Fill Out Your Patient Demographics Form
The Patient Demographics form is an essential document utilized by healthcare providers to gather vital information about patients, ensuring that they receive the appropriate medical care. This form requests key details such as the patient's name, address, birth date, and contact numbers, as well as emergency contact information. It inquires about the patient’s marital status, occupation, and insurance coverage, vital for determining financial responsibility and eligibility for services. Understanding race and religion can also assist in providing culturally competent care. Patients will also provide information regarding their referring physician, enhancing coordination in their medical treatment. Furthermore, this document incorporates an assignment of benefits and release of information section, where patients authorize their insurance providers to share necessary medical details and direct payments to the healthcare practice. The acknowledgment of privacy practices reinforces the commitment to safeguarding patient information. Completing this form accurately allows healthcare providers to tailor their services to meet patients' unique needs while maintaining compliance with regulatory standards.
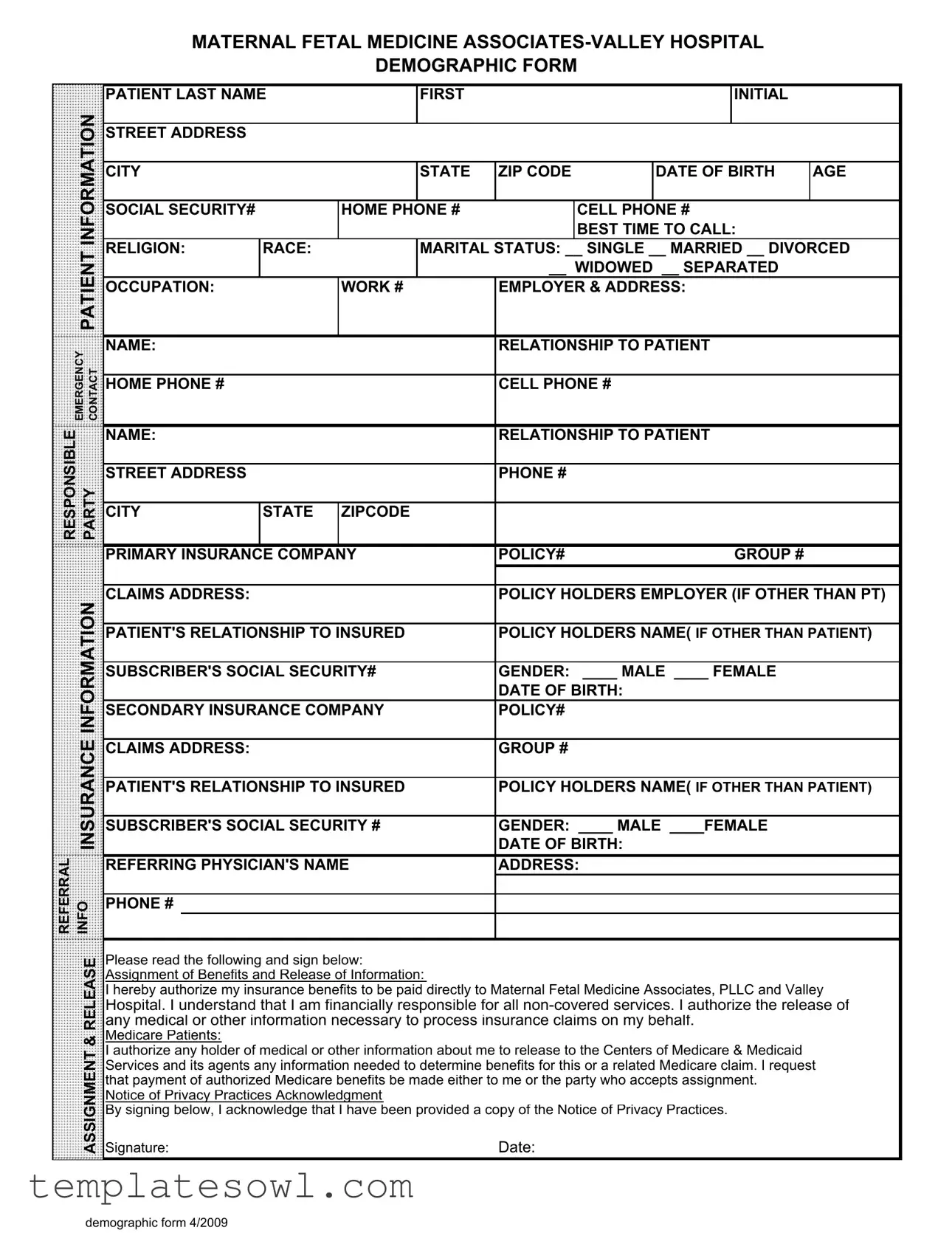
Patient Demographics Example
MATERNAL FETAL MEDICINE
DEMOGRAPHIC FORM
PATIENT LAST NAME |
FIRST |
INITIAL |
|
INFORMATION |
|
|
|
|
|
|
|
|
|
|
STREET ADDRESS |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
CITY |
|
|
STATE |
ZIP CODE |
DATE OF BIRTH |
AGE |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
SOCIAL SECURITY# |
|
HOME PHONE # |
|
CELL PHONE # |
|
|||
|
|
|
|
|
|
|
|
BEST TIME TO CALL: |
|
|
|
PATIENT |
RELIGION: |
RACE: |
|
MARITAL STATUS: __ SINGLE __ MARRIED __ DIVORCED |
|||||
|
|
|
|
|
|
__ WIDOWED __ SEPARATED |
|
|||
|
|
|
|
|
|
|
|
|||
|
|
OCCUPATION: |
|
WORK # |
EMPLOYER & ADDRESS: |
|
||||
|
|
|
|
|
|
|
|
|
|
|
EMERGENCY CONTACT |
NAME: |
|
|
|
RELATIONSHIP TO PATIENT |
|
||||
|
|
|
|
|
|
|
|
|
||
HOME PHONE # |
|
|
|
CELL PHONE # |
|
|
||||
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
||
RESPONSIBLE |
|
NAME: |
|
|
|
RELATIONSHIP TO PATIENT |
|
|||
PARTY |
|
|
|
|
|
|
|
|
|
|
STREET ADDRESS |
|
|
|
PHONE # |
|
|
||||
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
CITY |
STATE |
ZIPCODE |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
PRIMARY INSURANCE COMPANY |
POLICY# |
GROUP # |
|
|||||
|
|
|
|
|
|
|
|
|||
|
INFORMATION |
CLAIMS ADDRESS: |
|
|
|
POLICY HOLDERS EMPLOYER (IF OTHER THAN PT) |
||||
|
|
|
|
|
|
|
|
|
|
|
|
PATIENT'S RELATIONSHIP TO INSURED |
POLICY HOLDERS NAME( IF OTHER THAN PATIENT) |
||||||||
|
|
|||||||||
|
|
|
|
|
|
|||||
|
|
SUBSCRIBER'S SOCIAL SECURITY# |
GENDER: ____ MALE ____ FEMALE |
|
||||||
|
|
|
|
|
|
|
DATE OF BIRTH: |
|
|
|
|
|
SECONDARY INSURANCE COMPANY |
POLICY# |
|
|
|||||
|
INSURANCE |
|
|
|
|
|
|
|
|
|
|
CLAIMS ADDRESS: |
|
|
|
DATE OF BIRTH: |
|
|
|||
|
|
|
|
|
GROUP # |
|
|
|||
|
|
PATIENT'S RELATIONSHIP TO INSURED |
POLICY HOLDERS NAME( IF OTHER THAN PATIENT) |
|||||||
|
|
|
|
|
|
|||||
|
|
SUBSCRIBER'S SOCIAL SECURITY # |
