Fill Out Your Oha 7210 Form
The OHA 7210 form is an essential document for individuals seeking coverage under the Oregon Health Plan. As part of the application process, it collects vital information about applicants and their households to determine eligibility for health coverage. Applicants are required to provide details such as Social Security numbers, birth dates, income levels, and information regarding existing health insurance. The form must be filled out for everyone in the household, which can include spouses, children, and other dependents claimed on tax returns. There are specific instructions for individuals without a Social Security number and those who may qualify under various categories. Once the application is completed, it can be submitted either by mail or fax to the OHP Customer Service. For those needing assistance, resources are readily available, including trained agents and community partners to guide applicants through the process, ensuring that help is accessible in multiple languages. Understanding how to properly fill out the OHA 7210 is crucial for gaining access to necessary healthcare services in Oregon.
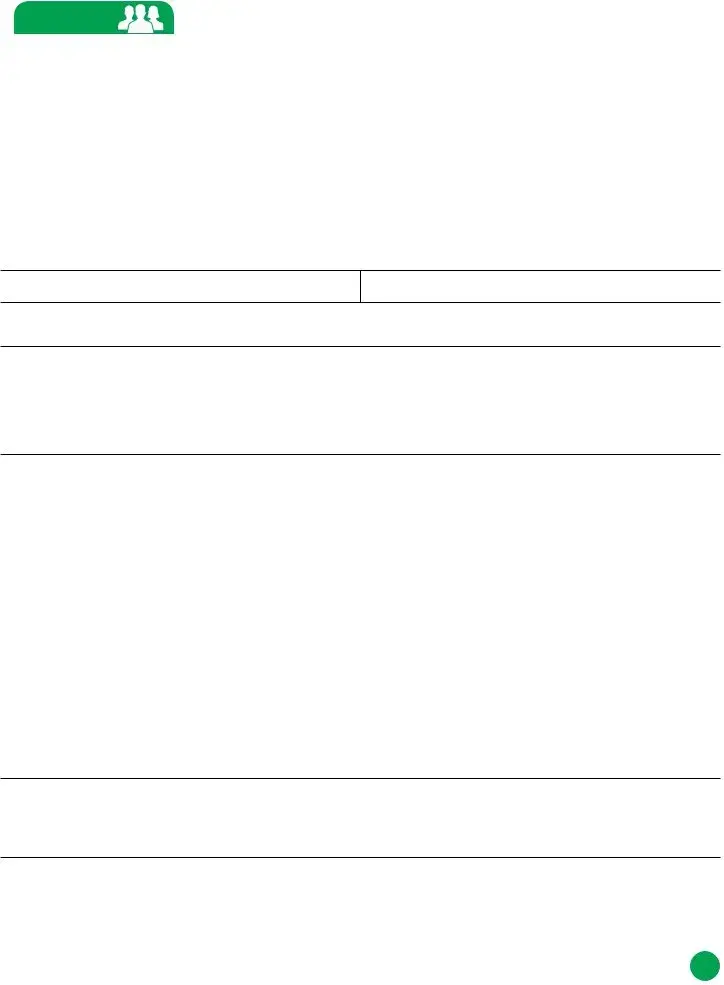
Oha 7210 Example

Application for Oregon
Health Plan Coverage
Need help with this |
Get expert help at no cost from a certified insurance agent, community |
||||||||
application? |
|
partner or customer service representative: |
|
|
|||||
|
|
|
• Visit www.OregonHealthCare.gov to find agents and community |
||||||
|
|
|
|
partners who can help you apply. |
|
|
|||
|
|
|
• Call OHP Customer Service at |
||||||
|
|
|
|
a list of agents and community partners in your area. You can ask for |
|||||
|
|
|
|
help in a different language, too. |
|
|
|||
|
|
|
|
|
|
|
|||
Information you will |
You will need the following information for everyone in your household: |
||||||||
need to provide on |
• Social Security number for everyone who has one and is applying |
||||||||
this application: |
|
||||||||
|
• Alien Resident number for everyone who has one and is applying (you |
||||||||
|
|
|
|||||||
|
|
|
|
may qualify even if you don’t have one) |
|
|
|||
|
|
|
• Birth dates |
|
|
|
|
||
|
|
|
• Income and deductions (for example, from pay stubs or |
||||||
|
|
|
• Information about health insurance available to you through an |
||||||
|
|
|
|
employer |
|
|
|
|
|
|
|
|
|
|
|
||||
