Fill Out Your Nwcc 1 Form
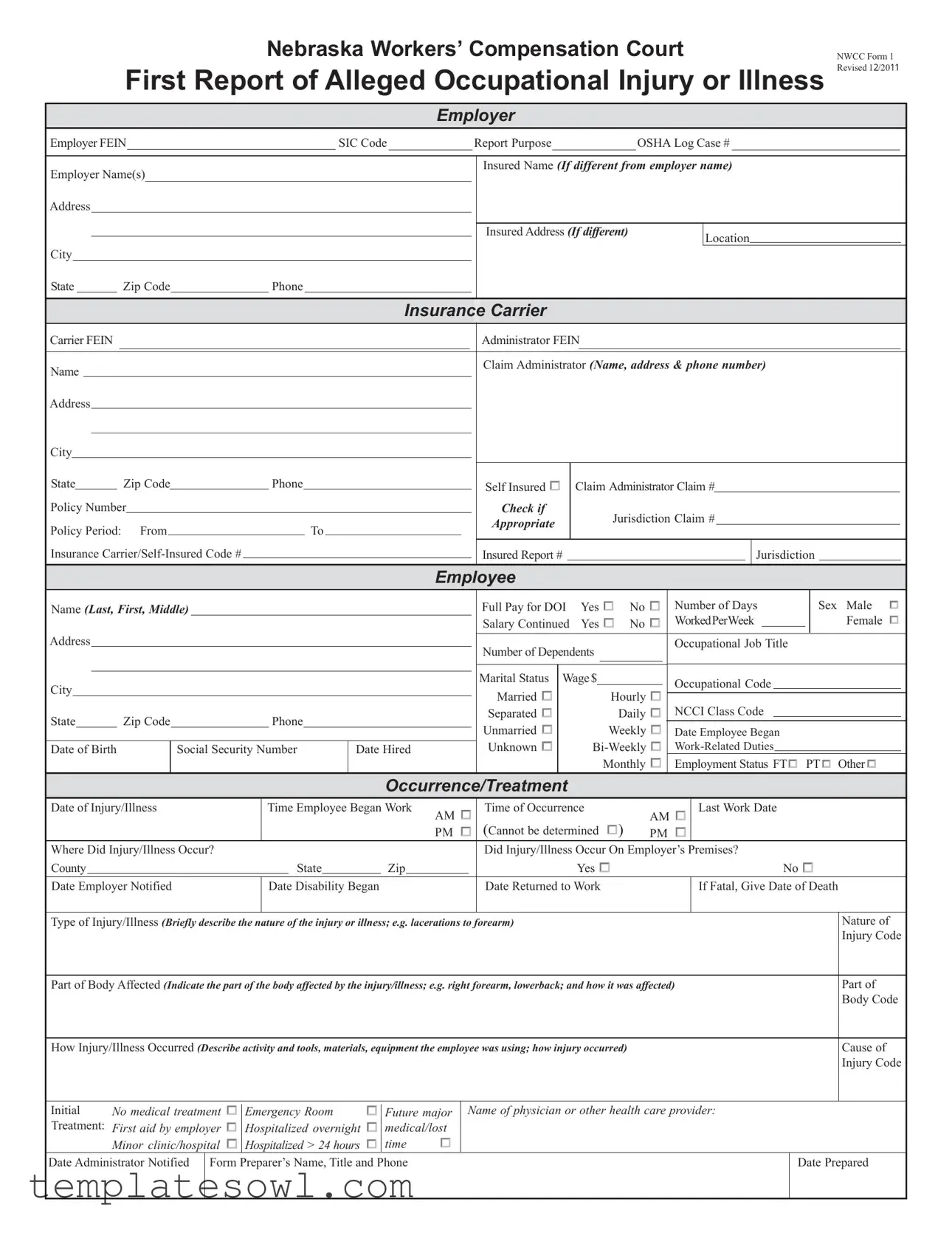
The NWCC 1 form, also known as the First Report of Alleged Occupational Injury or Illness, is a crucial document for both employers and employees in Nebraska’s workers' compensation system. This form serves as the initial communication to the Nebraska Workers’ Compensation Court concerning a work-related injury or illness. It captures essential details such as the employer's information, including their Federal Employer Identification Number (FEIN) and Standard Industrial Classification (SIC) code, which clarifies the nature of the business. The employee's information is equally vital, requiring personal details like their full name, Social Security Number, and employment status, along with specifics about the occurrence of the injury or illness. This includes the date and time of the incident, location, and a description of how it happened. Additionally, the form includes sections for health care provider details and information regarding initial treatment received. By providing a comprehensive account of the injury or illness, the NWCC 1 form ensures that accurate records are maintained, facilitating easier processing of workers' compensation claims and ultimately supporting those affected in their recovery and return to work.
