
|
|
|
|
|
V |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Locates |
|
|
|
|
|
|
|
|
|
|
|
|
E |
|
|
|
|
|
|
|
|
|
V |
||||||||
|
Obtains LCR, email, Pyxis, SIS & Bed Management System Access |
|
|
|
|
|
|
|
|
|
|
|
|
E |
|
|
|
|
|
|
|
|
|
V |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Recalls Proper |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
E |
|
|
|
|
|
|
|
|
|
V |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Identifies |
|
|
|
|
|
|
|
|
|
|
|
|
E |
|
|
|
|
|
|
|
|
|
V |
||||||||
|
Locates Educational Activity Records Binder / File |
|
|
|
|
|
|
|
|
|
|
|
|
E |
|
|
|
|
|
|
|
|
|
V |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Identifies Performance Improvement Initiatives |
|
|
|
|
|
|
|
|
|
|
|
|
E |
|
|
|
|
|
|
|
|
|
V |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
B. SAFETY/INFECTION CONTROL |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
Completes radiation dosimetry badge request, if desired |
|
|
|
|
|
|
|
|
|
|
|
|
E |
|
|
|
|
|
|
|
|
|
V |
||||||||
|
Places contact information onto disaster call tree |
|
|
|
|
|
|
|
|
|
|
|
|
E |
|
|
|
|
|
|
|
|
|
V |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
Identifies and locates personal protective equipment |
|
|
|
|
|
|
|
|
|
|
|
|
E |
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
Locates fire alarms, extinguishers and exits |
|
|
|
|
|
|
|
|
|
|
|
|
E |
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Reviews Safety Plan for unit with Safety Trainer |
|
|
|
|
|
|
|
|
|
|
|
|
E |
|
|
|
|
|
|
|
|
|
V |
||||||||
|
C. EQUIPMENT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
LEVEL 1: DEPARTMENTAL COMPETENCIES |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
Accesses OneSource for manufacturer equipment information |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
LEVEL 2: CLUSTER SPECIFIC COMPETENCIES – Operates the following according to the operator’s manual |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
Defibrillator |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Doppler |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
Infusion pumps: single- & |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Initials |
Signature |
|
|
Initials |
Signature |
|
|
|
|
|
|
|
|
|
Initials |
Signature |
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Revised 4/07, 5/07, 3/10, 3/11, 11/12 |
Page 1 of 7 |

UCHC Competency Checklist: ORIENTATION: RN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Position Title: Registered Nurse, JDH |
|
|
Employee Name: ________________ |
|
|
Unit: |
|
|
JDH PACU |
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cluster Area: Critical Care: ICU, CSDU, ED, PACU & ICU Float Pool |
Float Cluster: FSC Perianesthesia |
|
|
Start Date: _________________ |
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Method of Instruction Key: |
Method of Evaluation Key: |
|
|
|
|
|
|
|
Validation of Competency |
|||||||||||||||||||||
P = Protocol/Procedure Review |
O = Observation (in clinical setting) |
|
|
|
|
|
|
|
|
|
|
|
Method of |
|
|
|
|
|
|
|
|
Evaluation |
|
|||||||
E = Education Session |
RD = Return Demonstration |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
Never |
|
|
Needs |
|
|
|
|
|
Instruction |
|
|
|
|
|
|
|
|
Method |
|
||||||||
S = Self Learning Package |
T = Written Test |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
Review/ |
|
C |
ompetent |
|
|
(Use |
|
|
Date |
|
|
Initials |
|
|
(Use |
|
|||||||||
|
|
|
Done |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
C = Clinical Practice |
V = Verbal Review |
|
|
|
|
|
Practice |
|
|
|
|
|
Instruction |
|
|
|
|
|
|
|
|
Evaluation |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
D = Demonstration |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Key on Left) |
|
|
|
|
|
|
|
|
Key on Left) |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Infusion pumps: syringe |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Oxygen delivery: cannula, flow meter, mask, |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Pulse Oximeter |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Pyxis Machine(s) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Suction: Continuous/Intermittent |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Twelve Lead ECG Machine |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
LEVEL 3: JDH |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
Bair Hugger |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Code Cart |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Hemodynamic monitoring: arterial line |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Hemodynamic monitoring: central venous pressure |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Intubation Box |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Malignant Hyperthermia supply boxes |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Medication Lockboxes |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Monitors – GE Carescape B650 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Outside Entry Door |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Pediatric Anesthesia Cart |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Pulsatile |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Pumps - Epidural |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Pumps - PCA |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Radial Hemostasis Bands |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Initials |
