Fill Out Your Oca 960 Form
The OCA 960 form plays a vital role in the process of sharing health information while adhering to strict privacy guidelines. Designed under the New York State Department of Health's approval, it allows patients or their representatives to authorize the release of their medical records. Completion of this form ensures that any sensitive information, particularly regarding alcohol and drug abuse, mental health treatment, and HIV-related data, is only disclosed with express permission. The form also outlines the recipient's obligations regarding the confidentiality of the information being shared, including restrictions on redisclosure, thereby protecting patients' rights. Notably, signing the OCA 960 form is voluntary, meaning a patient's healthcare services or insurance coverage cannot be denied if they choose not to authorize the release. The document requires clear identification of both the healthcare provider releasing the information and the individual or entity receiving it. Moreover, patients maintain the right to revoke their consent at any time, although this revocation cannot affect actions already taken based on the authorization. The careful balance of facilitating necessary communications and safeguarding privacy is foundational to the OCA 960 form.
Oca 960 Example
@ |
|
|
OCA Official Form No.: 960 |
|
|
|
|
|
|
|
|
AUTHORIZATION |
FOR RELEASE OF HEALTH INFORMATION |
PURSUANT TO HIPAA |
|
|
[This form has been approved by the New York State Department of Health] |
||
Patient |
Name |
Date of Birth |
Social Security Number |
|
Patient |
Address |
|
|
|
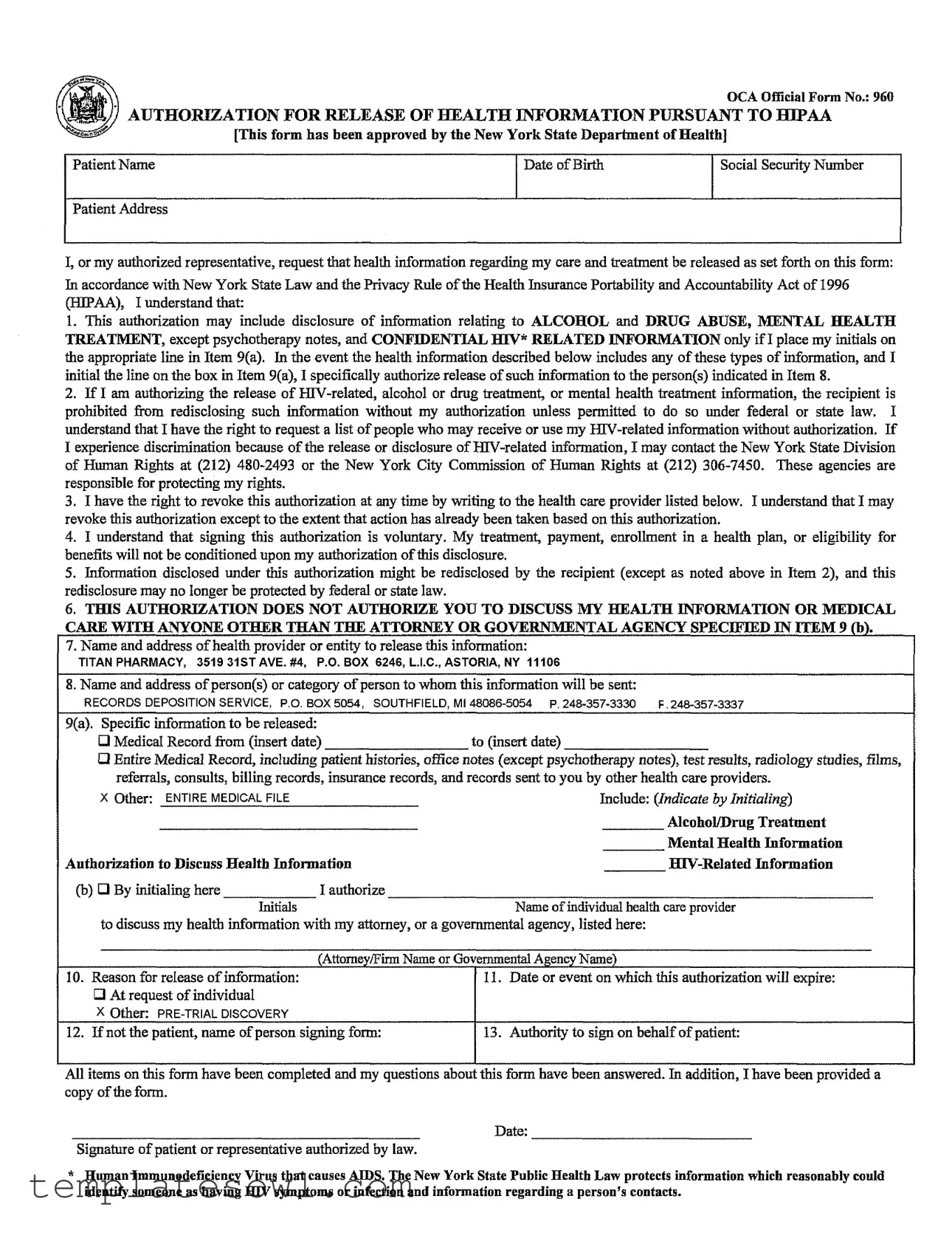
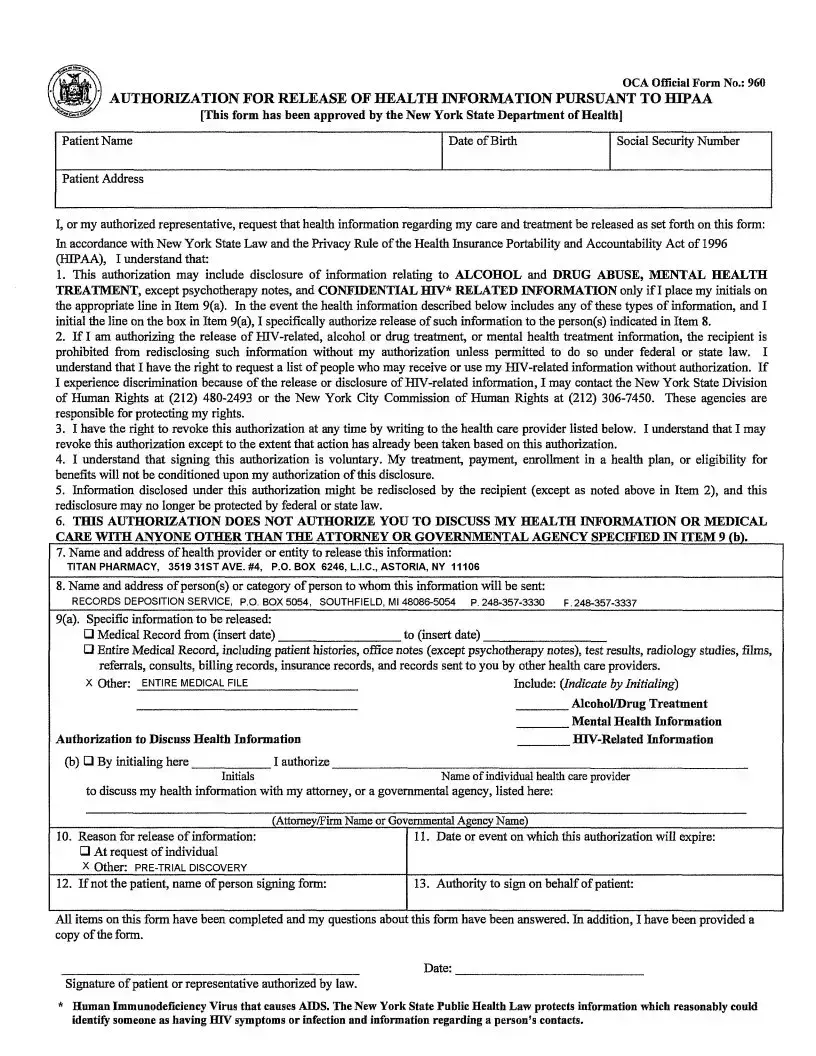
I, or my authorized representative, request that health information regarding my care and treatment be released as set forth on this form:
In accordance with New York State Law and the Privacy Rule of the Health Insurance Portability and Accountability Act of 1996
1. This authorization may include disclosure of information relating to ALCOHOL and DRUG ABUSE, MENTAL HEALTH
TREA_NT, except psychotherapy notes, and CONFIDENTIAL H1V* RELATED INFORMATION only ifI place my initials on the appropriate line in Item 9(a). In the event the health information described below includes any of these types of information, and I initial the line on the box in Item 9(a), I specifically authorize release of such information to the person(s) indicated in Item 8.
2.If I am authorizing the release of
3.I have the right to revoke this authorization at any time by writing to the health care provider listed below. I understand that I may revoke this authorization except to the extent that action has already been taken based on this authorization.
4.I understand that signing this authorization is voluntary. My treatment, payment, enrollment in a health plan, or eligibility for benefits will not be conditioned upon my authorization of this disclosure.