GENDER: ____ MALE ____FEMALE |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
REFERRAL |
INFO |
REFERRING PHYSICIAN'S NAME |
ADDRESS: |
|
|
|||||
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
PHONE # |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RELEASE |
Please read the following and sign below: |
|
|
|
|
||||
|
Assignment of Benefits and Release of Information: |
|
|
|
|
|||||
|
|
|
|
|
|
|||||
|
|
I hereby authorize my insurance benefits to be paid directly to Maternal Fetal Medicine Associates, PLLC and Valley |
||||||||
|
|
Hospital. I understand that I am financially responsible for all |
||||||||
|
|
any medical or other information necessary to process insurance claims on my behalf. |
|
|||||||
|
& |
Medicare Patients: |
|
|
|
|
|
|
|
|
|
I authorize any holder of medical or other information about me to release to the Centers of Medicare & Medicaid |
|
||||||||
|
ASSIGNMENT |
|
||||||||
|
Signature: |
|
|
|
Date: |
|
|
|||
|
|
Services and its agents any information needed to determine benefits for this or a related Medicare claim. I request |
||||||||
|
|
that payment of authorized Medicare benefits be made either to me or the party who accepts assignment. |
|
|||||||
|
|
Notice of Privacy Practices Acknowledgment |
|
|
|
|
||||
|
|
By signing below, I acknowledge that I have been provided a copy of the Notice of Privacy Practices. |
|
|||||||
demographic form 4/2009
Form Characteristics
| Fact Name | Description |
|---|---|
| Patient Identification | The form collects personal details including last name, first initial, date of birth, and social security number. |
| Contact Information | It requests both home and cell phone numbers, along with the best time to call the patient. |
| Demographics | Patients provide their race, religion, marital status, and occupation to give context to their care. |
| Emergency Contact | The form requires an emergency contact person's name, relationship to the patient, and their phone numbers. |
| Insurance Details | Primary and secondary insurance information, including company names and policy numbers, are necessary for billing. |
| Signature Requirement | Patients must sign to authorize benefit assignments and release of medical information for insurance claims. |
| Medicare Information | Specific authorization for Medicare claims processing is included for patients eligible for these services. |
| Privacy Practices | Patients acknowledge receipt of a copy of the Notice of Privacy Practices by signing the form. |
| Updates | The demographic form was last updated in April 2009, which might affect its compliance with current laws. |
| State Specific Laws | This form may be subject to specific state laws governing patient information, such as HIPAA in the U.S. |
Guidelines on Utilizing Patient Demographics
Completing the Patient Demographics form is an important step in ensuring accurate and efficient medical care. Your details will help healthcare providers better understand your needs and manage your treatment effectively. Take a moment to gather any necessary documents, and follow the steps below to fill out the form accurately.