Signature |
|
|
Initials |
Signature |
|
|
|
|
|
|
|
|
|
Initials |
Signature |
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Revised 4/07, 5/07, 3/10, 3/11, 11/12 |
Page 2 of 7 |

|
UCHC Competency Checklist: ORIENTATION: RN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
Position Title: Registered Nurse, JDH |
|
|
Employee Name: ________________ |
|
|
Unit: |
|
|
JDH PACU |
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cluster Area: Critical Care: ICU, CSDU, ED, PACU & ICU Float Pool |
Float Cluster: FSC Perianesthesia |
|
|
Start Date: _________________ |
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
Method of Instruction Key: |
|
Method of Evaluation Key: |
|
|
|
|
|
|
Validation of Competency |
||||||||||||||||||||||
|
P = Protocol/Procedure Review |
|
O = Observation (in clinical setting) |
|
|
|
|
|
|
|
|
|
|
|
Method of |
|
|
|
|
|
|
|
|
Evaluation |
|
|||||||
|
E = Education Session |
|
RD = Return Demonstration |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
Never |
|
|
Needs |
|
|
|
|
|
Instruction |
|
|
|
|
|
|
|
|
Method |
|
|||||||||
|
S = Self Learning Package |
|
T = Written Test |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
Review/ |
|
C |
ompetent |
|
(Use |
|
|
Date |
|
|
Initials |
|
|
(Use |
|
|||||||||||
|
|
|
|
Done |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
C = Clinical Practice |
|
V = Verbal Review |
|
|
|
|
Practice |
|
|
|
|
|
Instruction |
|
|
|
|
|
|
|
|
Evaluation |
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
D = Demonstration |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Key on Left) |
|
|
|
|
|
|
|
|
Key on Left) |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Regional Anesthesia Cart |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Ventilators |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
D. DOCUMENTATION/COMMUNICATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
LEVEL 1: DEPARTMENTAL COMPETENCIES |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
Accesses email account |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Accesses patient information in LCR |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Aware of patient information in eHIMS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Locates link to Patient Safety Net |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
Adheres to customer service values of UCHC (telephone, interpersonal) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
LEVEL 2: CLUSTER SPECIFIC COMPETENCIES |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
Initiates and documents discharge teaching to patients & families |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
States proper time frames for completion of various documentation |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
LEVEL 3: UNIT SPECIFIC COMPETENCIES |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
Accesses information from Physician Postop Note/Orders & Progress Notes |
|
|
|
|
|
|
|
|
|
|
|
V / O |
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Completes documentation |
|
|
|
|
|
|
|
|
|
|
|
V / O |
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Completes forms/requisitions |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
V / O |
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Completes ISBAR forms (2) appropriately |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
V / O |
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Explains use of |
|
|
|
|
|
|
|
|
|
|
|
V / O |
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Generates medication reconciliation forms and report reprints from SIS |
|
|
|
|
|
|
|
|
|
|
|
V / O |
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Identifies correctly completed History & Physical |
|
|
|
|
|
|
|
|
|
|
|
V / O |
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Identifies correctly completed Informed Consent – Procedure & Transfusion |
|
|
|
|
|
|
|
|
|
|
|
V / O |
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Initials |
Signature |
|
|
Initials |
Signature |
|
|
|
|
|
|
|
|
|
Initials |
Signature |
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Revised 4/07, 5/07, 3/10, 3/11, 11/12 |
Page 3 of 7 |

|
UCHC Competency Checklist: ORIENTATION: RN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Position Title: Registered Nurse, JDH |
|
|
Employee Name: ________________ |
|
|
|
Unit: |
|
|
JDH PACU |
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cluster Area: Critical Care: ICU, CSDU, ED, PACU & ICU Float Pool |
Float Cluster: FSC Perianesthesia |
|
|
|
Start Date: _________________ |
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Method of Instruction Key: |
Method of Evaluation Key: |
|
|
|
|
|
|
|
|
Validation of Competency |
|||||||||||||||||||||
|
P = Protocol/Procedure Review |
O = Observation (in clinical setting) |
|
|
|
|
|
|
|
|
|
|
|
Method of |
|
|
|
|
|
|
|
|
Evaluation |
|
||||||||
|
E = Education Session |
RD = Return Demonstration |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
Never |
|
|
Needs |
|
|
|
|
|
Instruction |
|
|
|
|
|
|
|
|
Method |
|
|||||||||
|
S = Self Learning Package |
T = Written Test |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
Review/ |
|
C |
ompetent |
|
|
(Use |
|
|
Date |
|
|
Initials |
|
|
(Use |
|
||||||||||
|
|
|
|
Done |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
