Fill Out Your Oregon Dmv Accident Report Form
The Oregon DMV Accident Report Form, officially known as the Oregon Traffic Crash and Insurance Report, serves as a crucial document for drivers involved in specific automobile crashes. If the damages to a vehicle exceed $2,500, or if there are injuries, fatalities, or damaged property involved, drivers are required to complete and submit this form within 72 hours of the incident. The urgency of this process ensures that all necessary information is captured promptly, helping to maintain accurate records. Information is collected through a series of sections that include details about the crash such as date, time, and location, as well as specifics about the vehicles and parties involved. Notably, it's required for all drivers—even those licensed in other states—to report to the Oregon DMV if the criteria are met. In addition to the accident details, the form emphasizes the necessity of providing thorough insurance information to avoid potential penalties, including suspension of driving privileges. Finally, additional provisions exist for commercial vehicle operators and those dealing with totaled vehicles, ensuring comprehensive guidance is available for various situations. Completing this form accurately is paramount, as it helps the DMV maintain a clear record and ensures drivers comply with state law.
Oregon Dmv Accident Report Example
OREGON TRAFFIC CRASH AND INSURANCE REPORT
Tear this sheet off your report, read and carefully follow the directions.
ONLY drivers involved in a crash resulting in any of the following MUST file a Crash & Insurance Report: |
|||
• |
Damage to your vehicle is over $2500 |
• |
Damage to any one person’s property over $2500 |
• |
Injury (No matter how minor) |
• |
Any vehicle has damage over $2500 and any vehicle is |
• |
Death |
towed from the scene as a result of damages |
|
Oregon law requires these reports be filed within 72 hours of the crash. If you are not able to file within the 72 hours, submit it as soon as possible. If you fail to report the crash to DMV, it may result in suspension of your driving privileges. If the police department files a police report, you are still required to file your own Crash and Insurance Report with DMV. When required to report, even if you are licensed in another state, or you are not an Oregon resident, you still must file a report with Oregon DMV. DMV does not determine fault in a crash, but does post the crash to the driving record of those drivers required to report, unless the vehicle is parked. If you have questions, please call DMV Crash Reporting Unit at (503)
INSTRUCTIONS
PRINT OR TYPE ALL INFORMATION. (Use black or dark blue ink and press firmly.)
• Complete both sides of the form.
• If additional vehicles were involved in the crash, complete the attached Supplemental Report (Form
• DMV Headquarters will verify the insurance information submitted. Complete the insurance section or a suspension of your driving privileges may occur.
SECTION 1
DATE, LOCATION AND TIME — Clearly identify the date, location and time of the crash. The correct date, location and time is critical to processing your report. If you are unsure of the county, contact any local law enforcement agency for assistance.
SECTION 2
Your vehicle is Vehicle #1. Complete ALL fields. Provide Insurance company name (not agent), policy number, and Vehicle identification number (VIN). Failure to provide complete insurance and vehicle information may result in DMV issuing Notice of Suspension due to incomplete information.
SECTION 3
Failure to complete this section may result in DMV sending Notice of Suspension for failure to file a report. Principle purpose of driving and being paid to drive does not mean driving to reach a destination to perform a service. Property: Includes, but is not limited to, fixed or real property, landscaping, signs, parked vehicles, and animals.
COMMERCIAL MOTOR VEHICLE OPERATORS: In addition to this report, Oregon Administrative Rule requires that Form
You may now file the Motor Carrier Crash Report at: www.oregontruckingonline.com/cf/MCAD/pubMetaEntry/accidentRpt/
SECTION 4
OTHER VEHICLE (# 2) — Completion of this information will help DMV match all driver's crash reports more efficiently. If additional vehicles were involved in the crash, complete attached Supplemental Report (Form
SECTION 5
DESCRIPTION AND SIGNATURE — Describe what happened. It is important for you to sign and date the form. Only a family member may sign and date this form on behalf of a driver when the driver is incapacitated or physically unable to sign. No other signatures will be accepted.
COMPLETING AND FILING REPORT
HOW TO SUBMIT A REPORT TO DMV:
•Email to OregonDMVAccidents@odot.oregon.gov
•Fax to
•Mail to DMV Crash Reporting Unit 1905 Lana Ave NE, Salem, Oregon 97314
•Deliver to a DMV office
Keep a copy of the report and documentation that shows when you submitted your report to Oregon DMV. Under ORS 802.220(5), DMV is not authorized to provide you with a copy of the report that you file. If submitting by:
•Email, DMV sends an autoreply that your email was received. Save that autoreply.
•Fax, many fax machines provide the option to generate a fax confirmation report. Save that report.
•DMV Field Office, request and save that receipt.
PURSUANT TO OREGON INSURANCE LAW, AN INSURANCE COMPANY CAN NOT REQUIRE REPAIRS BE MADE TO A MOTOR VEHICLE BY A PARTICULAR PERSON OR REPAIR SHOP.
STK# 300009 |
INSTRUCTIONS
TOTALED VEHICLE NOTICE
DEFINITIONS AND INSTRUCTIONS FOR TOTALED VEHICLES
IF YOUR CRASH HAS RESULTED IN A “TOTALED” VEHICLE, YOU ARE REQUIRED BY LAW TO
FOLLOW APPROPRIATE INSTRUCTIONS IN THIS NOTICE.
DEFINITION OF “TOTALED” VEHICLE
“Totaled Vehicle” or “Totaled” as defined in Oregon law (ORS 801.527) means:
•A vehicle that is declared a total loss by an insurer who is obligated to cover the loss or a vehicle that the insurer takes possession of or title to.
•A vehicle that has sustained damage that is not covered by an insurer and the estimated cost to repair the vehicle is equal to at least 80% of the retail market value prior to the damage. “Retail market value” is defined as the amount shown in publications used by financial institutions (banks or lenders) in this state.
•A vehicle that is stolen, if it is not recovered within 30 days of theft and the loss is not covered by an insurer. In this situation, you must notify DMV within 60 days of the theft.
▼ FOLLOW THESE INSTRUCTIONS IF YOUR VEHICLE IS TOTALED ▼
If your vehicle is totaled, in addition to completing the crash report, follow the instruction that is applicable to your case. Either:
1.SURRENDER the title to the insurer if the damage is covered by an insurer who declares the vehicle to be a “total loss,” and the insurer takes possession of the vehicle; or
2.SURRENDER the title to DMV and apply for salvage title if the damage is covered by an insurer who declares the vehicle to be a “total loss,” but you keep possession of the vehicle; or
3.SURRENDER the title to DMV and apply for salvage title if the damage was not covered by an insurer and the estimated cost of repair is at least 80% of the retail market value of the vehicle before the damage; or
4.NOTIFY DMV that your vehicle has been totaled if, for some reason, you are unable to obtain the title for surrender. You must provide DMV with a signed statement which includes:
•A description of the vehicle which includes the year model, make, plate number and vehicle identification number.