- Begin with your last name and first initial in the specified fields.
- Provide your street address, followed by the city, state, and ZIP code in the designated areas.
- Enter your date of birth and your current age.
- Fill in your Social Security number.
- List your home phone number and cell phone number.
- Indicate the best time to call you.
- Select your religion and race from the provided options.
- Choose your marital status by checking the appropriate box: SINGLE, MARRIED, DIVORCED, WIDOWED, or SEPARATED.
- Specify your occupation and provide your work phone number.
- List your employer's name and address.
- Fill in details for your emergency contact including their name, relationship to you, home phone number, and cell phone number.
- Provide the responsible party's name, their relationship to you, and their street address.
- Include the responsible party's phone number as well as their city, state, and ZIP code.
- Complete your primary insurance company details including the policy number and group number.
- Write the claims address for your primary insurance.
- List the policy holder’s employer (if different from you) along with the patient’s relationship to the insured.
- Provide the policy holder's name (if different from you) and their Social Security number.
- Select your gender by checking MALE or FEMALE.
- Fill in the date of birth for the policy holder (if different from you).
- For secondary insurance, repeat the steps for the insurance company, policy number, claims address, and other relevant details.
- Provide referral information, including the referring physician's name and address along with their phone number.
- Read and understand the release section, sign your name, and add the date to confirm your authorization for benefits assignment.
- Lastly, acknowledge receipt of the Notice of Privacy Practices by signing where indicated.
What You Should Know About This Form
What information is required on the Patient Demographics form?
The Patient Demographics form collects a variety of important information about the patient. This includes personal details such as the patient's name, address, date of birth, and contact numbers. Additionally, it requests socio-economic data like marital status, occupation, and employer information. The form also asks for insurance details, including primary and secondary insurance companies, policy numbers, and the relationship of the patient to the insured individual. Emergency contact information is also included, ensuring that staff can communicate effectively in case of an unexpected event.
How is the information used?
The information gathered in the Patient Demographics form serves multiple purposes. Firstly, it helps healthcare providers verify identity and contact details. Moreover, it is crucial for insurance billing by ensuring that proper claims can be submitted. Physicians also rely on this data to understand patient backgrounds, which can inform treatment decisions. Additionally, certain demographic information may help in research studies related to healthcare trends and outcomes.
Why is it important to complete the form accurately?
