Fill Out Your Philhealth Registration Form
Filling out the PhilHealth Registration Form is an essential step for anyone looking to avail themselves of health benefits in the Philippines. This form serves as a way to register your information, update existing details, or make necessary amendments. Key components of the form include your personal information, such as your PhilHealth Identification Number (PIN), which is unique and should be used in all transactions. Additionally, you’ll provide details about your address, contact information, and any dependents you wish to enroll. It’s important to specify your member type—whether you are an employed individual, a migrant worker, or a self-earning individual, among others. There’s also a section for updating your details if anything has changed since your initial registration, so you’ll want to check the appropriate boxes and attach any supporting documents. Before you proceed, don’t forget to read the instructions on the back of the form, which guide you through the filling process and ensure accuracy. Properly completing this registration can set you on the path to enjoying the health coverage you deserve.
Philhealth Registration Example
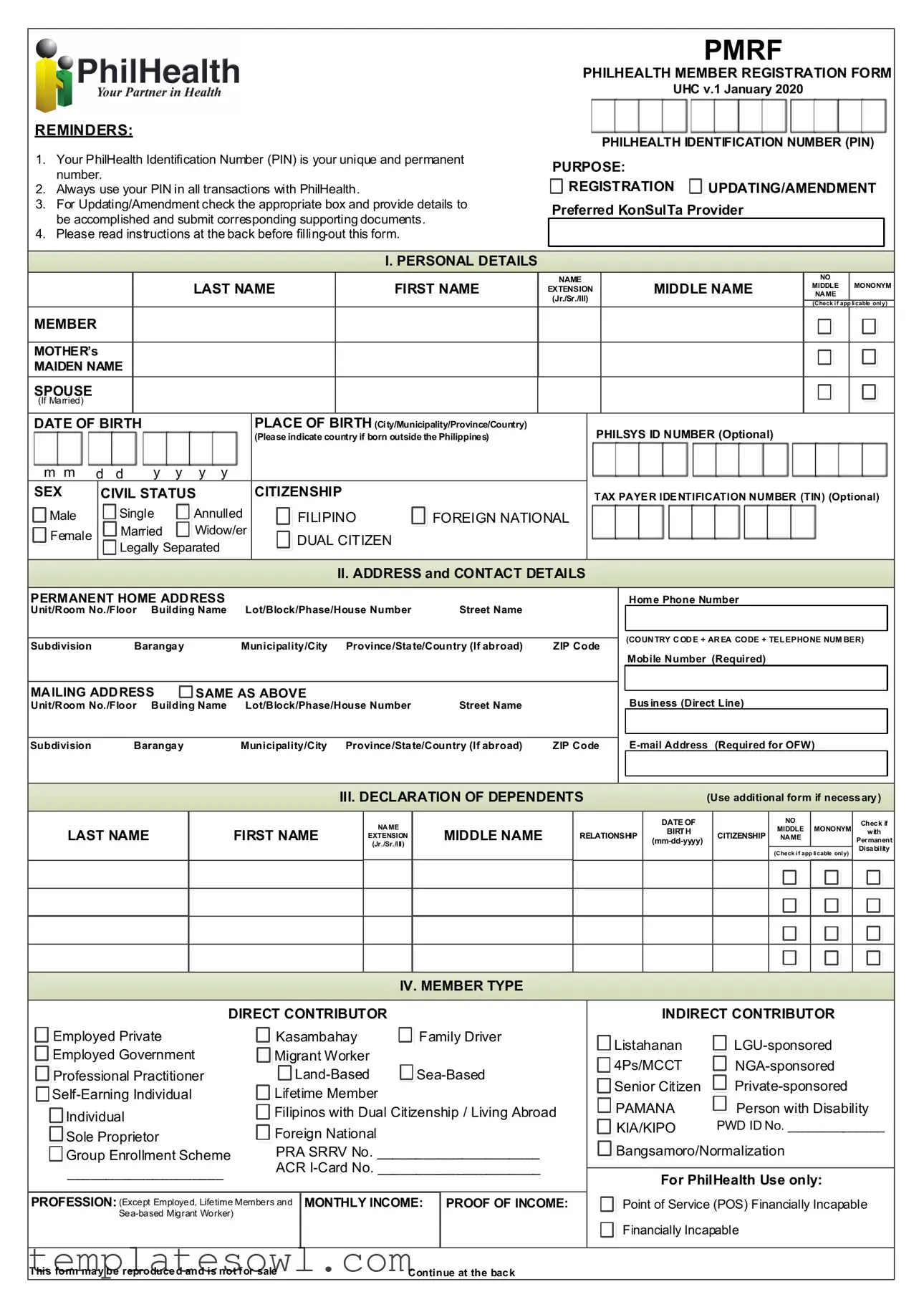
REMINDERS:
1.Your PhilHealth Identification Number (PIN) is your unique and permanent number.