•A statement indicating the vehicle has been totaled.
•A statement that you are unable to obtain the title and why.
DO NOT SUBMIT THE TITLE WITH THE CRASH REPORT. You can obtain the Application for Salvage Title (Form
NOTE: It is a Class A misdemeanor with a penalty of imprisonment and/or fine if you fail to comply with the above requirements. (ORS 819.012)
OREGON TRAFFIC CRASH AND INSURANCE REPORT
COMPLETE BOTH SIDES
Print Form
Reset Form
Complete this form if the traffic crash occurred on a highway or premise open to the public and meets at least one of the reporting requirements outlined in Section 3. Failure to report when required may result in DMV issuing Notice of Suspension. Call
SECTION 1
CRASH DATE |
DAY OF WEEK TIME OF DAY |
|
COUNTY |
|
|
|
|
|
DMV USE ONLY |
|
|
|
|
M T W TH F |
AM |
|
|
|
|
|
CRASH REF # _________________________________ ALIR |
INS CO |
|||
|
S SN |
PM |
|
|
|
|
|
|||||
ROAD ON WHICH CRASH OCCURRED (Name of street, road or route ) |
MILE POST |
|
TYPE OF CRASH - The crash involved one or more of the following: |
(Mark all that apply) |
||||||||
|
|
|
|
|
|
|
|
Two vehicles |
ATV / Snowmobile |
Parked vehicle |
||
NAME OF NEAREST INTERSECTING ROAD |
WITHIN |
FEET |
N |
S |
E |
W |
More than two vehicles |
Motorcycle |
Overturned vehicle |
|||
Motor Home / RV |
||||||||||||
|
|
NEAR |
MILES |
N |
S |
E |
W |
Fatality |
Animal |
|
||
|
|
Motorized Scooter |
|
|||||||||
NAME OF NEAREST CITY / TOWN |
WITHIN |
FEET |
N |
S |
E |
W |
Bicycle |
Personal (assisted) |
Fixed object / property |
|||
|
|
NEAR |
MILES |
N |
S |
E |
W |
Pedestrian |
mobility device |
Other ____________________ |
||
|
|
Train |
||||||||||
SECTION 2 (YOUR INFORMATION)
Complete ALL fields. Failure to provide complete information may result in DMV issuing Notice of Suspension.
DRIVER’S LAST NAME |
FIRST NAME |
MIDDLE NAME |
DRIVER’S LICENSE NUMBER |
STATE DATE OF BIRTH |
GENDER |
|
|
|
M |
F |
X |
DRIVER’S RESIDENCE ADDRESS |
CITY |
STATE |
ZIP CODE |
CHECK BOX |
|
|
|
|
|
IF ADDRESS |
|
MAILING ADDRESS (IF DIFFERENT THAN RESIDENCE) |
CITY |
STATE |
ZIP CODE |
CHANGE |
|
|
|
||||
VEHICLE OWNER’S NAME AND ADDRESS |
|
CITY |
STATE |
ZIP CODE |
SAME |
|
|
|
|
RENTAL? |
|
|
|
|
INSURANCE COMPANY NAME (NOT AGENT) AND ADDRESS |
CITY |
STATE |
ZIP CODE |
|
POLICY NUMBER |
VEHICLE IDENTIFICATION NUMBER |
|
STATE VEHICLE PLATE NUMBER |
YEAR MAKE & MODEL |
Check all statements that apply:
SECTION 3
 Damage to your vehicle was more than $2500.
Damage to your vehicle was more than $2500.
 Damage to any one person’s property (other than vehicle) was more than $2500.
Damage to any one person’s property (other than vehicle) was more than $2500.
 Your vehicle was towed from the scene as a result of damages.
Your vehicle was towed from the scene as a result of damages.

 You or passengers in your vehicle were injured.
You or passengers in your vehicle were injured.

 Collision with a parked vehicle.
Collision with a parked vehicle.

 The crash occurred while you were driving your employer’s vehicle.
The crash occurred while you were driving your employer’s vehicle.

 You were driving on your job and being paid for the principal purpose of driving.
You were driving on your job and being paid for the principal purpose of driving.

 You were being paid to drive and/or deliver persons or property.
You were being paid to drive and/or deliver persons or property.

 You were operating a government owned vehicle marked for transporting mail in accordance with government rules.
You were operating a government owned vehicle marked for transporting mail in accordance with government rules. 
 You were operating an authorized emergency vehicle.
You were operating an authorized emergency vehicle.
The crash occurred in a work or maintenance zone. ORS 811.230 |
|
|
|
A police officer came to the scene. |
City |
County |
State Police |
Name of police department: __________________________ |

 You were operating a commercial motor vehicle requiring you to have a commercial driver license.
You were operating a commercial motor vehicle requiring you to have a commercial driver license. 

 You were transporting hazardous material.
You were transporting hazardous material.