5.Information disclosed under this authorization might be rediselosed by the recipient (except as noted above in Item 2), and this
redisclosure may no longer be protected by federal or state law.
6.THIS AUTHORIZATION DOES NOT AUTHORIZE YOU TO DISCUSS MY HEALTH INFORMATION OR MEDICAL
CARE WITH ANYONE OTHER THAN THE ATTORNEY OR GOVERNMENTAL AGENCY SPECIFIED IN ITEM 9 (b).
7. Name and address of health provider or entity to release this information:
TITAN PHARMACY, 3519 31STAVE. #4, P.O. BOX 6246, K.L.C., ASTORIA, NY 11106
8. Name and address of person(s) or category of person to whom this information will be sent:
RECORDS DEPOSITION |
SERVICE, P.O. BOX 5054, SOUTHFIELD, |
MI |
P. |
|
9(a). Specific information to be released: |
|
|
|
|
[] Medical Record |
from (insert date) |
to (insert |
date) |
|
[] Entire Medical Record, including patient histories, office notes (except psychotherapy notes), test results, radiology studies, films, referrals, consults, billing records, insurance records, and records sent to you by other health care providers.
X Other: |
ENTIREMEDICALFILE |
Include: (Indicate by Initialing) |
||
|
|
|
Alcohol/Drug |
Treatment |
|
|
|
Mental Health |
Information |
Authorization |
to Discuss Health |
Information |
||
Co) [] By initialing here |
I authorize |
|
|
|
|
Initials |
Name of individual health care provider |
|
|
to discuss my health information with my attorney, or a governmental agency, listed here: |
|
|||
(Attome_f/FirmName or
I0. Reason for release of information: [] At request of individual
X Other:
12. If not the patient, name of person signing form:
GovernmentalAgency Name)
[ 11. Date or event on which this authorization will expire:
!13. Authority to sign on behalf of patient:
All items on this form have been completed and my questions about this form have been answered. In addition, I have been provided a copy of the form.
Date:
Signature of patient or representative authorized by law.
*Ituman Immunodeficiency Virus that causes AIDS. The New York State Public Health Law protects information which reasonably could identify someone as having HIV symptoms or infection and information regarding a person's contacts.
Form Characteristics
| Fact Name | Description |
|---|---|
| Form Title | Authorization for Release of Health Information Pursuant to HIPAA. |
| Governing Law | This form is governed by New York State Law and the Privacy Rule of the Health Insurance Portability and Accountability Act of 1996 (HIPAA). |
| Patient Information | The form requires the patient's name, date of birth, and social security number for verification. |
| Types of Information | Disclosure may include sensitive information about alcohol and drug abuse, mental health treatment, and HIV-related information. |
| Voluntary Authorization | Signing this form is voluntary; patient's treatment or eligibility for benefits is unaffected by this decision. |
| Revocation Rights | Patients can revoke authorization at any time unless actions have already been taken based on the authorization. |
| Redisclosure | Released information might be redisclosed by the recipient and may not be protected thereafter under federal or state law. |
| Health Provider | The form specifies the health provider or entity responsible for releasing the information, such as Titan Pharmacy. |
| Recipient's Information | Information will be sent to specified persons or organizations, such as Records Deposition Service. |
| Expiration | The authorization includes a section for specifying when it will expire, ensuring clarity on the duration of the consent. |
Guidelines on Utilizing Oca 960
Once you obtain the OCA 960 form, filling it out involves providing specific personal and health information. Make sure to review your completed form before submission to ensure all necessary details are included.
- Enter the patient's full name in the designated space.
- Provide the patient's date of birth.
- Fill in the patient's social security number.
- Input the patient's complete address.
- Review the sections regarding authorization and initial any applicable options in Item 9(a) to include sensitive information, if desired.
- In Item 7, write the name and address of the health provider releasing the information, for instance, Titan Pharmacy, along with their address.
- In Item 8, list the name and address of the person or entity receiving the information, such as Records Deposition Service.
- Select what specific information is to be released in Item 9, marking the appropriate boxes.
- If applicable, initial any boxes for Alcohol/Drug Treatment, Mental Health Information, or HIV-Related Information.
- State the reason for release in Item 10, such as "Pre-Trial Discovery."
- If the form is not signed by the patient, provide the name of the representative signing in Item 12.
- Indicate the expiration date or event of the authorization in Item 11.
- Sign and date the form at the bottom, ensuring the individual authorized to sign is indicated.
What You Should Know About This Form
What is the OCA 960 form used for?