2.Always use your PIN in all transactions with PhilHealth.
3.For Updating/Amendment check the appropriate box and provide details to be accomplished and submit corresponding supporting documents.
4.Please read instructions at the back before
PMRF
PHILHEALTH MEMBER REGISTRATION FORM
UHC v.1 January 2020
PHILHEALTH IDENTIFICATION NUMBER (PIN)
PURPOSE: |
|
REGISTRATION |
UPDATING/AMENDMENT |
Preferred KonSulTa Provider
I. PERSONAL DETAILS
|
|
NAME |
|
NO |
|
|
LAST NAME |
FIRST NAME |
MIDDLE NAME |
MIDDLE |
MONONYM |
||
EXTENSION |
||||||
NAME |
|
|||||
|
|
(Jr./Sr./III) |
|
|
|
|
|
|
|
(Check if app licable only) |
|||
|
|
|
|
|||
MEMBER
MOTHER’s
MAIDEN NAME
SPOUSE
(If Married)
DATE OF BIRTH |
|
|
PLACE OF BIRTH (City/Municipality/Province/Country) |
PHILSYS ID NUMBER (Optional) |
||
|
|
|
|
(Please indicate country if born outside the Philippines) |
||
m m |
d d |
y y |
y y |
|
|
|
SEX |
CIVIL STATUS |
CITIZENSHIP |
|
TAX PAYER IDENTIFICATION NUMBER (TIN) (Optional) |
||
Male |
Single |
Annulled |
FILIPINO |
FOREIGN NATIONAL |
|
|
Female |
Married |
Widow/er |
DUAL CITIZEN |
|
|
|
|
|
|
|
|
||
|
Legally Separated |
|
|
|||
|
|
|
|
|||
|
|
|
|
|
|
|
II. ADDRESS and CONTACT DETAILS
PERMANENT HOME ADDRESS
Unit/Room No./Floor Building Name |
Lot/Block/Phase/House Number |
Street Name |
|
|
|
|
|
|
|
Subdivision |
Barangay |
Municipality/City Province/State/Country (If abroad) |
ZIP Code |
|
MAILING ADDRESS |
SAME AS ABOVE |
|
|
|
Unit/Room No./Floor Building Name Lot/Block/Phase/House Number |
Street Name |
|
||
|
|
|
|
|
Subdivision |
Barangay |
Municipality/City Province/State/Country (If abroad) |
ZIP Code |
|
|
|
|
|
|
Home Phone Number
(COUNTRY CODE + AREA CODE + TELEPHONE NUMBER)
Mobile Number (Required)
Business (Direct Line)
III. DECLARATION OF DEPENDENTS |
(Use additional form if necessary) |
LAST NAME
FIRST NAME
NAME
EXTENSION (Jr./Sr./III)
MIDDLE NAME
RELATIONSHIP
DATE OF
BIRTH
CITIZENSHIP
NO
MIDDLE MONONYM NAME
(Check if app licable only)
Check if
with
Permanent Disability
IV. MEMBER TYPE
DIRECT CONTRIBUTOR
Employed Private |
Kasambahay |
Family Driver |
||
Employed Government |
Migrant Worker |
|
|
|
Professional Practitioner |
||||
Lifetime Member |
|
|
||
Individual |
Filipinos with Dual Citizenship / Living Abroad |
|||
|
|
|
|
|
Sole Proprietor |
Foreign National |
|
|
|
|
|
|
|
|
Group Enrollment Scheme |
PRA SRRV No. _____________________ |
|||
____________________ |
ACR |
|||
|
|
|
|
|
|
|
|
||
PROFESSION: (Except Employed, Lifetime Members and |
MONTHLY INCOME: |
PROOF OF INCOME: |
||
|
|
|
|
|
|
|
|
|
|
INDIRECT CONTRIBUTOR
Listahanan |
|
4Ps/MCCT |
|
Senior Citizen |
|
PAMANA |
Person with Disability |
KIA/KIPO |
PWD ID No. ______________ |
 Bangsamoro/Normalization
Bangsamoro/Normalization
For PhilHealth Use only:

 Point of Service (POS) Financially Incapable
Point of Service (POS) Financially Incapable 
 Financially Incapable
Financially Incapable
This form may be reproduced and is not for sale |
Continue at the back |
V. UPDATING/AMENDMENT
Please check: |
FROM |
TO |
Change/Correction of Name
(Last Name, First Name, Name Extension (Jr./Sr./III) Middle Name)

 Correction of Date of Birth
Correction of Date of Birth

 Correction of Sex
Correction of Sex

 Change of Civil Status
Change of Civil Status
Updating of Personal Information/Address/
Telephone Number/Mobile
Address
Under penalty of law, I hereby attest that the information provided, including the documents I have attached to this form, are true and accurate to the best of my knowledge. I agree and authorize PhilHealth for the subsequent validation, verification and for other data sharing purposes only under the following circumstances:
As necessary for the proper execution of processes related to the legitimate and declared purpose;
The use or disclosure is reasonably necessary, required or authorized by or under the law; and,
Adequate security measures are employed to protect my information.