AFTER COMPLETING YOUR APPLICATION MAIL OR FAX TO: |
|
||||||||
Mail: |
|
|
Fax: |
|
|
|
|
||
OHP Customer Service |
|
|
|
|
|
||||
P.O. Box 14015 |
|
|
|
|
|
|
|
|
|
Salem, OR |
|
|
|
|
|
|
|
||
Be sure to fill out all necessary pages and SIGN your application before sending. |
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OFFICIAL USE ONLY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date of request |
|
Received |
|
Program |
Branch |
|
Case no. |
Worker ID |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Case name |
|
|
|
Route to |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Prime no. |
|
|
SSN |
App status |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Office use |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OHA 7210 (Rev 09/16)
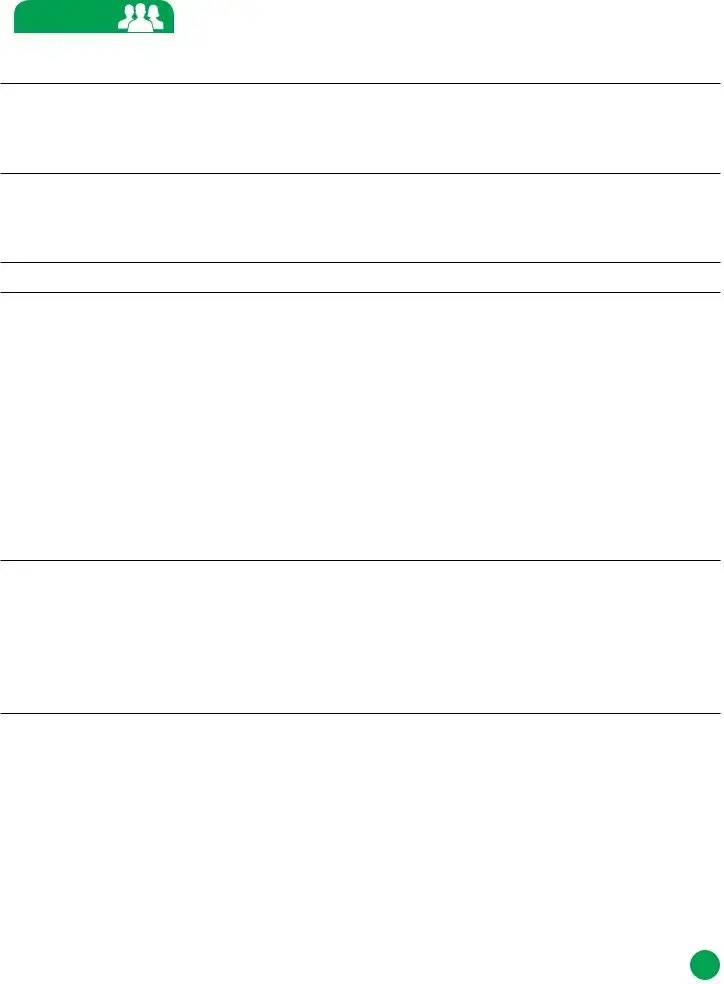
How do we use |
First we’ll ask some basic questions about each person. Then we’ll ask about |
your information? |
income, current health insurance, disabilities and Tribal ancestry. |
|
We’ll keep all the information you provide private, as required by law. |
|
See our privacy policy in the Application Guide for more information. |
|
|
Who to include on |
We need you to tell us about yourself and everyone else in your household. |
this application |
Your household includes the people below: |
|
• You. |
|
• Your legal spouse. |
|
• Your children. Include children of all ages who you claim as dependents on |
|
your taxes. |
|
• Your |
|
• Anyone else you include on your federal income tax return; even if they do |
|
not live with you. |
|
Important: Is someone living with you who is not on the list above? If they |
|
want health coverage, they must fill out a separate application. |
|
Please write clearly and provide as much information as possible about each |
|
person when filling out this application. |
|
If you are applying for more than four people, please make copies of |
|
pages |
|
|
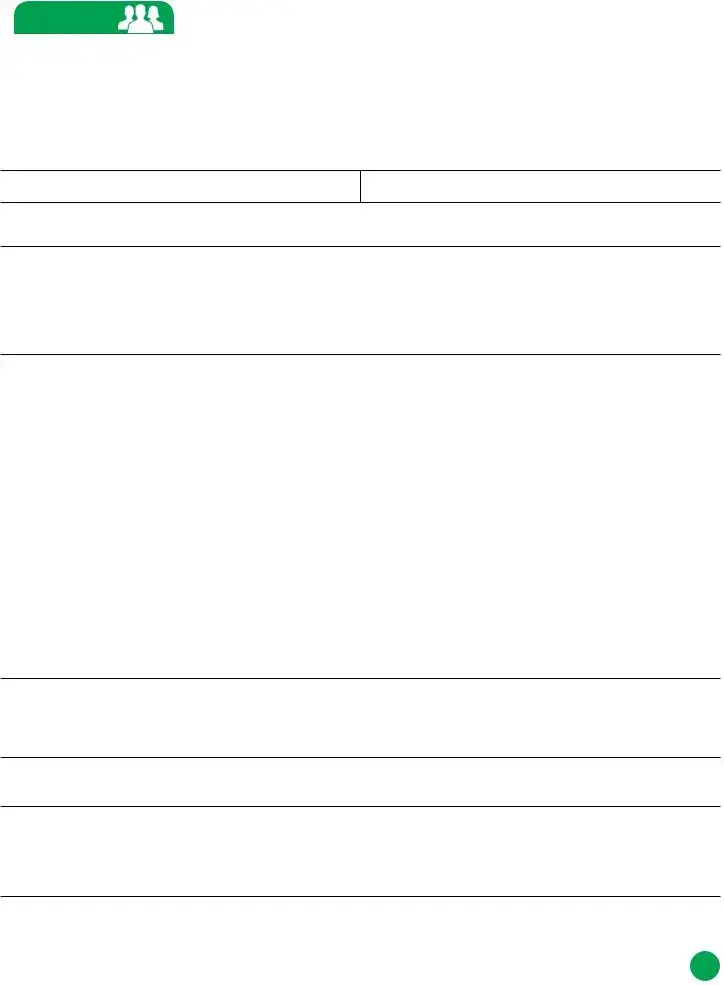
STEP 1 TELL US ABOUT YOURSELF You’ll be our primary contact
TELL US ABOUT YOURSELF You’ll be our primary contact
1. Legal name (first, middle, last and suffix) |
2. Maiden or other names used (first, middle, last) |
|
|
3.Social Security number (SSN) – An SSN is required for everyone who is applying for health coverage and who has one. An SSN is optional for others, but providing an SSN can speed up the application process.