Nwcc 1 Example
Nebraska Workers’ Compensation Court
First Report of Alleged Occupational Injury or Illness
NWCC Form 1 Revised 1 /20
Employer
Employer FEIN |
|
|
|
|
SIC Code |
|
|
|
Report Purpose |
|
|
|
OSHA Log Case # |
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Employer Name(s) |
|
|
|
|
|
|
|
|
|
|
Insured Name (If different from employer name) |
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Insured Address (If different) |
|
Location |
||||||||||||
City |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
State |
Zip Code |
Phone |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Insurance |
|
Carrier |
|
|
|
|
|
|
|
|
|
|
|
||||||
Carrier FEIN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Administrator FEIN |
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Claim Administrator (Name, address & phone number) |
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
City |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
State |
|
|
|
Zip Code |
|
|
Phone |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Claim Administrator Claim # |
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Self Insured |
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
Policy Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Check if |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Jurisdiction Claim # |
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Appropriate |
|
|
||||||||||||
Policy Period: |
|
From |
|
|
|
To |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
Insurance |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
Insured Report # |
|
|
|
|
|
|
|
|
Jurisdiction |
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Employee |
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name (Last, First, Middle)
Address
City
State |
Zip Code |
|
Phone |
|
|
||
|
|
|
|
|
|
|
|
Date of Birth |
|
Social Security Number |
Date Hired |
||||
|
|
|
|
|
|
|
|
Full Pay for DOI |
Yes |
|
|
No |
|
|
|
|
|
|
|
|
Number of Days |
Sex |
Male |
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
Salary Continued |
Yes |
|
|
No |
|
|
|
|
|
|
|
WorkedPerWeek |
|
|
|
Female |
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
Occupational Job Title |
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
Number of Dependents |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Marital Status |
|
Wage$ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
Occupational Code |
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Married |
|
|
|
|
|
|
|
|
|
Hourly |
|
|
|
|
|
|
NCCI Class Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Separated |
|
|
|
|
|
|
|
|
|
Daily |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
Unmarried |
|
|
|
|
|
|
|
Weekly |
|
|
|
Date Employee Began |
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
Unknown |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
Monthly |
|
|
|
|
Employment Status FT |
|
|
PT |
|
|
Other |
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Occurrence/Treatment
Date of Injury/Illness |
Time Employee Began Work |
|
|
Time of Occurrence |
AM |
|
|
Last Work Date |
||||||||||||||
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
AM |
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
PM |
|
|
|
|
(Cannot be determined |
|
|
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
PM |
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Where Did Injury/Illness Occur? |
|
|
|
|
|
|
|
|
|
Did Injury/Illness Occur On Employer’s Premises? |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
County |
|
State |
Zip |
Yes |
|
|
|
|
|
|
No |
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date Employer Notified |
Date Disability Began |
|
|
|
|
|
|
Date Returned to Work |
|
|
|
|
If Fatal, Give Date of Death |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Type of Injury/Illness (Briefly describe the nature of the injury or illness; e.g. lacerations to forearm)
Part of Body Affected (Indicate the part of the body affected by the injury/illness; e.g. right forearm, lowerback; and how it was affected)
How Injury/Illness Occurred (Describe activity and tools, materials, equipment the employee was using; how injury occurred)
Nature of Injury Code
Part of Body Code
Cause of
Injury Code
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Initial |
No medical |
treatment |
|
|
Emergency Room |
|
|
|
Name of physician or other health care provider: |
|
|
|
||
Treatment: First aid by |
No Medi |
cal |
Treatment |
Fir |
stFutureAid BymajorEmployer |
Minor Clinic/Hospital |
Emergency Care |
|
||||||
|
|
|||||||||||||
employer |
|
|
Hospitalized overnight |
|
medical/lost |
|
|
|
|
|||||
|
|
|
|
|
|
Hospitalized M |
ore Than 24 Hours |
Future Major Medical/Lost Time |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Minor clinic/hospital |
|
|
Hospitalized > 24 hours |
|
time |
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date Administrator Notified |
Form Preparer’s Name, Title and Phone |
|
|
Date Prepared |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
GENERAL INSTRUCTIONS
Underlined items are mandatory fields. A first report of injury or illness submitted without this information will be returned unfiled.