 A citation was issued to you. The citation was: ________________________________________________________
A citation was issued to you. The citation was: ________________________________________________________
SECTION 4 (OTHER VEHICLE # 2)
DRIVER’S NAME (LAST, FIRST, MIDDLE) |
DRIVER’S LICENSE NUMBER |
STATE |
DATE OF BIRTH |
GENDER |
|
|
|
|
|
|
M F X |
|
|
|
|
|
|
DRIVER’S ADDRESS |
CITY |
|
STATE |
ZIP CODE |
|
|
|
|
|
|
|
VEHICLE OWNER’S NAME AND ADDRESS |
CITY |
|
STATE |
ZIP CODE |
|

 SAME
SAME
INSURANCE COMPANY NAME (NOT AGENT) AND ADDRESS |
|
|
POLICY NUMBER |
VEHICLE IDENTIFICATION NUMBER |
STATE VEHICLE PLATE NUMBER YEAR MAKE & MODEL |
IF ADDITIONAL VEHICLES WERE INVOLVED IN THE CRASH, USE ATTACHED SUPPLEMENTAL REPORT (Form
DESCRIBE WHAT HAPPENED: (IF MORE SPACE IS NEEDED, SUBMIT ADDITIONAL PAGE)
5 |
|
|
SECTION |
I certify all information given on this report is true and accurate to the best of my knowledge. |
|
|
||
|
SIGNATURE OF PERSON MAKING REPORT |
PRINTED NAME OF PERSON MAKING REPORT |
|
X |
REASON DRIVER IS UNABLE TO SIGN REPORT |
|
IF NOT DRIVER’S SIGNATURE, STATE RELATIONSHIP |
|
DMV COPY
DAYTIME PHONE # |
|
DATE SIGNED |
|||
|
|||||
( |
) |
|
|
|
|
|
|
PHONE NUMBER OF DRIVER |
|||
|
|
( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
STK# 300009 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
WEATHER CONDITIONS |
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||
|
|
|
YOU INTENDED TO... |
YOUR VEHICLE |
|
|
|
|
|
|
|
|
|
|
YOUR RESIDENCE |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
Go straight ahead |
|
|
Passenger car, pickup, van |
|
|
|
Clear |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Local resident |
|
|
|
|||||||||||||||||||||||||||||||
|
|
Make right turn |
|
|
|
Military vehicle |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Raining |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(within 25 miles of crash site) |
|||||||||||||||||||||
|
|
Make left turn |
|
|
|
Taxicab |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Snowing |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Residing elsewhere in state |
||||||||||||||
|
|
Make “U” turn |
|
|
|
Emergency vehicle |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Fog |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
Any of the above and trailer |
|
|
|
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
College student |
|||||||||||||||||||||||||||||||||
|
|
Enter driveway (also |
|
|
Private or public agency |
|
|
|
|
|
|
|
ROAD SURFACE |
|
|
|
|
|
|
Military |
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||
|
|
mark left or right turn) |
|
|
transit vehicle |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Dry |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Temporary job |
|
|
|
||||||||||||||||
|
|
Remain stopped in traffic |
|
|
Bus |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Wet |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
YOU WERE HEADED |
|||||||||||
|
|
Enter parked position |
|
|
School bus |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Snowy |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
North |
|
East |
|
|
|
||||||||||
|
|
Slow or Stop |
|
|
|
Other |
|
|
|
|
|
|
Icy |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
South |
|
West |
|
|
|
|||||||||||||||||||||||
|
|
Leave driveway (also |
|
|
Motorcycle |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
On: ____________________ |
||||||||||||||||||
|
|
mark left or right turn) |
|
|
Motor Home / RV |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LIGHT CONDITIONS |
|
|
|||||||||||||||||||||||||||||||||||||||||||||||
|
|
Start in traffic lane |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Daylight |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(name of street, road or route) |
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OTHER DRIVER WAS HEADED |
||||||||||||||||||||||||||||
|
|
Leave parked position |
|
|
Personal (assisted) mobility device |
|
|
|
Dawn or dusk |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
North |
|
East |
|
|
|
|||||||||||||||||||||||||||||||||
|
|
|
|
Truck tractor & semi trailer |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||
|
|
Remain parked |
|
|
|
|
|
|
Darkness (lighted) |
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
South |
|
West |
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
Overtake and pass |
|
|
Truck/truck tractor |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Darkness (unlighted) |
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
Other truck combination |
|
|
|
|
|
|
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
On: ____________________ |
||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
Farm tractor/farm equip. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(name of street, road or route) |
|||||||||||||||||||||||||
|
WITNESS INFORMATION: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
If this crash involved a pedestrian or |
||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
bicyclist, complete the following: |
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PEDESTRIAN NAME |
|
BICYCLIST NAME |
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Pedestrian or bicyclist was going: |
|
|
|
||||||||||||||||||||||||||
|
|
|
|
OCCUPANT INJURY AND SAFETY EQUIPMENT INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
N |
|
|
|
|
S |
|
E |
W |
||||||||||||||||||||||||||||||||||
|
|
SAFETY EQUIPMENT CODES |
|
|
|
|
INJURY CODE FOR OCCUPANTS |
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
ALONG OR ACROSS: (name of street, road or route) |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
WRITE one of the codes |
|
WRITE one of the codes |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||
|
|
0 No seat belt available |
|
|
|
|
1 |
Fatal |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