SSN: |
|
No: £Applied for SSN □Newborn Don’t have SSN □Not eligible for SSN □Refuses to obtain SSN |
|||||||||
|
4. |
Birthdate (MM/DD/YYYY) |
5. Sex: |
6. Phone number £ Home |
£ Work £ Cell |
|
|||||
|
|
|
|
£ Male £ Female |
( |
) |
|
|
|
|
|
|
|
|
|
|
|
||||||
7. |
Do you live in Oregon? Answer yes, even if you are in Oregon to look for work or because of a job. |
||||||||||
|
|
Only answer if you are applying for health coverage for yourself. £ Yes £ No |
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
8. |
Email address |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
||
9. |
Home address (skip to #15 if you don’t have one) |
|
|
|
10. |
Apartment/Unit # |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
11. |
City |
|
12. County |
13. State |
|
14. |
ZIP code |
||||
|
|
|
|
|
|
|
|
|
|||
15. |
If you don’t have a home address, please tell us where you spend the majority of your time and then give |
||||||||||
|
|
|
us a mailing address (#16). County: ___________________________ State:______ ZIP code: ________ |
||||||||
|
|
|
|
|
|
|
|
||||
16. |
Mailing address (only required if different from home address) |
|
17. |
Apartment/Unit # |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
18. |
City |
|
|
|
19. State |
|
20. |
ZIP code |
|||
|
|
|
|
|
|
|
|
|
|
|
|
NEED HELP? Call us at |
2 |
|
OHA 7210 (Rev 09/16) |
||
|
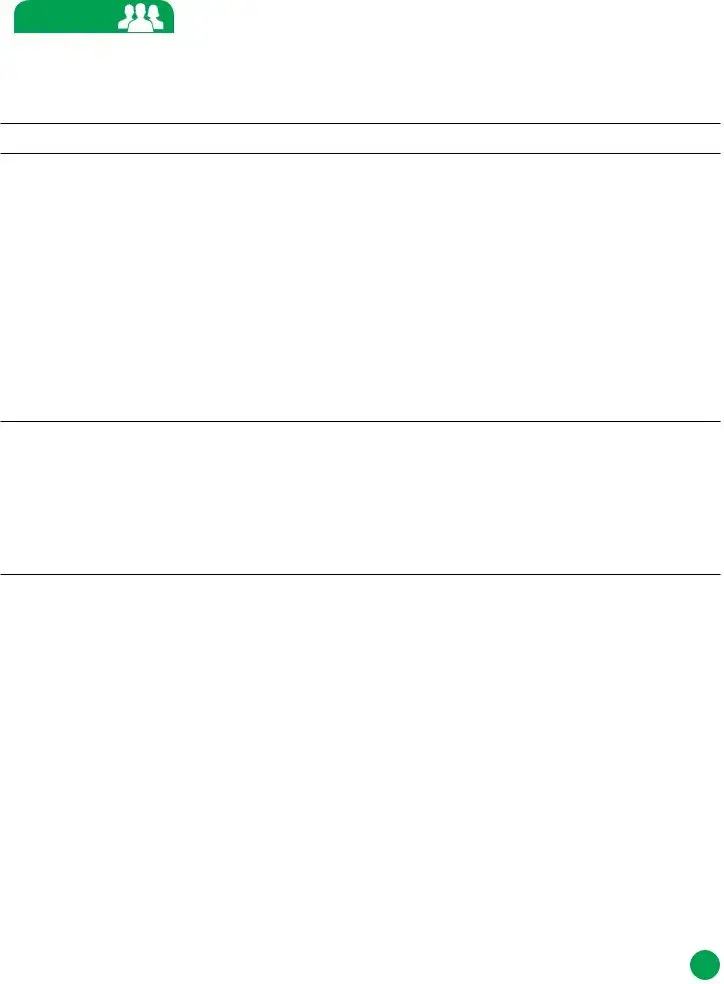
STEP 1 Primary Contact, continued
Primary Contact, continued
21.In what language do you want us to speak with you?
22.In what language do you want us to write to you?
23.Do you need written materials in an alternate format? £ Yes £ No
If yes, which? £ Braille £ Oral presentation £ Computer disk £ Audio tape £ Large print
24.Are you pregnant? £ Yes £ No
25.Is anyone else in your household pregnant? £ Yes £ No
26.Do you, the primary contact, plan to file a 2017 federal income tax return in 2018? Answer “yes” if you plan to file, even if you will not owe taxes or are getting a refund. You can apply for health coverage, even if you don’t plan to file taxes.
£ YES. If yes, complete
a.What will your filing status be on your 2017 tax return?
£ Single £ Head of household £ Qualifying Widow(er) Married filing: £ Jointly £ Separately
If married, spouse’s name?___________________________________________________________
b.Do you have any tax dependents? List all dependents regardless of their age or address. £ Yes £ No
First/last name and birthdate of each dependent: ________________________________________
________________________________________________________________________________
Note: for each person listed as a dependent, complete Step 2.
27.Are you claimed as a dependent on anyone else’s tax return? £ Yes £ No
If yes, list first/last name and birthdate of the tax filer:________________________________________
How are you related to the tax filer? ______________________________________________________
28.If Hispanic/Latino ethnicity — check all that apply
£Mexican £ Mexican American £ Chicano/a £ Puerto Rican £ Cuban £ Other £ Decline to answer
29.Race — check all that apply
£American Indian or Alaska Native £ Asian Indian £ Black or African American £ Chinese
£Filipino £ Guamanian or Chamorro £ Japanese £ Korean £ Native Hawaiian £ Other Asian
£Other Pacific Islander £ Samoan £ Vietnamese £ White £ Decline to answer
30.Is your 2016 tax filing information the same as listed for 2017?