C = Clinical Practice |
V = Verbal Review |
|
|
|
|
|
Practice |
|
|
|
|
|
Instruction |
|
|
|
|
|
|
|
|
Evaluation |
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
D = Demonstration |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Key on Left) |
|
|
|
|
|
|
|
|
Key on Left) |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Locates Face Sheet – Locker Assignment Notation |
|
|
|
|
|
|
|
|
|
|
|
|
|
V / O |
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
Recognizes printed orders / accesses POE orders correctly |
|
|
|
|
|
|
|
|
|
|
|
|
|
V / O |
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
Refers to Patient Belongings Log – Valuables Checklist |
|
|
|
|
|
|
|
|
|
|
|
|
|
V / O |
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
States proper time frames for completion of various documentation |
|
|
|
|
|
|
|
|
|
|
|
|
|
V / O |
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
E. PROVISION OF CARE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
HOSPITAL ADMINISTRATIVE MANUAL– aware of content and/or provides care according to the following protocols/procedures: |
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
Consent – Procedural |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Consent / Refusal of Blood and/or Blood Products |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
History & Physical |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Medical Orders |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Universal Protocol |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
NURSING PRACTICE MANUAL – aware of content and/or provides care according to the following protocols/procedures: |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
Blanket / Solution Warmers |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Central Lines – (Blood Draws, Flush, IV Fluid Administration, & Dressing Care) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Chest Tube |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
CPAP and BiPAP Units: for use during Hospital Stay |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Diabetes Mellitus Management: Periprocedural Care |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Hemodynamic Monitoring |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
IV Therapy: Peripheral |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
IV Push Medications |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
Jewelry: Wearing of Jewelry and Body Piercings during … Procedures |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Medications: Double Check |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Neurologic Assessment of the Adult Inpatient |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Initials |
Signature |
|
|
Initials |
Signature |
|
|
|
|
|
|
|
|
|
Initials |
|
Signature |
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Revised 4/07, 5/07, 3/10, 3/11, 11/12 |
Page 4 of 7 |

UCHC Competency Checklist: ORIENTATION: RN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Position Title: Registered Nurse, JDH |
|
|
Employee Name: ________________ |
|
|
Unit: |
|
|
JDH PACU |
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cluster Area: Critical Care: ICU, CSDU, ED, PACU & ICU Float Pool |
Float Cluster: FSC Perianesthesia |
|
|
Start Date: _________________ |
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Method of Instruction Key: |
Method of Evaluation Key: |
|
|
|
|
|
|
|
Validation of Competency |
|||||||||||||||||||||
P = Protocol/Procedure Review |
O = Observation (in clinical setting) |
|
|
|
|
|
|
|
|
|
|
|
Method of |
|
|
|
|
|
|
|
|
Evaluation |
|
|||||||
E = Education Session |
RD = Return Demonstration |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
Never |
|
|
Needs |
|
|
|
|
|
Instruction |
|
|
|
|
|
|
|
|
Method |
|
||||||||
S = Self Learning Package |
T = Written Test |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
Review/ |
|
C |
ompetent |
|
|
(Use |
|
|
Date |
|
|
Initials |
|
|
(Use |
|
|||||||||
|
|
|
Done |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
C = Clinical Practice |
V = Verbal Review |
|
|
|
|
|
Practice |
|
|
|
|
|
Instruction |
|
|
|
|
|
|
|
|
Evaluation |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
D = Demonstration |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Key on Left) |
|
|
|
|
|
|
|
|
Key on Left) |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Pain: Care of the Adult |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Pain: Continuous Narcotic Infusion |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Pain: Epidural Narcotic Infusion and Patient Controlled Epidural Analgesia |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Pain: Narcotics via PCA Pump |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Restraints: Acute Medical/Surgical |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Transportation: Inpatients |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
UNIT PRACTICE MANUAL - aware of content and/or provides care according to the following protocols/procedures: |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
Anesthesia, Spinal & Epidural: Perioperative Care |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Cardiovascular Monitoring: Perioperative Care |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