From: |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||
|
|
1 Seat belt available but NOT used |
|
|
|
|
2 |
Suspected Serious: severe laceration, broken |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||
|
|
2 Seat belt available and in use |
|
|
|
|
|
or distorted limb, crush injury, significant burns, |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||
|
|
3 Child restraint device available but NOT used |
|
|
unconsciousness, paralysis |
|
|
|
|
|
|
To: |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||
|
|
4 Child restraint device in use |
|
|
|
|
3 Suspected Minor: lump, abrasions, bruises, |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||
|
|
5 Child restraint device not available |
|
|
|
|
|
minor lacerations |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EXAMPLE: (From: NE corner To: SE corner (or) From: East side To: West side, etc.) |
|||||||||||||||||||||||||||||||||||||||||||||||||
|
|
6 Helmet NOT in use |
|
|
|
|
4 Possible |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
7 |
Helmet in use |
|
|
|
|
|
5 No apparent |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Gender and age of pedestrian / bicyclist: |
||||||||||||||||||||||||||||||||||||||||||||
|
|
8 |
Air bag deployed |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
F |
|
X |
Age: _____ |
|
|
|
|||||||||||||||||
|
|
9 |
Air bag available - NOT deployed |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
10 |
Air bag NOT available |
|
|
|
|
GENDER CODE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Extent of pedestrian / bicyclist injury: |
|
|
|
|||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
WRITE M, F or X in column A |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Fatal |
|
|
|
|
|
Complaint of Pain |
|||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||
|
|
SEAT |
|
|
OCCUPANTS' NAMES |
(your vehicle) |
|
|
|
A |
|
|
B |
|
C |
|
|
D |
|
|
|
|
|
|
|
|
|
Suspected Serious |
No apparent injury |
|||||||||||||||||||||||||||||||||||||||||
|
|
POSITION |
|
|
GENDER |
|
|
AGE |
|
SFTY |
AIR |
INJURY |
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EQP |
BAG |
|
|
|
|
|
|
|
|
Visible injury |
|
|
(or none noted) |
|||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
DRIVER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Pedestrian / bicyclist action: (mark one) |
||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
|
|
FRONT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
|
|
CENTER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Crossing at intersection or crosswalk |
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
FRONT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Crossing not at intersection or crosswalk |
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
|
RIGHT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
MIDDLE |
* |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Walking / riding in roadway with traffic |
|
|
|
||||||||||||||||||||
|
|
LEFT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Walking / riding in roadway against traffic |
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
|
MIDDLE |
* |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
CENTER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Standing in roadway |
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
MIDDLE |
* |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Pushing or working on vehicles in roadway |
|||||||||||||||||||||||
|
|
RIGHT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Other working in road |
|
|
|
|
|
|
|||||||||||||||||
|
|
REAR |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
LEFT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Playing in road |
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
REAR |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hitchhiking |
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
CENTER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
REAR |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Not in roadway |
|
|
|
|
|
|
|||||||||||||||||
|
|
RIGHT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Other________________________________ |
|||||||||||||||||||||||
|
|
|
|
*Use only for vehicles with middle row of seats (i.e., vans, SUVs, etc.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(specify) |
|
|
|
|||||||||||||||||
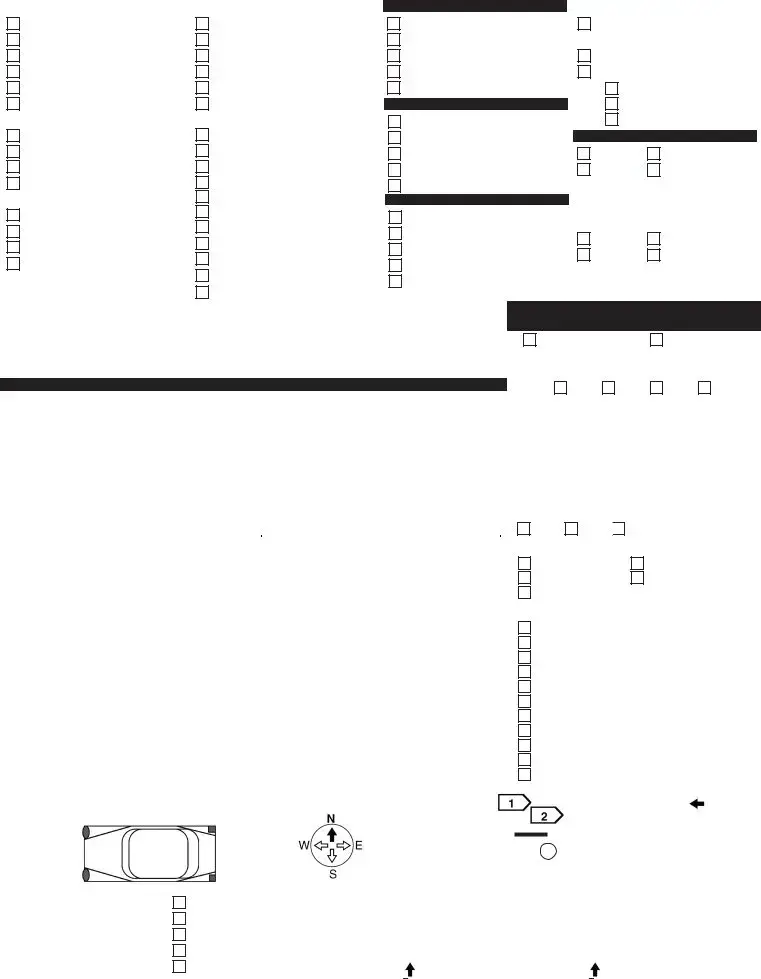
|
Vehicle Damage |
|
|
|
|
|
|
Diagram |
|
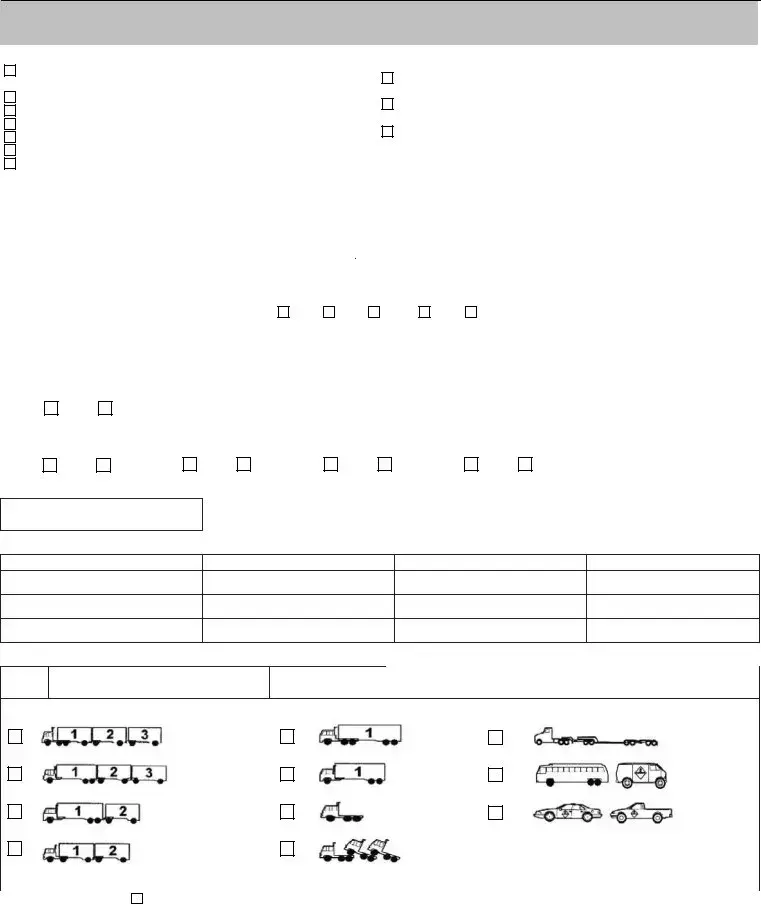
Number each vehicle: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
street, |
route) |
||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
FRONT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Show path by: |
|
|
|
|
|
|
|
|
|
|
|
|
U |
|
|
|
|
|
|
|
(nameof roador |
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Show pedestrian/bicyclist by: |
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Show railroad tracks by: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
USE ARROW TO SHOW |
Vehicle towed |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Show fixed object by: |
|
|
|
|
|
X |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
FIRST IMPACT (SHADE |
Rollover |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
IN DAMAGED AREA) |
Under car |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
Totaled |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
Unknown |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Your Vehicle (No. 1) damage: $ __________ . |
|
|
|
|
|
|
|
|
(name of street, |
|
|
|
|
|
|
|
|
|
|
|
(name of street, |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
road or route) |
|
|
|
|
|
|
|
|
|
|
|
|
|
road or route) |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SUPPLEMENTAL REPORT
OREGON TRAFFIC CRASH
Supplemental for more than two drivers involved in the crash.
Attach this form to your OREGON TRAFFIC CRASH AND INSURANCE REPORT.