Employer:
•Employer FEIN — the employer/insured’s Federal Employer’s Identification Number.
•SIC Code — Standard Identification Classification code which represents the nature of the employer’s business.
•Report Purpose — defines the specific purpose of the transaction (examples: original = 00; cancel = 01; change = 02; denial = 04; correction = CO).
•OSHA Log Case # — the Log Case number required for reporting to OSHA.
•Employer Name — include all business names/doing business as (dba).
•Address (including city,state, and zip code) — the address of the employer’s actual location where the employee was employed at the time of the injury.
•Phone — phone number at the employer’s facility.
•Insured Name (if different from employer) — the named insured on the policy or the financially responsible
•Insured Address (if different from employer) — mailing address of the insured.
•Location — a code defined by the insured/employer which is used to identify the employer’s location.
Insurance Carrier:
•Carrier FEIN — carrier’s Federal Employer’s Identification Number.
•Administrator FEIN — administrator’s Federal Employer’s Identification Number.
•Name — the workers’ compensation insurer, approved self insured, or intergovernmental risk management pool.
•Address — address, city, state and zip code of insurer.
•Phone — phone number of insurer.
•Claim Administrator (name, address, & phone) — enter the name, address and phone number of the carrier, third party administrator, risk management pool, or self- insurer responsible for administering the claims, if different from carrier information.
•Policy # — the number assigned to the contract/policy for that employer.
•Policy Period — the effective and expiration dates of the contract/policy.
•Insurance Carrier/Self Insured Code # — for insurance carriers, the number assigned by the Nat’l Assn. of Insurance Commissioners. For
•Self Insured — check if appropriate.
•Claim Administrator Claim # — identifies a specific claim within a claim administrator’s claims processing system.
•Jurisdiction Claim # — number assigned by the court when the initial First Report is accepted.
•Insured Report # — a number used by the insured to identify a specific claim.
•Jurisdiction — the governing body or territory whose statutes apply (NE).
Employee:
•Name — give full name as shown on payroll (avoid initials if possible).
•Address — address, city, state and zip code of employee.
•Social Security Number. The social security number must be provided. This is mandatory pursuant to Neb.Rev.Stat.
•Date of Birth — the date the injured worker was born.
•Date Hired — the date the injured worker began his/her employment with the employer.
•Full Pay for DOI (date of injury) — check one.
•Salary Continued — check one.
•Number of Days Worked Per Week — the number of the employee’s regularly scheduled work days per week.
•Sex — check one.
•Number of Dependents — the number of dependents as defined by the Nebraska Workers’ Compensation Act.
•Marital Status — check one.
•Wage — check one and state wage.
•Occupational Job Title — the primary occupation of the claimant at the time of the accident.
•Occupational Code — Standard Occupational Classification code used to identify the primary occupation of the employee at the time of the accident.
•NCCI Code — The identifying number for an occupational classification.
•Date Employee Began
•Employment Status — check one.
Occurrence/Treatment:
•Date of Injury/Illness — date on which the accident occurred (only one date of injury per form).
•Time Employee Began Work — time employee began work for that date.
•Time of Occurrence — time of day the injury occurred.
•Last Work Date — the last paid work day prior to the initial date of disability.
•Where Did Injury/Illness Occur — complete county, state, and zip code.
•Did Injury/Illness Occur On Employer’s Premises — check one.
•Date Employer Notified — the date that the injury was reported to a representative of the employer.
•Date Disability Began — if not disabled answer none and skip questions.
•Date Returned to Work — if injured has returned to work, complete this question.
•If Fatal, Give Date of Death, (date employee died as a result of the
•Type of Injury/Illness — describe the nature of injury.
•Nature of Injury Code — the code which corresponds to the nature of the injury sustained by the employee.
•Part of Body Affected — the part of the body to which the employee sustained injury.
•Part of Body Code — the code which corresponds to the Part of the body to which the employee sustained injury.
•How Injury/Illness Occurred — a
•Cause of Injury Code — the code that corresponds to the cause of injury.
•Initial Treatment — check one.
•Name of physician or other health care provider — provide name of physician or other health care provider that treated employee for injury.
•Date Administrator Notified — the date the claim administrator who is processing the claim received notice of the loss or occurrence.