DOC Patients in Perioperative Area |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Discharge from PACU: Ambulatory Patients (Phase 2) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Discharge from PACU: Inpatients (Phase 1) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Documentation: Perioperative Electronic and |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Extended PACU Stay |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Falls: Perioperative Risk Identification |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Flolan: Perioperative Care |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Hysteroscopy: Perioperative Care |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Implanted Electronic Cardiac Devices |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
IV Catheter Removal: MA |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
IV Catheters: Problem Insertion |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
IV Push Medications: Perianesthetic Approved |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Latex Allergy Care |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Malignant Hyperthermia: Perioperative Care |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Initials |
Signature |
|
|
Initials |
Signature |
|
|
|
|
|
|
|
|
|
Initials |
Signature |
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Revised 4/07, 5/07, 3/10, 3/11, 11/12 |
Page 5 of 7 |
UCHC Competency Checklist: ORIENTATION: RN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Position Title: Registered Nurse, JDH |
|
Employee Name: ________________ |
|
Unit: |
|
|
JDH PACU |
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cluster Area: Critical Care: ICU, CSDU, ED, PACU & ICU Float Pool |
Float Cluster: FSC Perianesthesia |
|
Start Date: _________________ |
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Method of Instruction Key: |
|
Method of Evaluation Key: |
|
|
|
|
|
Validation of Competency |
||||||||||||||||||
P = Protocol/Procedure Review |
|
O = Observation (in clinical setting) |
|
|
|
|
|
|
|
|
|
|
Method of |
|
|
|
|
|
|
|
|
Evaluation |
|
|||
E = Education Session |
|
RD = Return Demonstration |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
Never |
|
|
Needs |
|
|
|
|
Instruction |
|
|
|
|
|
|
|
|
Method |
|
|||||
S = Self Learning Package |
|
T = Written Test |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
Review/ |
|
C |
ompetent |
|
(Use |
|
|
Date |
|
|
Initials |
|
|
(Use |
|
||||||
|
|
|
Done |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
C = Clinical Practice |
|
V = Verbal Review |
|
|
|
|
Practice |
|
|
|
|
Instruction |
|
|
|
|
|
|
|
|
Evaluation |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
D = Demonstration |
|
|
|
|
|
|
|
|
|
|
|
|
|
Key on Left) |
|
|
|
|
|
|
|
|
Key on Left) |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Nausea & Vomiting: Perioperative Care |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Nerve Blockade, Regional and Peripheral |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
PACU Admission |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Pain and Comfort Management: Perioperative |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Respiratory Compromise Management: Perioperative Care |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Skin Care: Perioperative Care |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Thermoregulation and Prevention of Unplanned Hypothermia |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Tonsillectomy: Postoperative Care |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Visitors & Observers in the Perioperative Area |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
PRACTICUMS & SKILL VALIDATIONS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Anesthesia Observation |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Arrhythmia Course (or passing exam in GNO) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
ICU Rotation (inexperienced staff) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Phlebotomy practicum |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Preoperative Experience |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
IV Insertion #1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
IV Insertion #2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
IV Insertion #3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
JDH PACU to FSC PACU Float Experience
B. SAFETY/INFECTION CONTROL
Initials Signature
Initials Signature
Initials Signature
Revised 4/07, 5/07, 3/10, 3/11, 11/12 |
Page 6 of 7 |

UCHC Competency Checklist: ORIENTATION: RN |
|
|
|
|
|
|
|||||
Position Title: Registered Nurse, JDH |
Employee Name: ________________ |
Unit: JDH PACU |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
Cluster Area: Critical Care: ICU, CSDU, ED, PACU & ICU Float Pool Float Cluster: FSC Perianesthesia |
Start Date: _________________ |
||||||||||
|
|
|
|
|
|
|
|
|
|
||
Identifies and locates personal protective equipment |
|
|
|
|
E |
|
|
|
|
||
Locates fire alarms, extinguishers and exits |
|
|
|
|
E |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
C. EQUIPMENT |
|
|
|
|
|
|
|
|
|
|
|
Code Cart |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