£YES. £ NO. If no, complete Appendix D - 2016 Tax Filing Status
31.Are you applying for health coverage for yourself? You can apply even if you already have health coverage.
£ YES. If yes, go to #32. £ NO. If no, skip to page 5 for Step 2.
NEED HELP? Call us at |
3 |
|
OHA 7210 (Rev 09/16) |
||
|
STEP 1 Primary Contact, continued
Primary Contact, continued
32.Are you a U.S. citizen or national? £ YES. If yes, skip to #34. £ NO
33.If you are not a U.S. citizen or national, do you have an eligible immigration status?
We only use this information to determine eligibility. See the Application Guide for more information
about eligible immigration statuses.
£YES. If yes, complete
a.Immigration document type: ____________________________________
b.Document ID #: _______________________________________________
c.Status: ______________________________________________________
d.Date status gained: _________________
e.Have you lived in the U.S. since 1996? £ Yes £ No
f.Are you, your spouse or a parent a veteran or an
34.Are you the primary caretaker for any children under age 19 who: 1) live with you and 2) are related to you but are not your own children? For example, a grandparent who is the primary caretaker for a grandchild.
£ Yes £ No
If yes, list first/last name of child(ren). Do not include your adopted, biological or step children: ________
______________________________________________________________________________________
______________________________________________________________________________________
NEED HELP? Call us at |
4 |
|
OHA 7210 (Rev 09/16) |
||
|
|
STEP 2 |
ADDITIONAL HOUSEHOLD MEMBER – PERSON 2 |
Complete Step 2 for everyone in your household. See page 2 for more information about who to include on your application.
If you are listing more than four people in your household, please make copies of pages
|
1. |
Legal name (first, middle, last and suffix) |
2. Maiden or other names used (first, middle, last) |
|
|
|
|
|
|
3. |
Relationship to you |
|
|
|
|
|
|
|
|
4. |
Social Security number (SSN) – An SSN is required for everyone who is applying for health coverage and |
|||
|
|
who has one. An SSN is optional for others, but providing an SSN can speed up the application process. |
||
SSN: |
No: £Applied for SSN □Newborn Don’t have SSN □Not eligible for SSN □Refuses to obtain SSN |
|||
5.Birthdate (MM/DD/YYYY)
6. Sex: £ Male £ Female
7.Does Person 2 live in Oregon? Answer yes, even if you are in Oregon to look for work or because of a job. Only answer if you are applying for health coverage for Person 2. £ Yes £ No
8.Does Person 2 live at the same address as you? £ Yes £ No
a.If no, why not? (choose one) £ Alcohol/drug rehab facility £ Foster care £ Incarcerated
£Job £ Long term medical care £ Mental health facility £ Military £ Other facility £ School
£Separate residence £ Short term medical care £ No home address
b.If no, list home address: _______________________________________________________________
9.Does Person 2 plan to file a 2017 federal income tax return in 2018? Answer “yes” if Person 2 plans to file, even if they will not owe taxes or are getting a refund. Person 2 can apply for health coverage, even if they don’t plan to file taxes.
£YES. If yes, complete
a.What will Person 2's filing status be on their 2017 tax return?
£ Single £ Head of household £ Qualifying Widow(er) Married filing: £ Jointly £ Separately
If married, spouse’s name?___________________________________________________________
b.Does Person 2 have any tax dependents? List all dependents regardless of their age or address. £ Yes £ No
First/last name and birthdate of each dependent: ________________________________________
________________________________________________________________________________
Note: for each person listed as a dependent, complete Step 2.
10.Is Person 2 claimed as a dependent on anyone else’s tax return? £ Yes £ No
If yes, list first/last name and birthdate of the tax filer:________________________________________
How is Person 2 related to the tax filer? ___________________________________________________
11.Is Person 2's 2016 tax filing information the same as listed for 2017?
£YES. £ NO. If no, complete Appendix D - 2016 Tax Filing Status
NEED HELP? Call us at |
5 |
|
OHA 7210 (Rev 09/16) |
||
|
|
STEP 2 |
Person 2, continued |
|
|
|
12.If Hispanic/Latino ethnicity — check all that apply
£Mexican £ Mexican American £ Chicano/a £ Puerto Rican £ Cuban £ Other £ Decline to answer
13.Race — check all that apply
£American Indian or Alaska Native £ Asian Indian £ Black or African American £ Chinese
£Filipino £ Guamanian or Chamorro £ Japanese £ Korean £ Native Hawaiian £ Other Asian
£Other Pacific Islander £ Samoan £ Vietnamese £ White £ Decline to answer
14.Is Person 2 applying for health coverage? Person 2 can apply even if they already have health coverage.
£YES. If yes, go to #15.
£NO. If no, and there is someone else you need to include on this application, skip to page 7. If there is no one else you need to include on this application, skip to page 11 for Step 3.
15.Is Person 2 a U.S. citizen or national? £ YES. If yes, skip to #17. £ NO
16.If Person 2 is not a U.S. citizen or national, does Person 2 have an eligible immigration status?
We only use this information to determine eligibility. See the Application Guide for more information
about eligible immigration statuses.