•Form Preparer’s Name, Title and Phone.
Form Characteristics
| Fact Name | Description |
|---|---|
| Form Purpose | This form reports alleged occupational injuries or illnesses in Nebraska. |
| Mandatory Fields | Certain fields are required. If not filled out correctly, the form may be returned unfiled. |
| Employer Information | Information about the employer includes FEIN, SIC code, and addresses. |
| Employee Details | Name, address, social security number, and employment status must be included for employees. |
| Date Requirements | Key dates are needed: the date of injury, notification, and return to work. |
| Insurance Carrier | The form requires details about the insurance carrier or self-insured entity. |
| Governing Law | This form is governed by the Nebraska Workers’ Compensation Act. |
Guidelines on Utilizing Nwcc 1
Filling out the NWCC 1 form is an essential step in reporting a work-related injury or illness. This form must be completed accurately to ensure a smooth process for all parties involved. The information provided here will be used to assess the situation and identify any potential benefits or claims.
- Employer Information: Enter the employer's Federal Employer Identification Number (FEIN) and Standard Industrial Classification (SIC) code. Specify the report purpose (e.g., original) and provide the OSHA log case number.
- Fill in the Employer Name and any other names or "doing business as" (DBA) names. Provide the complete address, including city, state, and zip code, along with a contact phone number.
- If applicable, enter the Insured Name and Insured Address. Include details about the insurance carrier and the claim administrator, along with their FEIN numbers and contact information.
- Policy Information: Include the policy number, effective dates, and insurance carrier/self-insured code number. Check the box if self-insured and provide the corresponding claim numbers.
- Employee Information: Record the employee's full name, address, date of birth, and Social Security number. Include the date hired, job title, and employment status (full-time/part-time).
- Provide details about the employee's work, including salary, number of dependents, marital status, and wage.
- Occurrence/Treatment: Describe the date and time of injury or illness. Specify the location and whether it occurred on the employer's premises. Include dates for employer notification, disability began, and return to work.
- Briefly describe the injury or illness and indicate the affected part of the body. Outline how the injury occurred, including the activity and equipment involved.
- Treatment Details: Indicate whether treatment was provided, and if so, include the name of the physician or health care provider involved.
- Complete the section for Form Preparer's name, title, and phone number, and date prepared.
Once the form is thoroughly filled out, it should be submitted according to the established protocols set by your organization or state regulations. Ensure all mandatory fields are completed accurately to prevent any delays in processing the report.
What You Should Know About This Form
What is the NWCC 1 form and why is it necessary?
The NWCC 1 form, or Nebraska Workers’ Compensation Court First Report of Alleged Occupational Injury or Illness, serves as a formal notification of an employee’s work-related injury or illness. It is essential for ensuring that the claim is officially recorded and processed under Nebraska's workers' compensation regulations. Completion of this form enables the employer and insurance providers to initiate appropriate benefits and support for the affected employee.
Who is responsible for completing the NWCC 1 form?
What information is required on the NWCC 1 form?
Several critical details must be included on the NWCC 1 form. This includes information about the employer, the insurance carrier, and the employee involved. Specific fields require the employee’s name, date of birth, date of injury, nature of the injury, and how it occurred. General instructions emphasize that some fields are mandatory; failure to complete these can result in the form being returned unfiled.
Is the employee's Social Security Number required on the NWCC 1 form?
Yes, the employee's Social Security Number is mandatory. It helps the Nebraska Workers' Compensation Court verify the employee's identity, especially when multiple individuals have similar names or birthdates. This unique identifier is crucial for accurately processing claims and ensuring the correct employee receives benefits.
What happens if the NWCC 1 form is not submitted in time?
If the NWCC 1 form is not submitted within the specified timelines, it may hinder the processing of the workers’ compensation claim. This could lead to delays in medical benefits and wage loss compensation for the injured employee. Timeliness is essential to ensure that the rights of the employee are protected and that they receive the necessary support promptly.
Are there penalties for incorrect information on the NWCC 1 form?
Providing inaccurate or false information on the NWCC 1 form can lead to serious consequences. It may result in delays in claim processing, loss of benefits, or even legal implications for the employer. Accuracy is critical; therefore, employers are encouraged to review the form thoroughly before submission.
Who can I contact if I have questions about the NWCC 1 form?