IV Cart |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Monitors – Dash |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Narcotics Security System |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Nurse Call System |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Regional Block Cart |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Scale - electronic |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Initials Signature
Initials Signature
Initials Signature
Revised 4/07, 5/07, 3/10, 3/11, 11/12 |
Page 7 of 7 |
Form Characteristics
| Fact Name | Description |
|---|---|
| Purpose | The Nursing Competency Checklist is designed to assess and validate essential skills and knowledge for Registered Nurses in a clinical setting. |
| Orientation Requirement | Completion of the checklist is a mandatory part of the orientation process for all new Registered Nurses (RNs) employed at JDH. |
| Instruction Methods | Various instructional methods include self-assessment, observation, education sessions, and return demonstrations. |
| Evaluation Methods | The checklist utilizes different evaluation methods, including written tests, verbal reviews, and clinical practice assessments. |
| Compliance Tracking | All Level 1 competencies must be reviewed and documented in Central Orientation for compliance tracking. |
| Safety Protocols | The checklist emphasizes safety and infection control, requiring nurses to complete safety-related tasks and training. |
| Equipment Competencies | Nurses are required to demonstrate competency in operating crucial medical equipment, including defibrillators and infusion pumps. |
| State Governing Laws | Specific laws governing nursing practices vary by state and can impact training and competency requirements; refer to local regulations for details. |
Guidelines on Utilizing Nursing Competency Checklist
Completing the Nursing Competency Checklist form is essential for ensuring that all required competencies are assessed and validated for new Registered Nurses. The form should be filled out carefully to provide a comprehensive overview of each competency. The steps below guide you through the process of accurately completing this document.
- Gather Information: Before starting, collect your personal details, including your name, start date, and unit information.
- Enter Personal Details: Fill in your name, position title (Registered Nurse), unit (JDH PACU), and start date in the designated fields at the top of the form.
- Select Method of Instruction and Evaluation: Familiarize yourself with the key provided for the methods of instruction and evaluation. Mark the appropriate boxes corresponding to each competency being assessed.
- Complete Each Competency Section: Go through the sections: A (Getting Into the System), B (Safety/Infection Control), C (Equipment), D (Documentation/Communication), and E (Provision of Care). Mark the appropriate columns as you complete each competency based on your assessment and validation.
- Initial and Sign: For each competency you complete, provide your initials in the appropriate space provided. Ensure that the evaluation is clear and indicates whether you are competent or need further instruction.
- Submit the Checklist: Once all sections are filled out, submit the completed checklist to your supervisor or the designated personnel for review and recording.
Completing the Nursing Competency Checklist serves to validate and document knowledge and skills essential for safe nursing practice. Keeping a clear record is beneficial for both personal growth and compliance with institutional requirements.
What You Should Know About This Form
What is the Nursing Competency Checklist form?
The Nursing Competency Checklist form is a structured tool designed to assess the skills and competencies of registered nurses during their orientation process. It ensures that new hires demonstrate the necessary knowledge and abilities required to perform in their roles effectively. The checklist covers various competencies, including safety protocols, equipment operation, documentation, and patient care standards.
Who needs to complete this checklist?
All newly hired registered nurses (RNs) in the JDH PACU, Critical Care Units, or other designated clusters are required to complete the Nursing Competency Checklist. This form is crucial for ensuring that each nurse meets the specific expectations and standards of practice within their respective unit.
What are the key components of the checklist?
The checklist encompasses several key areas, including orientation procedures, safety and infection control protocols, equipment competencies, documentation practices, and provision of care. Each section assesses specific skills and knowledge, helping to validate that the nurse is prepared to deliver safe and effective patient care.
How is competency evaluated using this checklist?
Competency evaluation occurs through multiple methods outlined in the checklist. Nurses undergo self-assessments, direct observations, and demonstrations of skills in a clinical setting. In addition, completion of educational sessions and return demonstrations may be required to show proficiency with equipment and procedures.
What happens if a nurse does not meet the competency requirements?
If a nurse does not meet the required competencies outlined in the checklist, a plan for additional training or remediation will be developed. This may include further education sessions, practice opportunities, or one-on-one guidance. The aim is to ensure that the nurse achieves the necessary skills to fulfill their role before they assume full responsibilities.