£YES. If yes, complete
a.Immigration document type: ____________________________________
b.Document ID #: _______________________________________________
c.Status: ______________________________________________________
d.Date status gained: _________________
e.Has Person 2 lived in the U.S. since 1996? £ Yes £ No
f.Is Person 2, their spouse or a parent a veteran or an
17.Is Person 2 the primary caretaker for any children under age 19 who: 1) live with Person 2 and 2) are related to Person 2 but are not Person 2's own children? For example, a grandparent who is the primary caretaker for a grandchild.
£ Yes £ No
If yes, list first/last name of child(ren). Do not include Person 2's adopted, biological or step children:
______________________________________________________________________________________
______________________________________________________________________________________
NEED HELP? Call us at |
6 |
|
OHA 7210 (Rev 09/16) |
||
|
|
|
|
STEP 2 |
ADDITIONAL HOUSEHOLD MEMBER – PERSON 3 |
|
|||
1. |
Legal name (first, middle, last and suffix) |
|
2. Maiden or other names used (first, middle, last) |
|||||
|
|
|
|
|
|
|
|
|
3. |
Relationship to you |
|
|
|
|
|
||
|
|
|
|
|
|
|||
4. |
Social Security number (SSN) – An SSN is required for everyone who is applying for health coverage and |
|||||||
|
|
|
who has one. An SSN is optional for others, but providing an SSN can speed up the application process. |
|||||
SSN: |
|
No: £Applied for SSN |
□Newborn Don’t have SSN □Not eligible for SSN □Refuses to obtain SSN |
|||||
5.Birthdate (MM/DD/YYYY)
6. Sex: £ Male £ Female
7.Does Person 3 live in Oregon? Answer yes, even if you are in Oregon to look for work or because of a job.
Only answer if you are applying for health coverage for Person 3. £ Yes £ No
8.Does Person 3 live at the same address as you? £ Yes £ No
a.If no, why not? (choose one) £ Alcohol/drug rehab facility £ Foster care £ Incarcerated
£Job £ Long term medical care £ Mental health facility £ Military £ Other facility £ School
£Separate residence £ Short term medical care £ No home address
b.If no, list home address: _______________________________________________________________
9.Does Person 3 plan to file a 2017 federal income tax return in 2018? Answer “yes” if Person 3 plans to file, even if they will not owe taxes or are getting a refund. Person 3 can apply for health coverage, even if they don’t plan to file taxes.
£YES. If yes, complete
a.What will Person 3's filing status be on their 2017 tax return?
£ Single £ Head of household £ Qualifying Widow(er) Married filing: £ Jointly £ Separately
If married, spouse’s name?___________________________________________________________
b.Does Person 3 have any tax dependents? List all dependents regardless of their age or address. £ Yes £ No
First/last name and birthdate of each dependent: ________________________________________
________________________________________________________________________________
Note: for each person listed as a dependent, complete Step 2.
10.Is Person 3 claimed as a dependent on anyone else’s tax return? £ Yes £ No
If yes, list first/last name and birthdate of the tax filer:________________________________________
How is Person 3 related to the tax filer? ___________________________________________________
11.If Hispanic/Latino ethnicity — check all that apply
£Mexican £ Mexican American £ Chicano/a £ Puerto Rican £ Cuban £ Other £ Decline to answer
12.Race — check all that apply
£American Indian or Alaska Native £ Asian Indian £ Black or African American £ Chinese
£Filipino £ Guamanian or Chamorro £ Japanese £ Korean £ Native Hawaiian £ Other Asian
£Other Pacific Islander £ Samoan £ Vietnamese £ White £ Decline to answer
NEED HELP? Call us at |
7 |
|
OHA 7210 (Rev 09/16) |
||
|
|
STEP 2 |
Person 3, continued |
|
|
|
13.Is Person 3 applying for health coverage? Person 3 can apply even if they already have health coverage.
£YES. If yes, go to #14.
£NO. If no, and there is someone else you need to include on this application, skip to page 9. If there is no one else you need to include on this application, skip to page 11 for Step 3.
14.Is Person 3 a U.S. citizen or national? £ YES. If yes, skip to #16. £ NO
15.If Person 3 is not a U.S. citizen or national, does Person 3 have an eligible immigration status?
We only use this information to determine eligibility. See the Application Guide for more information about eligible immigration statuses.
£YES. If yes, complete
a. Immigration document type: ____________________________________
b. Document ID #: _______________________________________________
c.Status: ______________________________________________________
d.Date status gained: _________________
e.Has Person 3 lived in the U.S. since 1996? £ Yes £ No
f.Is Person 3, their spouse or a parent a veteran or an
16.Is Person 3 the primary caretaker for any children under age 19 who: 1) live with Person 3 and 2) are related to Person 3 but are not Person 3's own children? For example, a grandparent who is the primary
caretaker for a grandchild.
£Yes £ No
If yes, list first/last name of child(ren). Do not include Person 3's adopted, biological or step children:
______________________________________________________________________________________
______________________________________________________________________________________
17.Is Person 3's 2016 tax filing information the same as listed for 2017?