Completing the form accurately is vital for several reasons. Inaccurate information can lead to billing errors, which may result in unexpected charges for patients. It may also delay necessary medical services if verification is needed. Furthermore, having correct demographic data helps ensure compliance with regulations and can improve care by allowing healthcare providers to tailor services to diverse patient needs. Overall, accuracy supports both administrative efficiency and quality patient care.
Are there privacy protections for the information provided?
Yes, privacy protections are in place for the information provided on the Patient Demographics form. By signing the release section, patients are informed that their data will be used solely for medical and billing purposes. Healthcare providers are bound by laws such as the Health Insurance Portability and Accountability Act (HIPAA), which mandates the protection and confidentiality of patient information. Patients are also encouraged to review the Notice of Privacy Practices to understand how their information will be handled and what rights they have regarding its use.
Common mistakes
Completing the Patient Demographics form might seem straightforward, but many individuals stumble when providing their information. One common mistake is omitting essential details. Forgetting to include basic data such as the patient's last name or date of birth can lead to complications in medical records and billing processes. Even a simple left out digit in a phone number can create unnecessary delays in communication or emergency contact availability.
Another frequent error occurs when individuals incorrectly fill out their marital status. It's important to acknowledge your current relationship status, as it may impact various aspects of healthcare, including the classification of dependents or insurance coverage. By ticking the wrong box or leaving this section blank, a patient may create confusion or lead to complications regarding healthcare decisions.
Many people also mistakenly provide inaccurate emergency contact information. This crucial section should always include up-to-date names and phone numbers. If a medical emergency arises, having the right person contacted is vital. A missed call or a wrong number could result in a delay in getting help when it’s needed most.
Another mistake often made is neglecting to specify the best time to call. This is an important detail, especially if there are potential scheduling conflicts or if the healthcare provider’s office needs to reach the patient. A clear indication of when the patient is available can streamline communication and enhance the efficiency of scheduling appointments or discussing important medical information.
People often overlook the significance of accurately reporting their insurance information. Filling out the section with the correct company name, policy number, and group number is critical for seamless processing of claims. Errors in this section can cause unnecessary denials or delays in coverage, which ultimately lead to frustration and unexpected out-of-pocket expenses.
Finally, many forms feature a signature block for authorization. Patients often forget to sign or date the form, rendering it incomplete. This simple oversight can result in administrative headaches, delaying the processing of insurance claims or the commencement of care. Patients should remember that signing and dating the document confirms acceptance of the terms outlined in the form.
Documents used along the form
The Patient Demographics form is a crucial first step in collecting essential information about a patient. It serves to gather personal, insurance, and contact details necessary for effective medical care and billing. Several other forms and documents are typically used alongside it to ensure comprehensive patient management. Below is a list of commonly used documents.
- Medical History Form: This form collects information about the patient’s past medical conditions, surgeries, allergies, and any medications they are currently taking. It helps healthcare providers understand the patient’s health background.
- Consent for Treatment: This document provides the patient’s authorization to receive medical treatment. Patients acknowledge that they understand the procedures and potential risks involved in their care.
- Insurance Information Form: This form gathers detailed information about the patient’s primary and secondary insurance coverage. It includes policy numbers and the insured's details, ensuring accurate billing practices.
- HIPAA Privacy Notice: This document serves to inform patients of their rights regarding privacy and the handling of their healthcare information. It outlines how their information may be used and disclosed.
- Referral Form: When necessary, this form is used to refer patients to other specialists. It provides relevant patient details and the reason for the referral to ensure continuity of care.
- Financial Responsibility Agreement: Patients sign this document to acknowledge their financial responsibility toward services provided, including those not covered by insurance.
- Release of Information Form: This authorization allows healthcare providers to share the patient’s medical information with designated individuals, such as family members or other healthcare professionals.
- Advance Directive: This document outlines the patient’s preferences for medical treatment in case they become unable to communicate their wishes due to illness or injury.
- Patient Satisfaction Survey: After receiving care, patients often complete this survey to provide feedback on their experience, which helps healthcare providers improve their services.
Each of these forms plays a vital role in the patient care process, contributing to a comprehensive understanding of the patient’s needs and ensuring that their rights and responsibilities are clearly outlined. Together, they facilitate effective communication and management of healthcare services.