How often is the checklist updated?
The Nursing Competency Checklist is periodically reviewed and updated to reflect current best practices, regulatory standards, and any changes in equipment or protocols. This ensures that the checklist remains a relevant and effective tool for assessing nursing competencies.
Where can nurses access or submit their completed checklist?
Nurses can access the Nursing Competency Checklist typically from their unit's educational resources or the Department of Nursing website. Upon completion, the checklist should be submitted to the designated individual within their unit, such as the nurse educator or manager, for review and documentation in the nurse's personnel file.
Common mistakes
When filling out the Nursing Competency Checklist form, there are common mistakes that individuals often make. Awareness of these errors can streamline the process and ensure that competencies are accurately documented.
Firstly, many people neglect to complete the Employee Name and Start Date sections. Omitting these critical details can lead to confusion and delays in processing the documentation. Without this information, it becomes challenging to track who is being evaluated and when they started their role.
Secondly, failing to specify the method of instruction or evaluation is another common oversight. Each competency should be assessed with a clearly defined method, such as observation or written tests. Not indicating this can compromise the validity of the evaluation, making it difficult to ascertain how skills were measured.
Additionally, some individuals make the mistake of not initialing once they have completed each section. Missing initials fail to provide verification that the task has been completed. Each section should not only be checked off but also initialed to show personal accountability.
Another frequent error is overlooking the need for periodic reviews of competencies. Some may assume that once they have filled out the checklist, no further action is required. Regular reviews ensure continued adherence to standards, especially as procedures and protocols evolve.
Poor documentation is also a prevalent issue. Some nurses may write vague notes or leave fields incomplete, which can mislead evaluators. Each competency should be documented clearly, providing specific examples when possible.
Furthermore, without a solid understanding of the relevant policies and procedures, applicants might inaccurately assess their competencies. Familiarity with the Nursing Practice Manual and Hospital Administrative Manual is vital. A lack of knowledge can cause individuals to overlook important competencies.
Some individuals also misunderstand the meaning of terms used in the checklist. Using 'never needs instruction' when a competency is only partially understood can misrepresent their capabilities. It is important to evaluate honestly and accurately.
When accessing documents or resources, delays in finding the necessary manuals can hinder completion. Failing to prepare in advance by knowing where resources are located can lead to unnecessary wait times and missed evaluations.
Finally, not engaging with mentors or trainers during the checklist process can serve as a barrier. Seeking guidance often leads to a better understanding of competencies and enhances one's overall preparedness for evaluations. Building a collaborative approach can significantly improve the quality of submissions.
Documents used along the form
The Nursing Competency Checklist form is an essential document for assessing the skills and competencies of registered nurses during their orientation. However, several other forms and documents are commonly used alongside it to ensure comprehensive evaluation and compliance with healthcare standards. Here are some of those additional documents.
- Performance Improvement Plans: These documents outline specific areas where a nurse's performance may need enhancement. They establish goals, strategies, and timelines for improvement.
- Clinical Practice Guidelines: Written protocols provide evidence-based practices for various procedures and patient care scenarios. They serve as a reference for nurses to follow in their daily practice.
- Patient Safety Reports: Documenting incidents related to patient safety helps identify trends and areas for improvement. These reports can be vital for training and accountability.
- Accreditation Standards: These guidelines from accrediting bodies ensure facilities meet established healthcare standards. Familiarization with these standards is essential for nurses in clinical settings.
- Self-Assessment Tools: Used by nurses to evaluate their own strengths and weaknesses, these tools help promote personal growth and professional development.
- Documentation Policies: These outlines detail how nurses should maintain and document patient care records. They ensure clarity, compliance with legal standards, and proper communication.
- Training Manuals: Comprehensive guides that include protocols, equipment usage, and organizational policies. They provide in-depth knowledge essential for effective patient care.
Utilizing these documents in conjunction with the Nursing Competency Checklist helps create a thorough orientation process. This thoroughness ultimately supports high-quality patient care and elevates the overall performance of nursing staff.
Similar forms
- Skills Competency Checklist: Similar to the Nursing Competency Checklist, this document outlines essential skills and procedures a healthcare worker must demonstrate proficiency in, focusing on clinical skills and practices.
- Employee Orientation Checklist: This checklist ensures that new employees complete all necessary trainings and orientation sessions, documenting each item and providing a record similar to the competency evaluation.