For inquiries about the NWCC 1 form, employers can contact the Nebraska Workers’ Compensation Court directly or reach out to their workers’ compensation insurance carrier. They can provide guidance and assistance in filling out the form correctly and ensure compliance with relevant laws and regulations.
Common mistakes
Filling out the NWCC 1 form, which serves as the First Report of Alleged Occupational Injury or Illness in Nebraska, is an important task that requires careful attention to detail. One common mistake is omitting required fields. Sections that are underlined on the form indicate mandatory information. Without this data, the report will be considered incomplete and returned unfiled, potentially delaying benefit claims.
Another frequent error is using incorrect or outdated employer information. The employer’s Federal Employer Identification Number (FEIN) and Standard Industrial Classification (SIC) code must be accurate. Errors in this area can lead to confusion and might complicate the processing of the report.
Many individuals also fail to thoroughly describe the nature of the injury or illness. Vague descriptions can lead to misunderstandings or conflicts regarding the type of injury, making it crucial to provide comprehensive information about what occurred. Similarly, indicating the exact location where the injury took place is vital. The form should capture the complete county, state, and zip code to avoid any ambiguity.
Some people neglect to correctly fill in the employee's information. Providing the full name, date of birth, and Social Security number is essential for identity verification. Incomplete or incorrect employee details can hinder the claim process.
A mistake often encountered is the failure to provide proper dates. The form requires several crucial dates, such as the date of injury, the date the employer was notified, and the date the disability began, if applicable. Inaccurate dates can impact the legitimacy of the claim.
Moreover, misunderstandings about the treatment options can lead to errors. Individuals sometimes check incorrect boxes regarding the type of treatment received (e.g., emergency room versus first aid). This detail is essential for the claim's verification process and can affect the benefits awarded.
Lastly, an often overlooked aspect is the importance of the juristic designation. Selecting the correct Jurisdiction Claim number and ensuring the Insurance Carrier's information aligns with the policy details is crucial to ensuring proper claim processing. This mistake can lead to unnecessary complications in the administration of the claim.
Documents used along the form
The NWCC 1 form is an essential document used in reporting occupational injuries or illnesses in Nebraska. It serves as the first report to the Workers’ Compensation Court about an incident that affects an employee’s ability to work. However, there are several other forms and documents that often accompany it. Understanding these documents can help streamline the process of filing a workers' compensation claim and can provide clearer guidance throughout the recovery and claims process.
- NWCC Form 2: This form is used to report the continuation of wage loss benefits. It includes details about the employee's wages during the recovery period, providing necessary information for compensation calculations.
- NWCC Form 3: A medical authorization form, allowing healthcare providers to disclose an injured employee’s medical records to the employer or the insurance carrier. This is crucial for the claims process as it verifies the extent of the injury and any ongoing treatment needs.
- NWCC Form 4: The form is utilized to notify the court of any changes in the status of a workers’ compensation claim. This may include alterations in the employee's work capacity or changes in medical treatment. Regular updates help maintain accurate records for the court.
- NWCC Form 10: This document is a wage-loss report that helps track and report the employee's lost wages resulting from an injury. Detailed wage history ensures the employee is compensated fairly for their time away from work.
- Employer’s Written Report: Employers may provide a detailed account of the incident, including the circumstances surrounding the injury and any relevant safety protocols in place. This report can serve as a supplementary account to the NWCC 1 form.
- Medical Records: These documents from healthcare providers detail the injury or illness, treatment rendered, and the expected recovery timeline. They are critical for demonstrating the nature and extent of the injury during the claims process.
- Occupational Health Records: If applicable, these records provide information on the employee's work environment and any potential hazards associated with their job, helping to establish a connection between the work environment and the injury sustained.
- Witness Statements: Statements from coworkers or others who witnessed the incident can add important context to the claim. Their perspectives may help clarify how the injury occurred and support the employee’s account of events.
Each of these documents plays a role in developing a comprehensive view of the case, ensuring that the claims process moves forward efficiently. Familiarity with these forms can empower employees to navigate the workers' compensation system with confidence, helping them understand their rights and responsibilities in the event of an injury or illness related to their occupation.
Similar forms
The NWCC 1 form has several similar documents used for reporting and documenting workplace injuries or illnesses. Each one serves a specific purpose in the workers' compensation process.
- OSHA 300 Log: This document is used to record and summarize occupational injuries and illnesses. It is required for certain employers to track the number and types of work-related injuries over the year, similar to how the NWCC 1 form serves to report an individual injury.