|
CRASH DATE |
DAY OF WEEK |
TIME OF DAY |
AM |
COUNTY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M T W TH F |
|
|
|
|
DO NOT WRITE |
|
|
|
|
|
|
|
|
|
|
|
|
|
S SN |
|
PM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
IN THIS SPACE |
|
|
|
|
|
|
|
|
|
|
|
ROAD ON WHICH CRASH OCCURRED (Name of street, road or route ) |
MILE POST |
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VEHICLE |
INSURANCE COMPANY NAME (NOT AGENCY) |
|
|
|
|
|
POLICY NUMBER |
|
|
|
|
|
|||||
|
#3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VEHICLE IDENTIFICATION NUMBER |
|
|
|
VEHICLE PLATE NUMBER |
STATE |
YEAR |
MAKE & MODEL |
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
OTHER DRIVER’S FULL NAME (LAST, FIRST, MIDDLE) |
|
|
|
DRIVER’S LICENSE NUMBER |
|
STATE |
|
DATE OF BIRTH |
GENDER |
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
F |
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DRIVER’S ADDRESS |
|
|
|
|
|
CITY |
|
|
STATE |
ZIP CODE |
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VEHICLE OWNER’S NAME AND ADDRESS |
|
|
|
CITY |
|
|
STATE |
ZIP CODE |
|
|
|
|
|||||
|
SAME |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VEHICLE |
INSURANCE COMPANY NAME (NOT AGENCY) |
|
|
|
|
|
POLICY NUMBER |
|
|
|
|
|
|||||
|
#4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VEHICLE IDENTIFICATION NUMBER |
|
|
|
VEHICLE PLATE NUMBER |
STATE |
YEAR |
MAKE & MODEL |
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
OTHER DRIVER’S FULL NAME (LAST, FIRST, MIDDLE) |
|
|
|
DRIVER’S LICENSE NUMBER |
|
STATE |
|
DATE OF BIRTH |
GENDER |
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
F |
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DRIVER’S ADDRESS |
|
|
|
|
|
CITY |
|
|
STATE |
ZIP CODE |
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VEHICLE OWNER’S NAME AND ADDRESS |
|
|
|
CITY |
|
|
STATE |
ZIP CODE |
|
|
|
|
|||||
|
SAME |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VEHICLE |
INSURANCE COMPANY NAME (NOT AGENCY) |
|
|
|
|
|
POLICY NUMBER |
|
|
|
|
|
|||||
|
#5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VEHICLE IDENTIFICATION NUMBER |
|
|
|
VEHICLE PLATE NUMBER |
STATE |
YEAR |
MAKE & MODEL |
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
OTHER DRIVER’S FULL NAME (LAST, FIRST, MIDDLE) |
|
|
|
DRIVER’S LICENSE NUMBER |
|
STATE |
|
DATE OF BIRTH |
GENDER |
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
F |
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DRIVER’S ADDRESS |
|
|
|
|
|
CITY |
|
|
STATE |
ZIP CODE |
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VEHICLE OWNER’S NAME AND ADDRESS |
|
|
|
CITY |
|
|
STATE |
ZIP CODE |
|
|
|
|
|||||
|
SAME |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VEHICLE |
INSURANCE COMPANY NAME (NOT AGENCY) |
|
|
|
|
|
POLICY NUMBER |
|
|
|
|
|
|||||
|
#6 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VEHICLE IDENTIFICATION NUMBER |
|
|
|
VEHICLE PLATE NUMBER |
STATE |
YEAR |
MAKE & MODEL |
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
OTHER DRIVER’S FULL NAME (LAST, FIRST, MIDDLE) |
|
|
|
DRIVER’S LICENSE NUMBER |
|
STATE |
|
DATE OF BIRTH |
GENDER |
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
F |
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DRIVER’S ADDRESS |
|
|
|
|
|
CITY |
|
|
STATE |
ZIP CODE |
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VEHICLE OWNER’S NAME AND ADDRESS |
|
|
|
CITY |
|
|
STATE |
ZIP CODE |
|
|
|
|
|||||
|
SAME |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
VEHICLE |
INSURANCE COMPANY NAME (NOT AGENCY) |
|
|
|
|
|
POLICY NUMBER |
|
|
|
|
|
|||||
|
#7 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VEHICLE IDENTIFICATION NUMBER |
|
|
|
VEHICLE PLATE NUMBER |
STATE |
YEAR |
MAKE & MODEL |
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
OTHER DRIVER’S FULL NAME (LAST, FIRST, MIDDLE) |
|
|
|
DRIVER’S LICENSE NUMBER |
|
STATE |
|
DATE OF BIRTH |
GENDER |
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
F |
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
DRIVER’S ADDRESS |
|
|
|
|
|
CITY |
|
|
STATE |
ZIP CODE |
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
VEHICLE OWNER’S NAME AND ADDRESS |
|
|
|
CITY |
|
|
STATE |
ZIP CODE |
|
|
|
|
|||||
|
SAME |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SUPPLEMENTAL REPORT – USE IF MORE THAN TWO VEHICLES
CRASH ANALYSIS & REPORTING UNIT OREGON DEPARTMENT OF TRANSPORTATION POLICY, DATA & ANALYSIS DIVISION
555 13th ST NE STE 2 SALEM OR 97301 TELEPHONE
MOTOR CARRIER CRASH REPORT
(For CMV Drivers Only)
INSTRUCTIONS: IF YOU CHECKED A BOX UNDER THE QUALIFYING VEHICLE COLUMN AND A BOX UNDER THE CRITERIA COLUMN, COMPLETE THE MOTOR CARRIER CRASH REPORT AND SUBMIT TO THE ADDRESS SHOWN ABOVE. IF YOU HAVE ANY QUESTIONS REGARDING FILLING
OUT THE MOTOR CARRIER CRASH REPORT, PLEASE CALL (503)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
QUALIFYING VEHICLE |
|
|
|
|
|
|
|
|
|
CRITERIA |
|
|
|
|
|
|
|
|
|
|
||||
|
COMMERCIAL TRUCK (GVWR OVER 10,000 LBS OR ACTUAL WT |
|
ANY PERSON SUSTAINING A FATALITY (WITHIN 30 DAYS OF THE |
||||||||||||||||||||||
|
AT TIME OF CRASH EVEN IF GVWR IS SET UNDER 10,000 LBS ) |
|
|||||||||||||||||||||||
|
|
CRASH) |
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
HAZARDOUS MATERIAL PLACARD |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
ANY PERSON SUSTAINING INJURIES REQUIRING TREATMENT AWAY |
|||||||||||||||
|
COMMERCIAL BUS (DESIGNED FOR 8 OR MORE PASSENGERS) |
|
|||||||||||||||||||||||
|
|
FROM THE SCENE |