- Clinical Practice Evaluation Form: This form captures data on clinical performance, aligning closely with competency validation by tracking specific actions and decisions made in patient care.
- Medication Administration Record (MAR): The MAR serves as a formal log for tracking medication administration, similar to how the Nursing Competency Checklist tracks specific competencies and actions for nurses.
- Patient Care Plan Template: This document outlines expected nursing interventions and outcomes for patients, much like how competences are defined and measured in the checklist.
- Quality Improvement Audit Tool: Both tools measure competency and compliance in specific practices. This audit tool assesses adherence to established protocols, similar to a competency checklist.
- Nursing Competency Validation Tool: This form provides a means to assess nursing skills and knowledge according to established standards, closely mirroring the purpose of the Nursing Competency Checklist.
- Infection Control Practices Checklist: This document audits compliance with infection control policies, akin to how the Nursing Competency Checklist assesses adherence to safety and infection protocols.
- Staff Development Plan: Like the Nursing Competency Checklist, this plan identifies needed training and development for staff to ensure they meet competency standards within their roles.
- Patient Safety Incident Report: Both documents document potential safety issues and provide data on nursing performance. Investigation and analysis of incidents can involve similar methodologies as the competencies outlined in the checklist.
Dos and Don'ts
Here are ten things to consider when filling out the Nursing Competency Checklist form:
- Ensure all personal information, including your name and start date, is accurate and complete.
- Read each competency carefully before marking it, as this helps in understanding expectations.
- Utilize the provided method of evaluation key to appropriately assess your competencies.
- Consult available resources, such as manuals and training guides, when unsure about specific competencies.
- Document any completed competencies immediately to maintain current records.
Here are five things to avoid when completing the form:
- Do not leave any sections of the checklist blank unless specified; it may lead to confusion regarding your competencies.
- Avoid marking a competency as "Done" or "Competent" without sufficient practice or confidence.
- Do not rush through the evaluation process; take your time to ensure accuracy.
- Refrain from using abbreviations or unclear terminology that may not be widely understood.
- Do not submit the form without a thorough review to catch potential errors and confirm completeness.
Misconceptions
Here are some common misconceptions about the Nursing Competency Checklist form:
- It only addresses basic nursing tasks. Many believe that the checklist only covers foundational skills. In reality, it includes advanced competencies relevant to various clinical situations, ensuring that nurses are well-prepared for complex care.
- Completing the checklist guarantees competency. While the checklist is a valuable tool for evaluation, completing it does not automatically mean that a nurse is competent. Ongoing assessment and practical application of skills are essential for true competency.
- Self-assessment is less important than observation. Some think that observation is the only valid way to assess skills. However, self-assessment also plays a crucial role in understanding personal strengths and areas for improvement in nursing practice.
- All competencies are assessed at the same time. Many believe that the checklist requires all competencies to be completed in one session. In fact, it allows for flexibility and can be completed over time, accommodating individual learning paces.
- The checklist is only for new hires. There is a misconception that only new employees should use the checklist. Existing staff also benefit from regularly reviewing and updating their competencies, ensuring ongoing professional development.
Key takeaways
- Understand the purpose of the Nursing Competency Checklist. It serves as a tool to verify skills and knowledge for a Registered Nurse.
- The checklist is structured by unit-specific and departmental competencies to ensure that all relevant skills are covered.
- Access the Hard Copy and Online Manuals which contain important information related to procedures and protocols.
- Use various methods of evaluation, such as observation and self-assessment, to gauge competencies effectively.
- Ensure completion of required documentation on skills acquired during orientation. It is essential for future validations.
- Engage in safety and infection control practices according to the outlined protocols, as patient safety is paramount.
- Familiarize yourself with the equipment that you will be using, and ensure proficiency before operating these devices.
- Prioritize communication skills. Access patient information and document interactions according to established protocols.
- Participate actively in educational sessions and seek guidance from peers if uncertainty arises during practice.
- Regularly review and update your competency skills to stay aligned with best practices and institutional changes.
Browse Other Templates
Form W-8ben-e - Providing this form helps confirm your foreign income status.
Ohio State Tax Forms - Vendor license information is crucial to properly identify the seller on the form.
New York Sales Tax Rate - Privacy notice alerts you that personal information collected will be used for tax administration purposes.