The OCA 960 form, also known as the Authorization for Release of Health Information Pursuant to HIPAA, is used to give healthcare providers permission to share your medical records with specific individuals or entities. This form ensures that your health information is communicated securely and in compliance with New York State Law and federal regulations under the Health Insurance Portability and Accountability Act (HIPAA). It is commonly required in legal situations, such as pre-trial discovery, where access to health information may be essential.
What type of health information can be released using the OCA 960 form?
This form allows for the release of a variety of health information. It can include your entire medical records, which comprise patient histories, office notes (excluding psychotherapy notes), test results, insurance records, and more. Additionally, you can specifically request information regarding alcohol and drug treatment, mental health information, or HIV-related information. However, you must initial the respective lines on the form to authorize the release of these sensitive types of information.
Can I revoke my authorization after signing the OCA 960 form?
Yes, you have the right to revoke your authorization at any time. To do this, you simply need to notify your healthcare provider in writing. Keep in mind that your revocation will not affect any actions that have already been taken based on your original authorization. It's important to communicate this clearly and promptly to ensure the protection of your health information.
Are there any risks associated with the release of my health information through the OCA 960 form?
When you authorize the release of your health information, it可能 be shared with someone else. While the recipient is generally expected to keep your information confidential, this redisclosure may not always be protected under federal or state law. Thus, it’s important to be cautious about whom you allow access to your health information, especially if it contains sensitive details related to mental health, alcohol or drug treatment, or HIV status.
Do I have to provide my authorization to have my healthcare needs met?
No, signing the OCA 960 form is entirely voluntary. You should know that your treatment, payment, enrollment in a health plan, or eligibility for benefits will not depend on whether you choose to authorize the disclosure of your health information. You have the right to make decisions that prioritize your privacy and comfort with sharing your medical records.
Common mistakes
Filling out the OCA 960 form accurately is crucial for the proper release of health information. However, many individuals make several common mistakes that can lead to delays or issues in processing. Here are five notable errors to avoid.
One major mistake involves failing to provide complete patient information. Missing details such as the date of birth or social security number can prevent the healthcare provider from identifying the correct records. Ensure that all blank fields are filled in completely to avoid unnecessary complications.
Another frequent error is neglecting to specify which information should be released. If you don’t check off the specific types of information desired in Item 9(a), it may lead to the release of more information than intended, potentially violating privacy concerns.
Confusion around initials can be problematic. Some people don’t realize that initialing in Item 9(a) is necessary for authorizing the release of sensitive information, such as HIV-related or mental health records. Without these initials, the requested information may not be disclosed, impacting your case.
Moreover, individuals often overlook the importance of revocability. Not understanding that they can revoke authorization at any time can lead to anxiety and issues later. It’s essential to know that this right is in place and to communicate any changes promptly.
Lastly, forgetting to sign the form can invalidate it entirely. This seems simple, yet many submit incomplete forms. Remember that your signature is an essential part of the authorization process, confirming that you understand and agree to the release of health information.
Documents used along the form
The OCA 960 form is an essential document for authorizing the release of health information in compliance with HIPAA standards and New York State law. When completing this form, you might also need several other documents that can support the authorization process. Below are five commonly utilized forms and documents that may accompany the OCA 960 form.
- Patient Consent Form: This document confirms the patient's consent for their health information to be shared. It often contains details about the specific information to be disclosed and the parties involved in the release.
- Release of Information Form (ROI): Similar to the OCA 960, this form allows healthcare providers to disclose patient records to specific entities or individuals. It clarifies what information can be shared and with whom.
- Verification of Identity Form: To protect patient privacy, this form helps establish the identity of the person requesting the health information. It may require the requester to provide identification details to prevent unauthorized access.
- Authorization for Use and Disclosure of Medical Records: This comprehensive form allows healthcare providers to disclose records for various situations, including legal proceedings. It often includes more broad terms than the OCA 960 form.
- Notice of Privacy Practices: This document informs patients of their rights under HIPAA and how their health information may be used and disclosed. It may accompany other forms to ensure patients are aware of their privacy rights.
Incorporating these documents along with the OCA 960 form facilitates a smoother process for the release of health information, ensuring compliance with legal requirements. It's important to understand the purpose of each document to effectively navigate this complex area.
Similar forms
The OCA 960 form is designed to authorize the release of health information under specific conditions. Here are eight other documents that serve similar purposes, along with how they compare to the OCA 960 form:
- HIPAA Authorization Form: Like the OCA 960, this form is used to authorize health care providers to disclose health information. It also emphasizes patient rights regarding consent and revocation.
- Consent for Treatment Form: This document allows patients to agree to receive specific medical treatments. Similar to the OCA 960, it ensures that patients are informed before any actions are taken regarding their care.