- First Report of Injury (FROI) Form: This form serves the initial notification for a workers' compensation claim. Like the NWCC 1, it needs detailed information about the employee, the injury, and the circumstances.
- Employee's Claim for Compensation (Form 1): This document is submitted by an employee to request benefits related to a work injury. It shares similarities in collecting personal and employment details like the NWCC 1 form.
- State-Specific Workers' Compensation Claim Form: Each state has its own version of a claim form specific to that state's regulations. They collect similar information, such as employee details and injury descriptions, similar to the NWCC 1.
- Treatment Authorization Request (TAR): This document is used to obtain approval for medical treatment related to a work injury. It often requires similar information about the injury and the injured worker's details.
- Incident Report: Typically filled out by employers to document any work-related incidents. Like the NWCC 1 form, it includes details of the injury and circumstances surrounding it, although it may not be specifically for workers' compensation.
- Return to Work Form: This form is used when an employee is ready to return after an injury. It may require some of the same employee information as the NWCC 1 form and indicates the employee's status regarding the injury.
Dos and Don'ts
Things you should do:
- Provide accurate information for all mandatory fields, including the employer's FEIN and employee's Social Security Number.
- Double-check the spelling of names and addresses to avoid discrepancies.
- Submit the form promptly to avoid delays in processing the claim.
- Ensure a complete description of the injury or illness is included, noting the time and place it occurred.
- Include the date the employer was notified of the injury.
- Mark the appropriate checkboxes for full pay and salary continuation.
- List all dependents accurately, as this can affect claim processing.
- Keep a copy of the completed form for your records.
Things you shouldn't do:
- Do not leave mandatory fields blank; this will result in the form being returned.
- Avoid using initials for names; full names are required to minimize confusion.
- Do not submit a form without verifying the accuracy of dates and codes.
- Never provide personal information that is not required, as it may lead to privacy concerns.
- Do not forget to document any relevant details regarding the treatment received.
- Do not wait too long to submit the form after the injury; timely reporting is crucial.
- Do not assume information is known; always write it down clearly.
- Never submit incomplete information, as it can delay the processing of the claim.
Misconceptions
-
Misconception 1: The NWCC Form 1 is optional for employers.
In reality, this form is mandatory in Nebraska when reporting workplace injuries or illnesses. Employers must complete and submit it to ensure compliance with state regulations.
-
Misconception 2: Only injuries that require hospitalization need to be reported on the NWCC Form 1.
This is not true. The form should be filled out for all alleged occupational injuries or illnesses, regardless of the severity. Even minor incidents must be documented to safeguard both the employee's rights and the employer’s responsibilities.
-
Misconception 3: Filling out the NWCC Form 1 is a straightforward process that doesn’t require special attention.
While it may seem simple, accurate completion of the form is crucial. Missing information or errors can lead to delays in processing claims. Careful attention ensures that all required fields are properly filled.
-
Misconception 4: The NWCC Form 1 can be submitted at any time after an injury occurs.
There are specific timelines for reporting on this form. Employers should be aware that delays in submitting the report can impact their liability and the injured employee’s ability to receive timely benefits.
-
Misconception 5: The personal information provided on the NWCC Form 1 is not shared with anyone outside the company.
This is misleading. While the information is primarily for workers’ compensation purposes, it may need to be shared with insurance carriers or other entities involved in the claims process. Safeguarding this data is essential, but it's important to understand that it might be reviewed by other parties.
Key takeaways
The NWCC 1 Form is vital for reporting work-related injuries or illnesses in Nebraska. Understanding the key elements can ensure accurate completion and effective communication.
- Mandatory Fields: Certain fields on the form must be filled out for it to be processed. Missing mandatory information can result in delays, so attention to detail is essential.
- Timeliness: Reporting the injury or illness promptly is crucial. The date the employer is notified should align closely with the occurrence date of the event to facilitate timely claims processing.
- Employee Information: Providing comprehensive details about the employee, such as full name, social security number, and job title, helps in accurately identifying the individual and their specific claim.
- Type and Cause of Injury: Clearly describing the nature and cause of the injury on the form enhances the ability to process the claim effectively. Include any tools or equipment involved to provide thorough context.
Browse Other Templates
What Is the Maximum Income to Qualify for Masshealth - Ensure all names and social security numbers are correctly listed for accurate processing.
Closed Book Test - The Open Book examination includes questions that reflect real-world VE scenarios and protocols.