|
|
|
|
|
|
|
|
|||||||||||||||
|
FARM TRUCK INTERSTATE (OVER 10,000 LBS.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
ANY VEHICLE INCURRING DISABLING DAMAGE REQUIRING |
|||||||||||||||||||
|
FARM TRUCK |
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
REMOVAL FROM THE SCENE BY A TOW TRUCK OR ANOTHER |
||||||||||||||||
|
FARM TRUCK TOWING TRIPLE TRAILERS |
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
MOTOR VEHICLE |
|
|
|
|
|
|
|
|
||||||||
|
FARM TRUCK (OVER 80,000 LBS.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
MOTOR CARRIER NAME |
|
|
|
|
|
|
|
|
US DOT NUMBER |
|
|
|
|
AUTHORITY/FILE NUMBER |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
ADDRESS |
|
|
|
|
|
|
|
|
|
|
|
CITY |
|
|
|
|
|
STATE |
|
|
ZIP CODE |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DRIVER INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
DRIVER NAME (LAST, FIRST, MIDDLE) |
|
|
|
|
|
|
|
|
DATE OF BIRTH |
|
|
|
LENGTH OF EMPLOYMENT |
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MONTHS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
YEARS |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
CDL / DL NUMBER |
|
|
STATE |
|
|
|
|
|
LICENSE CLASS |
|
|
|
|
|
EXPIRATION DATE OF MEDICAL CERTIFICATE |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
A |
B |
C |
D |
M |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
COMPLETE THE FOLLOWING TWO QUESTIONS AS IF DOING A RECAP OF HOURS IN TIME DOCUMENTS AT TIME OF THE CRASH. |
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
AT TIME OF THE CRASH, TOTAL HOURS |
|
|
|
|
TOTAL HOURS ON DUTY DURING THE PREVIOUS |
|
|
7 CONSECUTIVE DAYS ____________ |
||||||||||||||||
|
DRIVING SINCE LAST |
|
|
|
|
(FILL OUT ONE ONLY, BASED ON TIME DOCUMENTS) |
|
|
8 CONSECUTIVE DAYS ____________ |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DOES YOUR DRIVER HAVE A MEDICAL WAIVER |
|
|
|
TYPE OF WAIVER (SIGHT, DIABETES, AMPUTEE, ETC.) |
|
|
|
|
|
|
|
|||||||||||||
|
YES |
NO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
DRIVER INJURY INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
YOUR DRIVER KILLED |
|
YOUR DRIVER INJURED |
|
|
RELIEF DRIVER KILLED |
RELIEF DRIVER INJURED |
|
TOTAL NUMBER OF PASSENGERS |
||||||||||||||||
|
YES |
NO |
|
YES |
NO |
|
YES |
NO |
|
YES |
NO |
|
_____KILLED |
_____ INJURED |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OTHER DRIVER INJURY INFORMATION
TOTAL NUMBER OF OTHER DRIVERS
_____KILLED |
_____ INJURED |
TOTAL NUMBER OF OTHER PASSENGERS |
|
TOTAL NUMBER OF PEDESTRIANS |
|
TOTAL NUMBER OF BICYCLISTS |
|||
_____KILLED |
_____ INJURED |
|
_____KILLED |
_____ INJURED |
|
_____KILLED |
_____ INJURED |
|
|
|
|
|
|
|
|
OTHER MOTOR CARRIER INFORMATION (IF 2 OR MORE MOTOR CARRIERS WERE INVOLVED)
MOTOR CARRIER NAME
VEHICLE LICENSE # AND STATE
DRIVER'S NAME
DRIVER'S LICENSE # AND STATE
MOTOR CARRIER VEHICLE INFORMATION
YEAR |
MAKE |
UNIT NUMBER |
LICENSE PLATE # & STATE - TRUCK/TRACTOR/BUS |
TOTAL NO. OF AXLES |
|
INCLUDING TRAILERS |
|
|
|
TRACTOR TYPE (SELECT APPROPRIATE TYPE) |
|
|
|
|
|
|
|||||
1 |
|
|
|
|
5 |
Standard |
|
|
|
9 |
Heavy Haul |
|
|
Triples (tractor with 3 trailers |
|
|
|
|
|
||||||
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
6 |
Tractor/Semi Trailer |
|
|
|
|
Bus/Van (8 or more |
|
|
|
|
|
|
|
|
|
|
|||
2 |
|
Triples (truck with 2 trailers) |
|
|
Straight Truck |
|
|
10 |
||||
|
|
|
||||||||||
|
|
|
|
|||||||||
3 |
|
|
|
|
7 |
|
|
|
11 |
passenger capacity) |
||
|
|
|
|
|
|
|
||||||
|
Straight |
|
|
|
|
|
Auto/Pickup |
|||||
|
|
|
|
|||||||||
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
4 |
|
Doubles (any) |
|
|
8 |
Saddlemount |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
COMPLETE REVERSE SIDE |
|
|
|
|
|
|
|
||||
SUPPLEMENTAL – MOTOR CARRIER CRASH REPORT
TRAILER TYPE (CHECK ONE)
|
VAN |
|
FLATBED |
|
TANKER |
|
|
CONTAINER |
|
|
POLE/LOG |
|
DUMP |
|
|
|
|
CAR CARRIER |
|
LIVESTOCK |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
MOBILE HOME TOTER |
|
PASSENGER |
|
|
GARBAGE |
|
|
|
|
|
MIXER |
|
SADDLEMOUNT |
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
WRECKER |
|
FIXED LOAD |
|
HEAVY HAUL |
|
|
UTILITY |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
COMMODITY INFORMATION
COMMODITY BEING TRANSPORTED AT TIME OF CRASH
WAS A HAZARDOUS COMMODITY BEING HAULED

 YES
YES  NO
NO
WAS HAZARDOUS MATERIAL RELEASED FROM THE VEHICLE CARGO(NOT A FUEL RELEASE)

 YES
YES  NO
NO
HAZARD CLASS
CRASH INFORMATION
LOCATION OF CRASH (NEAREST CITY OR TOWN) |
|
HIGHWAY AND MILEPOINT/STREET/COUNTY ROAD |
|
DIRECTION OF YOUR VEHICLE (CHECK) |
||||||||||
|
|
|
|
|
|
|
|
|
N |
S |
E |
W |
||
|
|
|
|
|
|
|
|
|
|
|
|
|||
DATE OF CRASH |
TIME |
|
|
AM |
DAY OF THE WEEK (CHECK ONE) |
|
|
|
|
|
|
|||
|
|
|
|
PM |
MON |
TUES WED THU |
FRI |
SAT |
SUN |
|||||
CONDITIONS AT TIME OF CRASH |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
WEATHER (CHECK ONE) |
1. CLEAR |
2. RAIN |
3. SNOW |
4. CLOUDY |
5. SLEET |
6. FOG |
7. OTHER |
|
|
|||||
ROAD SURFACE (CHECK ONE) |
1. DRY |
2. WET |
3. SNOWY |
4. ICY |
5. OTHER |
|
|
|
|
|
|
|
|
|
LIGHT CONDITION (CHECK ONE) |
1. DAY |
2. DAWN |
3. DUSK |
4. ARTIFICIAL LIGHTS |
5. DARK |
6. OTHER |
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DESCRIBE WHAT HAPPENED BY CHECKING ALL BOXES THAT APPLY. YOUR VEHICLE IS ALWAYS NO.1. IF OTHER VEHICLES WERE INVOLVED, COMPLETE COLUMNS 2 & 3 TO CORRESPOND TO THE ACTIONS OF THE SAME NUMBERED VEHICLES LISTED ABOVE UNDER "OTHER DRIVER INFORMATION".