Similar forms
Intake Form: Like the Patient Demographics form, an intake form gathers essential information about the patient, including personal details, medical history, and current health concerns. Both documents serve to collect fundamental data to facilitate patient care.
Insurance Verification Form: This document is similar because it also collects insurance details necessary for billing and benefit determination. Both forms require information about the insurance company, policy numbers, and the patient’s relationship to the insured.
Medical History Form: The medical history form collects detailed information about the patient's past medical issues, medications, and surgeries. While the Patient Demographics form focuses on personal and contact details, both documents play a crucial role in understanding the patient's overall health.
Consent for Treatment Form: This form obtains permission from the patient to receive medical treatment. Similar to the Patient Demographics form, it includes signatures to confirm that patients understand what they are consenting to, reinforcing the patient’s rights in the medical process.
Dos and Don'ts
When filling out the Patient Demographics form, clarity and attention to detail are essential. Here are some helpful do's and don'ts to guide you through the process:
- Do ensure that all information is accurate and up to date.
- Do use complete names when specifying the patient and emergency contacts.
- Do provide the correct insurance information to avoid delays in processing.
- Do clearly indicate your preferred method of communication for contact.
- Do read through the form thoroughly before signing for acknowledgment of privacy practices.
- Don't leave any required fields blank, as this can cause complications.
- Don't use nicknames or abbreviations; always use formal names.
- Don't forget to check the accuracy of Social Security numbers and dates of birth.
- Don't rush through the form; take your time to ensure all details are correct.
Misconceptions
Understanding the Patient Demographics form is crucial for both patients and healthcare providers. However, several misconceptions often arise regarding this form. Here are ten of them:
- It’s only for insurance purposes. Many people think the Patient Demographics form solely serves to gather insurance information. In reality, it also collects important medical history and personal information that aid in treatment and patient care.
- You must fill out every section. Some believe that every field is mandatory. While it is important to provide as much information as possible, certain sections can be left blank if they are not applicable to your situation.
- Your information is not confidential. There is often a misconception that personal details shared on the form are not securely protected. In fact, healthcare providers are required by law to safeguard patients' information and maintain confidentiality.
- Only new patients need to complete it. Many individuals think that this form is only for new patients. However, established patients may also need to update their information regularly to ensure accuracy in their records.
- Providing your social security number is mandatory. People sometimes are unsure if they must give their Social Security number. This information is often requested for insurance purposes, but patients can decide not to provide it if they have concerns about privacy.
- It doesn’t impact your care. Some assume that this form does not play a role in their healthcare. On the contrary, accurate information can lead to better treatment options and improved patient outcomes.
- You should lie if you do not meet certain criteria. There is a belief that patients should provide false information to fit into specific categories. It’s important to be honest, as providing inaccurate data can lead to complications in care and billing.
- The form is only about demographics. While the name suggests this is solely about demographics, it covers a broad range of information including medical history, insurance details, and emergency contacts which are vital for comprehensive care.
- It can wait until later. Some people think they can fill out the form at their convenience. However, completing this form promptly ensures that healthcare providers have the necessary information before any treatment or consultation.
- Signing means you agree with everything. Finally, there’s a misunderstanding that by signing the form, patients are automatically agreeing to everything, including treatment. Signing simply acknowledges that you provided the information; it does not mean consent for treatment is given without further discussion.
By clarifying these misconceptions, patients can approach the Patient Demographics form with a clearer understanding of its purpose and importance in their healthcare journey.
Key takeaways
Completing the Patient Demographics form accurately is essential for seamless patient care and billing. Below are key takeaways to consider when filling out this form:
- Provide Complete Information: Ensure all fields are filled out accurately, including your full name, address, and date of birth. Incomplete forms may delay care or billing processes.
- Emergency Contact Details: Include a reliable emergency contact and their relationship to you. This information is critical for your safety and communication during medical emergencies.
- Insurance Information: Clearly list your primary and secondary insurance companies along with policy numbers and claim addresses. Accurate insurance details help in timely processing of claims and avoiding unexpected costs.
- Read and Sign: Before submitting, carefully read the Assignment of Benefits and Notice of Privacy Practices. Your signature indicates your understanding and consent regarding the use of your information.
Browse Other Templates
Dwc 69 Form - The form ensures that both the treating doctor and the certifying doctor provide consistent evaluations.
Audit List - Identifies the complexity of data reviewed for accuracy.