£YES. £ NO. If no, complete Appendix D - 2016 Tax Filing Status
NEED HELP? Call us at |
8 |
|
OHA 7210 (Rev 09/16) |
||
|
|
|
|
STEP 2 |
ADDITIONAL HOUSEHOLD MEMBER – PERSON 4 |
|
|||
1. |
Legal name (first, middle, last and suffix) |
|
2. Maiden or other names used (first, middle, last) |
|||||
|
|
|
|
|
|
|
|
|
3. |
Relationship to you |
|
|
|
|
|
||
|
|
|
|
|
|
|||
4. |
Social Security number (SSN) – An SSN is required for everyone who is applying for health coverage and |
|||||||
|
|
|
who has one. An SSN is optional for others, but providing an SSN can speed up the application process. |
|||||
SSN: |
|
No: £Applied for SSN |
□Newborn Don’t have SSN □Not eligible for SSN □Refuses to obtain SSN |
|||||
5.Birthdate (MM/DD/YYYY)
6. Sex: £ Male £ Female
7.Does Person 4 live in Oregon? Answer yes, even if you are in Oregon to look for work or because of a job.
Only answer if you are applying for health coverage for Person 4. £ Yes £ No
8.Does Person 4 live at the same address as you? £ Yes £ No
a.If no, why not? (choose one) £ Alcohol/drug rehab facility £ Foster care £ Incarcerated
£Job £ Long term medical care £ Mental health facility £ Military £ Other facility £ School
£Separate residence £ Short term medical care £ No home address
b.If no, list home address: _______________________________________________________________
9.Does Person 4 plan to file a 2017 federal income tax return in 2018? Answer “yes” if Person 4 plans to file, even if they will not owe taxes or are getting a refund. Person 4 can apply for health coverage, even if they don’t plan to file taxes.
£YES. If yes, complete
a.What will Person 4's filing status be on their 2017 tax return?
£ Single £ Head of household £ Qualifying Widow(er) Married filing: £ Jointly £ Separately
If married, spouse’s name?___________________________________________________________
b.Does Person 4 have any tax dependents? List all dependents regardless of their age or address. £ Yes £ No
First/last name and birthdate of each dependent: ________________________________________
________________________________________________________________________________
Note: for each person listed as a dependent, complete Step 2.
10.Is Person 4 claimed as a dependent on anyone else’s tax return? £ Yes £ No
If yes, list first/last name and birthdate of the tax filer:________________________________________
How is Person 4 related to the tax filer? ___________________________________________________
11.If Hispanic/Latino ethnicity — check all that apply
£Mexican £ Mexican American £ Chicano/a £ Puerto Rican £ Cuban £ Other £ Decline to answer
12.Race — check all that apply
£American Indian or Alaska Native £ Asian Indian £ Black or African American £ Chinese
£Filipino £ Guamanian or Chamorro £ Japanese £ Korean £ Native Hawaiian £ Other Asian
£Other Pacific Islander £ Samoan £ Vietnamese £ White £ Decline to answer
NEED HELP? Call us at |
9 |
|
OHA 7210 (Rev 09/16) |
||
|
|
STEP 2 |
Person 4, continued |
|
|
|
13.Is Person 4 applying for health coverage? Person 4 can apply even if they already have health coverage.
£YES. If yes, go to #14.
£NO. If no, skip to page 11 for Step 3.
14.Is Person 4 a U.S. citizen or national? £ YES. If yes, skip to #16. £ NO
15.If Person 4 is not a U.S. citizen or national, does Person 4 have an eligible immigration status?
We only use this information to determine eligibility. See the Application Guide for more information about eligible immigration statuses.
£YES. If yes, complete
a. Immigration document type: ____________________________________
b. Document ID #: _______________________________________________
c.Status: ______________________________________________________
d.Date status gained: _________________
e.Has Person 4 lived in the U.S. since 1996? £ Yes £ No
f.Is Person 4, their spouse or a parent a veteran or an
16.Is Person 4 the primary caretaker for any children under age 19 who: 1) live with Person 4 and 2) are related to Person 4 but are not Person 4's own children? For example, a grandparent who is the primary
caretaker for a grandchild.
£Yes £ No
If yes, list first/last name of child(ren). Do not include Person 4's adopted, biological or step children:
______________________________________________________________________________________
______________________________________________________________________________________
17.Is Person 4's 2016 tax filing information the same as listed for 2017?
£YES. £ NO. If no, complete Appendix D - 2016 Tax Filing Status
NEED HELP? Call us at |
10 |
|
OHA 7210 (Rev 09/16) |
||
|
Form Characteristics
| Fact Name | Description |
|---|---|
| Form Purpose | The OHA 7210 form is used to apply for Oregon Health Plan coverage. |
| Governing Law | This application is governed by Oregon state law concerning public health programs. |
| Information Required | Applicants must provide personal information for all household members, including Social Security numbers, birth dates, and income details. |
| Contact Options | Help is available through a variety of channels, including a website and a customer service phone line. |
| Filing Instructions | After completing the application, it must be mailed or faxed to OHP Customer Service at the specified address or number. |
| Privacy Protection | All information provided is kept confidential in accordance with privacy laws. |
| Language Assistance | The form allows applicants to request assistance in different languages and in various formats such as Braille and large print. |
Guidelines on Utilizing Oha 7210
Once you have gathered the necessary information, you'll be ready to complete the OHA 7210 form. This form is essential for applying for health coverage through the Oregon Health Plan. Make sure to follow the steps carefully, providing accurate information for everyone in your household.
- Begin filling out the form by entering your legal name, including first, middle, last names, and suffix.
- If applicable, list any maiden or other names you have used.
- Provide your Social Security number (SSN). Remember, this is required for all applicants who have one.
- Enter your birthdate in the format MM/DD/YYYY.
- Indicate your sex by selecting male or female.
- Provide a contact phone number (home, work, or cell).
- Confirm whether you live in Oregon. Select "yes," even if you are there for work or job searching.