VEHICLES 1 2 3
ACTION
SLOWING - STOPPING
STOPPED
BACKING
MAKING RIGHT TURN
MAKING LEFT TURN
MAKING U TURN
PROCEEDING STRAIGHT
INTERSECTION
ENTERING TRAFFIC (FROM SHOULDER, MEDIAN, PARKING STRIP OR PRIVATE DRIVE)
VEHICLES 1 2 3
ACTION
PASSING
CHANGING LANES
SIDESWIPE
SKIDDING
VEHICLE OUT OF CONTROL
CONTROLLED RR CROSSING
UNCONTROLLED RR CROSSING
RAN OFF ROAD
VEHICLES 1 2 3
ACTION
JACKKNIFE
OVERTURN
SEPARATION OF UNITS
FIRE
EXPLOSION
CARGO SHIFT
CARGO SPILL (HAZARDOUS)
CARGO SPILL
OTHER (DEER, GUARDRAIL, ETC)
DID YOUR VEHICLE STRIKE A PARKED VEHICLE

 YES
YES  NO
NO
WAS YOUR PARKED VEHICLE STRUCK BY ANOTHER VEHICLE

 YES
YES  NO
NO
DESCRIPTION OF CRASH (BY CARRIER OR DRIVER)
NAME AND TITLE OF PERSON SIGNING REPORT |
TELEPHONE NUMBER(S) |
|
|
SIGNATURE I CERTIFY THE INFORMATION PROVIDED IS TRUE AND ACCURATE |
DATE |
X |
|
Form Characteristics
| Fact Name | Details |
|---|---|
| Filing Requirement | Drivers must complete the Oregon Traffic Crash and Insurance Report if the damage exceeds $2,500, an injury occurs, or a vehicle is towed. |
| Deadline for Submission | The report must be filed within 72 hours of the crash. Delays can lead to issues, including suspension of driving privileges. |
| Responsibility to Report | All drivers involved in a qualifying crash, regardless of residency status, are required to file a report with Oregon DMV. |
| Police Reports | If a police report is filed, individuals are still obligated to submit their own Crash and Insurance Report to the DMV. |
| Crash Fault Determination | The DMV does not determine fault in a crash, but reports are recorded unless the vehicle was parked during the incident. |
| Additional Vehicle Information | In the case of multiple vehicles involved, completed supplemental forms are necessary for all drivers for efficient processing. |
| Insurance Verification | Insurance information, including company name and policy number, must be included. Incomplete info may lead to penalties. |
| Titled Vehicles and Salvage Title | If a vehicle is deemed "totaled," specific actions are required regarding the title, including surrendering it to either the insurer or DMV. |
| Communication with DMV | Drivers can submit the report via email, fax, mail, or in person at a DMV office. Always keep documentation of submission. |
| Legal Citations | ORS 802.220(5) governs the reporting requirements, while ORS 819.012 outlines penalties for failure to comply with the notice to DMV. |
Guidelines on Utilizing Oregon Dmv Accident Report
Filling out the Oregon DMV Accident Report form requires careful attention to detail. Accurate information must be provided to ensure that all necessary aspects of the accident are documented properly. Timely submission is also crucial, as Oregon law mandates that this report is filed within 72 hours of the incident. Following the provided steps can streamline the process and mitigate potential penalties.
- Begin by accessing the Oregon DMV Accident Report form. Ensure you have a clear workspace and the necessary documentation at hand.
- In Section 1, fill out the date, location, and time of the crash. Ensure correctness, as inaccuracies can delay processing.
- In Section 2, identify your vehicle as Vehicle #1. Complete all fields, including your insurance company name, policy number, and VIN. Incomplete data may lead to suspension notices.
- In Section 3, check all statements that apply regarding the consequences of the crash, such as damage amounts and injury statuses. Comprehensive reporting is vital here.
- If there were other vehicles involved, proceed to Section 4. Provide the details for Other Vehicle #2. Use the attached Supplemental Report for additional vehicles.
- Moving on to Section 5, summarize what happened during the incident. Your description should be concise yet comprehensive. Ensure to sign and date the report.
- Complete the reverse side of the form by providing any required further details.
- Choose a submission method. Options include email, fax, mail, or in-person delivery to a DMV office. Maintain a copy of the report and any submission receipt for your records.
What You Should Know About This Form
What is the Oregon DMV Accident Report form?
The Oregon DMV Accident Report form, also known as the Traffic Crash and Insurance Report, is a document that drivers involved in a vehicle crash must complete. This report is mandatory if the crash results in vehicle damage exceeding $2,500, property damage over $2,500, any form of injury, or if a vehicle is towed from the scene. The form must be submitted to the Oregon DMV within 72 hours of the accident.
Who is required to file an accident report?
Any driver involved in a crash that meets specific criteria must file an accident report with the Oregon DMV. Requirements include incidents where vehicle damage exceeds $2,500, property damage to someone else's property exceeding $2,500, any injuries sustained, or if a vehicle is towed from the scene. Furthermore, if a police report is filed, the driver is still obligated to file their own report with the DMV.
How can I submit the accident report?
There are several ways to submit the Oregon DMV Accident Report. You can email the completed form to OregonDMVAccidents@odot.oregon.gov, fax it to 503-945-5267, or mail it to the DMV Crash Reporting Unit at 1905 Lana Ave NE, Salem, Oregon 97314. Additionally, you have the option to deliver it in person to a DMV office. Be sure to keep a copy of the report and any documentation proving you submitted it.
What happens if I don’t file the report on time?
If you fail to file the accident report within the mandated 72-hour period, it is essential to submit it as soon as possible. Failure to report the crash may result in the suspension of your driving privileges. The DMV will send a Notice of Suspension if they do not receive your report on time.
What information do I need to provide on the form?
When completing the Oregon DMV Accident Report form, ensure that all sections are filled out accurately. You must provide details such as the date, time, and location of the crash, your vehicle's information, and the insurance details. Moreover, describe the incident clearly and sign the document. If additional vehicles were involved, complete the supplemental report form or include the necessary information on a blank piece of paper.
Common mistakes
Filling out the Oregon DMV Accident Report form can be a straightforward process if individuals pay attention to key details. One common mistake is neglecting to clearly state the date, location, and time of the crash. Providing accurate information is critical, as this details the circumstances surrounding the incident. If unsure of the county, individuals should contact local law enforcement for assistance rather than guessing, which may lead to a report being rejected or delayed.
Another frequent error is not completing all sections thoroughly. The insurance information section must be completed with the name of the insurance company, policy number, and the vehicle identification number (VIN). Omitting this information can result in the DMV issuing a Notice of Suspension of driving privileges. It's essential to ensure that no fields are left blank and all details are correct, as any mistakes can have serious repercussions.
Some people mistakenly believe that if the police file a report, they are exempt from submitting their own. This is incorrect. Regardless of any police involvement, individuals must still complete and file their accident report with the DMV. Failing to do so can lead to additional complications, including possible suspension of driving rights. Always remember to submit the form within the required 72-hour timeframe.
Lastly, individuals sometimes overlook the importance of signing and dating the report. This signature indicates that all provided information is true and accurate. If a driver cannot sign, only a family member may sign on their behalf under specific circumstances. Neglecting this step can result in the report being considered invalid, which can complicate the processing of claims or any legal matters arising from the crash.
Documents used along the form
When involved in an accident in Oregon, the DMV Accident Report form is one of several necessary documents that may need to be completed. Each of these forms helps to ensure accurate reporting and proper follow-up after an incident. Below is a list of documents frequently used in conjunction with the DMV Accident Report.