- Medical Records Release Form: This form permits the transfer of medical records from one provider to another. It parallels the OCA 960 by specifying the information to be shared and requiring patient consent.
- Power of Attorney for Healthcare: This document designates an individual to make health care decisions on behalf of another. Like the OCA 960, it involves clear authorization for sharing health-related information.
- Financial Disclosure Form: Used in healthcare financing, this form can require disclosure of financial records. It resembles the OCA 960's focus on consent for sharing sensitive information.
- Release of Information for Insurance Purposes: This form is often required by insurance companies to access medical records for claims. Its function is similar to the OCA 960 in that it facilitates the release of health data with the patient’s consent.
- Substance Abuse Treatment Disclosure Consent: This document specifies the release of records related to substance abuse treatment. It shares similarities with the OCA 960 in outlining specific protections around sensitive information.
- Mental Health Treatment Release Request: This form is used to disclose mental health treatment records. Like the OCA 960, it includes particular provisions for protecting sensitive health information.
Dos and Don'ts
When filling out the OCA 960 form, there are several important dos and don'ts to keep in mind. Following these guidelines can help ensure that your health information is handled properly.
- Do read the entire form carefully before filling it out.
- Do include your full name, date of birth, and social security number accurately.
- Do initial the appropriate lines if you are disclosing sensitive information (like mental health or HIV-related information).
- Do specify exactly what information you want to be released.
- Don’t leave any unnecessary blank spaces, as this can lead to misunderstandings.
- Don’t forget to provide the contact information for both the health provider and the recipient of the information.
- Don’t sign the form if you have not received answers to all your questions.
- Don’t assume your authorization does not need to include a specific expiration date—make sure to fill that out.
Misconceptions
Misunderstandings about the OCA 960 form can lead to confusion when it comes to managing health information. Here are some common misconceptions debunked:
- The OCA 960 form is only for HIV-related information. This form is actually used to authorize the release of various types of health information, not just HIV-related. It covers alcohol and drug treatment, mental health information, and more.
- You must disclose everything if you sign the form. Signing the OCA 960 does not mean you are forced to share your entire medical history. You can specify the information you want to release by checking or initialing the appropriate boxes.
- You can't revoke the authorization once it's signed. That’s not true. Patients can revoke this authorization at any time, as long as they provide written notice to the healthcare provider listed.
- Your treatment depends on signing this authorization. Signing the authorization is completely voluntary. A healthcare provider cannot condition your treatment or payment upon whether you authorize the release of your information.
- All information disclosed remains confidential. While confidentiality is important, once the information is shared, the recipient may redisclose it, and such redisclosure might not be protected by the same laws.
- You can discuss your health information with anyone if you authorize it. Not exactly. The form only allows discussions with the specific attorney or governmental agency named in the document.
- You must include your Social Security Number on the form. Providing your Social Security Number is not a requirement. It’s good practice to only share this information when absolutely necessary.
- If the form is signed, there are no limits on who receives the information. The form includes specific fields where you designate who is allowed to receive your information, keeping your privacy in check.
- This form is not relevant in cases of court-ordered treatment. In fact, the OCA 960 form may still apply even in legal situations, but it’s essential to understand the specific context and regulations surrounding such cases.
Key takeaways
The OCA 960 form, also known as the Authorization for Release of Health Information, is essential for managing the release of sensitive health information. Here are key takeaways regarding its use:
- Purpose of the Form: It permits patients or their authorized representatives to request their healthcare information to be shared with designated individuals or entities.
- Types of Information: The form allows for sensitive information disclosure, including mental health records and substance use treatment, if specifically authorized by the patient.
- Revocation Rights: Patients can revoke the authorization at any time by informing the healthcare provider, though this won’t affect actions already taken based on the authorization.
- Voluntary Authorization: Signing the form is voluntary. It should not impact your treatment or eligibility for benefits.
- Redisclosure Risks: Once disclosed, the information may be further shared by the recipient, potentially diminishing protections under law.
- Limitations: Authorization does not allow discussions of health information with anyone other than the specified attorney or governmental agency.
- Contact Information: The provider releasing the information must be clearly identified, including their name and address.
- Expiration Details: The authorization must indicate its expiration date or event, which clarifies how long the recipient can use the information.
Browse Other Templates
Land Contract Template Michigan - Parties can determine possession rights contingent on contract compliance.
Broward Animal Care and Adoption - Knowing the vaccination history can aid in future healthcare decisions.
Farbar Contract - Specific closing documents to be provided by both parties are listed, ensuring clarity and organization.