- Provide your email address.
- Next, input your home address, including apartment/unit number, city, county, state, and ZIP code. If you don’t have a home address, skip to item 15.
- If your home address is different from your mailing address, fill in the mailing address details.
- Specify your preferred language for communication.
- Indicate the preferred language for written communication.
- Answer whether you need written materials in an alternate format. If yes, specify which format you need.
- Indicate if you are pregnant, as well as whether anyone else in the household is pregnant.
- State whether you plan to file a 2017 federal income tax return. If yes, fill in the filing status and dependents' details.
- Confirm if you are claimed as a dependent on someone else’s tax return.
- Mark your ethnicity and race according to options provided.
- Answer whether your 2016 tax information is the same as listed for 2017.
- Confirm if you are applying for health coverage for yourself.
- If not a U.S. citizen, provide details on your immigration status.
- Finally, if you are a caretaker for children under 19 that are related but not your own, provide their names.
After you complete these steps, review the information for accuracy. Once confirmed, sign the application. It is essential to send it via mail or fax to the correct OHP Customer Service address provided in the form. This step ensures that your application is processed in a timely manner.
What You Should Know About This Form
What is the OHA 7210 form used for?
The OHA 7210 form is the application for the Oregon Health Plan (OHP) coverage. It collects essential information about you and your household members to determine eligibility for health coverage. Completing this form accurately is critical to ensure you receive the benefits for which you qualify.
What information do I need to fill out the application?
To complete the OHA 7210, gather the following details for everyone in your household: Social Security numbers, Alien Resident numbers (if applicable), birth dates, income details (e.g., pay stubs or W-2 forms), and information about any health insurance available to you through an employer. Be thorough and precise to avoid delays in processing.
Who should I include on this application?
Your household includes yourself, your legal spouse, your children (of all ages, if claimed as dependents on your taxes), your live-in partner if you share a child, and anyone else you include on your federal income tax return. If someone living with you is not on this list and seeks health coverage, they must submit a separate application.
How do I submit the OHA 7210 form after completing it?
Once you have finished the application, you can submit it by mail or fax. To mail the application, send it to OHP Customer Service, P.O. Box 14015, Salem, OR 97309-5032. The fax number for submissions is 503-378-5628. Remember to sign your application and ensure all necessary pages are included.
What happens after I submit my application?
Once submitted, the OHP team will review the information you provided. They'll assess your eligibility based on the details about your household, income, and any existing health coverage. You should receive a notification regarding your application status, so keep an eye on any correspondence from OHP.
Can someone help me with the application process?
Yes, help is readily available. You can connect with certified insurance agents or community application partners who provide assistance at no cost. Visit www.OregonHealthCare.gov to find local resources, or call OHP Customer Service at 1-800-699-9075. Assistance is available in multiple languages too.
What privacy measures are in place for my information?
All information you share through the OHA 7210 form will be kept private according to legal requirements. The information gathered will only be used to determine eligibility for health coverage. For specific privacy policies, you can refer to the Application Guide associated with this form.
What if I don't have a Social Security number?
If you do not have a Social Security number, that does not automatically disqualify you from applying. You should indicate that you do not have one on the application. Providing a Social Security number can speed up processing, but it is not necessary for everyone applying.
Common mistakes
Filling out the OHA 7210 form can be tricky, and several mistakes are common among applicants. One significant error is failing to include all household members. It’s crucial to include everyone you are responsible for financially, such as your spouse, children, and anyone else listed on your tax return. Forgetting to mention a member can affect your eligibility for health coverage.
Another frequent mistake is not providing accurate Social Security numbers. Each person applying for health coverage must include their SSN. If someone doesn’t have one, indicating that on the form is essential. Applicants sometimes skip this detail, which can lead to delays in processing your application.
Missing or incorrect income information is also a common pitfall. Applicants must report all sources of income accurately. Providing estimates or failing to include all income sources can result in an invalid application. It’s best to gather the necessary documentation, like pay stubs or W-2 forms, before starting.
Some individuals mistakenly leave out their health insurance details, assuming it’s not relevant. However, knowing about any available employer health insurance is mandatory when applying for the OHA 7210. This information helps determine your eligibility for coverage under the Oregon Health Plan.
Signatures are often overlooked. After completing the form, it’s crucial to sign it before submission. An unsigned application can lead to processing delays or rejection. Be sure to double-check the form for a signature before mailing or faxing it.
Additionally, applicants sometimes fail to provide a valid mailing address. Ensure that you include a current address where you can receive any correspondence regarding your application. If you don't have a permanent home, provide information about where you spend most of your time.
Lastly, many applicants do not seek help when needed. If you find any part of the OHA 7210 confusing, reaching out for assistance is vital. You can connect with a certified insurance agent or call OHP Customer Service. They can provide guidance about filling the form out correctly, preventing errors that could impact your health coverage.
Documents used along the form
When applying for Oregon Health Plan coverage using the OHA 7210 form, there are several additional documents and forms that may be required. Each of these documents helps to provide the necessary information for processing the application smoothly. Here’s a brief overview of six commonly used forms:
- OHA 5200: This form is often used for reporting income. Applicants can list their income sources and amounts on this form, providing a clearer picture of their financial status.
- OHA 3503: The household member declaration form helps identify all individuals within the household who may need health coverage. It ensures that each person’s details are officially recorded.
- OHA 7240: The verification of income request form is essential for buyers to confirm their earnings. This form supports the legitimacy of income information provided during the application process.