- Supplemental Accident Report (Form 735-32B): This form is used when there are more than two vehicles involved in a crash. It allows drivers to provide detailed information about additional vehicles and their drivers.
- Motor Carrier Crash Report (Form 735-9229): Required for commercial motor vehicle operators, this report must be filed within 30 days if a crash results in a fatality, injury, or towing due to disabling damage.
- Application for Salvage Title (Form 735-229): If a vehicle is deemed totaled, this form is needed to apply for a salvage title, allowing the owner to retain possession of the vehicle or surrender the title to the insurer.
- Police Report: If law enforcement is involved, a police report will be created. While it does not replace the DMV Accident Report, it complements it and provides official documentation of the incident.
- Insurance Claim Form: In order to file a claim for damages or injuries, individuals typically need to complete their insurance company’s claim form, which documents the details of the accident and supports their request for compensation.
- Witness Statements: Collecting statements from witnesses can provide additional perspectives about the accident, aiding in the claims process and any potential legal proceedings.
- Medical Reports: If any injuries occur as a result of the accident, medical documentation detailing the injuries and treatment received may be required for insurance claims or personal injury cases.
- Proof of Insurance: A copy of the insurance card or policy is often required to validate coverage at the time of the accident and can affect claims processing.
- Crash Scene Photos: Photographs taken at the scene can serve as valuable evidence for insurance claims, legal proceedings, or dispute resolutions regarding fault.
- Vehicle Damage Estimates: For assessing repair costs following an accident, an estimate from a repair shop can be necessary for insurance claims and negotiations.
It is crucial for individuals involved in a crash to be aware of and utilize these forms as needed. Proper documentation helps to streamline processes with the DMV and insurance providers, ensuring a clearer path to resolution.
Similar forms
- Police Report: Similar to the Oregon DMV Accident Report, a police report documents the details of a crash, including parties involved and any injuries sustained. Unlike the DMV form, police reports often include an officer's assessment of the situation and might indicate fault.
- Insurance Claim Form: This form is used to report an accident to an insurance company. Like the DMV report, it requires specific details about the incident, but it focuses on the financial aspects and the damages incurred rather than legal obligations.
- Incident Report: Often used in healthcare or workplace scenarios, an incident report details accidents and injuries. Both this report and the DMV form seek to gather accurate information about what occurred, but the incident report emphasizes workplace safety regulations.
- Vehicle Maintenance Records: These records track the condition and service history of a vehicle. While the DMV report captures incident specifics, maintenance records help establish a vehicle’s operational history before an accident, which may be relevant for insurance assessments.
- State-Level Crash Report: A broader version of the DMV form collected by some state agencies. It serves a similar purpose by documenting crash-related data for statistical analysis, but it may include additional information such as traffic conditions and road hazards present during the incident.
Dos and Don'ts
When filling out the Oregon DMV Accident Report form, here are five important do's and don'ts:
- Do: Ensure all information is printed or typed clearly, using black or dark blue ink. This helps avoid delays and misunderstandings.
- Do: Complete both sides of the form fully. Omitting details can lead to unnecessary complications, including potential suspension of your driving privileges.
- Do: Accurately supply the date, location, and time of the crash. This information is crucial for processing your report and avoiding legal issues.
- Do: Take note that you must file your report within 72 hours of the incident. If you cannot meet this deadline, submit the report as soon as possible.
- Do: Keep a copy of your report for your records, along with documentation proving when you submitted it.
- Don't: Neglect to include insurance information. Failure to provide this can result in a suspension of your driving privileges.
- Don't: Forget to describe what happened in detail. Incomplete descriptions may lead to further inquiries.
- Don't: Attempt to leave any section of the form blank. Each part is essential to ensure the proper handling of your case.
- Don't: Submit titles along with your crash report if your vehicle is totaled; follow the specific instructions provided for totaled vehicles.
- Don't: Rely solely on a police report. You are still required to submit your own accident report to the DMV, regardless of any police involvement.
Misconceptions
- Misconception 1: Only Oregon residents need to file an accident report.
- Misconception 2: If the police report is filed, you don’t need to do anything else.
- Misconception 3: You don’t have to report minor injuries.
- Misconception 4: You have plenty of time to file the report.
- Misconception 5: You can submit the report in any format.
- Misconception 6: You can sign the report for someone else.
- Misconception 7: A totaled vehicle doesn’t need to be reported.
- Misconception 8: You don’t need to worry about insurance details when filing.
Many people mistakenly believe that if they are not residents of Oregon, they don’t need to submit a report. In fact, any driver involved in a crash within Oregon must file a Crash & Insurance Report, regardless of their residency status.
While it's true that police officers may file a report, individuals involved in the crash are still required to file their own report with the DMV. This is a separate requirement and is crucial for maintaining your driving privileges.
Even if an injury seems minor, Oregon law mandates that any injury—no matter how small—be reported. Failure to report can lead to unexpected legal issues, including a potential suspension of driving privileges.
It's common to think that a few extra days won't make a difference, but the law requires that the report be filed within 72 hours of the crash. Delays can lead to penalties, including suspension.
While there are multiple ways to submit the report—such as email, fax, or mail—you must use the specific form provided by the DMV. Failure to use the correct format can result in complications.
Unless a driver is incapacitated, only that driver may sign their own report. A family member can only sign on their behalf if they are physically unable to do so, which is often misunderstood.
Many believe that once a vehicle is declared totaled, it doesn't need to be reported. However, if you have a totaled vehicle, specific laws require you to notify the DMV and surrender the title.
Providing complete and accurate insurance information is essential. Failure to do this may result in the DMV issuing a Notice of Suspension. Take special care to fill out the insurance section correctly.
Key takeaways
- Filing Requirement: If you've been in a crash with damages over $2,500 to your vehicle or someone else's property, or if there are injuries, you must file the Oregon DMV Accident Report.
- Deadline: Reports should be submitted within 72 hours of the crash. If you can't do this, send it in as soon as possible.
- License Status: Failing to file could lead to a suspension of your driving privileges.
- Police Reports: If the police file a report, you still need to submit your Accident Report to the DMV.
- Out-of-State Drivers: Even if you're not an Oregon resident, you must file a report if required.
- No Fault Determination: The DMV does not decide who is at fault in a crash, but they will record the incident on your driving record.
- Complete Information: Fill out both sides of the form, making sure to include all required fields. Missing details can lead to suspension notices.
- Insurance Details: Provide accurate insurance information. The DMV will verify this info, and incomplete insurance data can trigger a Notice of Suspension.
- Salvage Titles: If your vehicle is totaled, follow specific instructions for surrendering the title to either the insurer or the DMV.
- Submission Options: You can submit the report via email, fax, mail, or in person at a DMV office. Keep a copy and documentation of your submission method.
Browse Other Templates
How to Get Your College Transcript - Transcripts can be sent to multiple addresses, as indicated by the requester.
Patent Application Form Pdf - The application may be affected by a secrecy order, which limits electronic filing options.