- OHA 3050: This form is used to document any current health coverage. Applicants provide details about any active insurance plans which may affect their eligibility.
- OHA 9010: If there are changes in household circumstances after submitting the application, this form is used to report any relevant updates, ensuring that the application reflects current situations.
- OHA 8410: This is the appeal form for applicants who wish to contest a denial of eligibility. It allows individuals to formally request a review of a decision that affects their health coverage.
Providing these documents alongside the OHA 7210 form can simplify the process and help you receive the appropriate coverage more quickly. Always double-check that everything is filled out correctly to avoid delays.
Similar forms
- Form 1040: The individual income tax return form used by U.S. taxpayers to report their income and calculate their tax liability. Similar to the OHA 7210, it requires personal information, an SSN, and details about dependents to determine eligibility for benefits.
- Medicaid Application: A state-specific application form for individuals seeking health coverage through Medicaid. Like the OHA 7210, it collects household information, social security numbers, and may assess income to establish qualification for benefits.
- Marketplace Application (Form 80040): Used for application to the Health Insurance Marketplace under the Affordable Care Act. This form collects similar data, including household composition, income, and SSNs, to determine eligibility for subsidies or insurance coverage.
- SNAP Application: The form required for food assistance benefits through the Supplemental Nutrition Assistance Program. It gathers personal, household, and income information, reflecting the same need for detailed applicant data as seen in the OHA 7210.
Dos and Don'ts
When filling out the OHA 7210 form for Oregon Health Plan coverage, there are specific actions to take and avoid to ensure accuracy and efficiency in processing your application. Below is a list of eight guidelines to consider.
- Do read the entire form carefully before starting.
- Do gather all necessary information for each household member, including Social Security numbers and income details.
- Do write legibly to prevent misunderstandings or delays.
- Do sign the application before submitting it; unsigned forms may be returned.
- Don't skip any questions that apply to you or your household members; incomplete applications may result in denial.
- Don't provide false information, as this can lead to legal consequences.
- Don't forget to check all boxes and sections relevant to your household's situation.
- Don't submit the application via email; use the provided mailing or fax options only.
Taking these precautions can enhance your chances of a smooth application process and timely approval.
Misconceptions
Below is a list of common misconceptions regarding the OHA 7210 form, along with clarifications for each:
- Misconception 1: You must have a Social Security number to apply.
- Misconception 2: Applications can be submitted without signatures.
- Misconception 3: Only children under a certain age need to be reported.
- Misconception 4: You cannot apply if you already have health coverage.
- Misconception 5: Only household members living at the same address need to be reported.
- Misconception 6: The process does not allow for corrections.
- Misconception 7: You cannot get assistance in other languages.
- Misconception 8: The application must be completed all at once.
- Misconception 9: You cannot apply if you do not plan to file taxes.
- Misconception 10: You need a lawyer to fill out the form correctly.
While having a Social Security number is required for individuals applying for health coverage who possess one, the application process can proceed without it for others in your household.
It is crucial to sign your application before mailing or faxing it. A signature indicates your consent and verification of the information provided.
All children you claim as dependents on your taxes, regardless of age, should be included in the application. This ensures accurate determination of eligibility and coverage.
You can still apply for health coverage even if you already have it. This may be beneficial if you are seeking to switch plans or obtain additional benefits.
Anyone you claim on your federal income tax return must be included in the application, even if they do not reside with you. This helps provide a complete picture of your household's composition.
If you discover errors after submission, you can contact OHP Customer Service to update your application. Providing accurate information is vital for processing.
The application process accommodates multiple languages. You can request help in a language of your choice, ensuring that language is not a barrier to obtaining coverage.
You can take your time to gather necessary information and complete the application. It is important to fill it out accurately, which may take some time.
You can apply for health coverage even if you do not intend to file federal income taxes. Eligibility is determined by additional criteria, not solely tax filing status.
A lawyer is not necessary to complete the OHA 7210 form. Support is available from certified insurance agents and community partners at no cost. They are prepared to guide you through the application process.
Key takeaways
1. Use Available Resources: If assistance is needed while filling out the OHA 7210 form, certified insurance agents and community partners can provide help at no cost. Visit www.OregonHealthCare.gov or call OHP Customer Service at 1-800-699-9075.
2. Gather Necessary Information: Before starting the application, gather essential information for everyone in your household, including Social Security numbers, birthdates, and details about income and available health insurance.
3. Include All Required Household Members: Ensure that all individuals who meet the criteria are included in the application. This includes your legal spouse, children, live-in partners, and others claimed on your federal tax return.
4. Sign and Submit the Application Correctly: After completing the application, be sure to sign it. Submit it by mailing it to OHP Customer Service or faxing it. The mailing address is P.O. Box 14015, Salem, OR 97309-5032, and the fax number is 503-378-5628.
5. Provide Clear and Accurate Information: Write clearly and accurately for each household member. If applying for more than four individuals, make copies of specific pages to include additional people.
6. Maintain Privacy: Understand that the information provided will be kept confidential as required by law. Familiarize yourself with the privacy policy in the Application Guide to know how your information is handled.
Browse Other Templates
Transcription Certificate - Transcripts are an important part of your academic history and future opportunities.
8668425178 - Consider the potential impact on your health coverage.
Transcript Retrieval Request,Academic Record Request Form,Official Transcript Order,Student Transcript Application,Transcript Delivery Request,Bluefield College Transcript Form,Transcription Request Document,Educational Record Request Form,Transcript - Be explicit about the urgency of your transcript request in your message.