_________________________________________________ |
_________________ |
|
Member’s Signature over Printed Name |
Date |
Please affix right |
|
|
|
|
|
thumbmark if unable to write |
FOR PHILHEALTH USE ONLY
RECEIVED BY:
Full Name:
______________________________
PRO/LHIO/Branch:
_____________________________
Date & Time:
______________________________
INSTRUCTIONS
1.All information should be written in UPPER CASE/CAPITAL LETTERS. If the information is not applicable, write “N/A.”
2.All fields are mandatory unless indicated as optional. By affixing your signature, you certify the truthfulness and accuracy of all information provided.
3.A properly accomplished PMRF shall be accompanied by a valid proof of identity for first time registrants, and supporting documents to establish relationship between member and dependent/s for updating or request for amendment.
4.On the PURPOSE, check the appropriate box if for Registration or for Updating/Amendment of information.
5.Indicate preferred KonSulTa provider near the place of work or residence.
6.For PERSONAL DETAILS, all name entries should follow the format given below. Check the appropriate box if registrant has no middle name and/or with single name (mononym).
LAST NAME |
FIRST NAME |
NAME EXTENSION (JR./SR./III) |
MIDDLE NAME |
SANTOS |
JUAN ANDRES |
III |
DELA CRUZ |
7.Indicate registrant’s/member’s name as it appears in the birth certificate.
8.The full mother’s maiden name of registrant/member must be indicated as it appears in the birth certificate.
9.Indicate the full name of spouse if registrant/member is married.
10.Indicate the complete permanent and mailing addresses and contact numbers.
11.For updating/amendment, check the appropriate box to be updated/amended and indicate the correct data.
12.For MEMBER TYPE, check the appropriate box which best describes your current membership status.
13.For Direct Contributors, except employed,
14.For
15.In declaring dependents, provide the full name of the living spouse, children below 21 years old, and parents who are 60 years old and above totally dependent to the member.
16.Dependents with disability shall be registered as principal members in accordance with Republic Act 11228 on mandatory PhilHealth coverage for all persons with disability (PWD).
17.The registrant must affix his/her signature over printed name (or right thumbmark if unable to write) and indicate the date when the PMRF was signed.
Form Characteristics
| Fact Name | Description |
|---|---|
| Unique Identifier | The PhilHealth Identification Number (PIN) serves as a unique and permanent identifier for each member. |
| Usage of PIN | Members must always use their PIN for all transactions with PhilHealth to ensure proper identification and access to services. |
| Updating Information | When updating or amending details, members should check the appropriate box on the form and provide supporting documents. |
| Instructions | It's crucial to read the instructions on the back of the form before filling it out to avoid mistakes. |
| Documentation Requirement | Members submitting the PMRF for the first time must accompany it with a valid proof of identity and any necessary documentation of dependencies for updates. |
| Member Type Categorization | The form allows members to classify themselves according to their membership status, including categories like 'Direct Contributor' and 'Indirect Contributor.' |
| Dependents Information | Members can declare dependents, such as their spouse or children, and must include details like names and dates of birth. |
| Legislation Reference | Updates concerning dependents with disabilities align with Republic Act 11228, which mandates coverage for all persons with disabilities. |
| Signature Requirement | Members are required to sign the form or, if unable to write, to affix their right thumbmark, attesting to the accuracy of the provided information. |
Guidelines on Utilizing Philhealth Registration
Filling out the PhilHealth Registration Form is an important step for anyone looking to enroll or update their membership in the Philippine Health Insurance Corporation. Ensure that all information provided is accurate and complete, as it will be used for your health insurance coverage.
- Obtain the PhilHealth Member Registration Form (PMRF) from an authorized source.
- Read the instructions carefully, including the directions on the back of the form.
- Write in upper case or capital letters throughout the form.
- In the Purpose section, check the box that indicates whether you are registering or updating your information.
- In the Personal Details section, fill in your full name as it appears on your birth certificate:
- Last Name
- First Name
- Middle Name
- Name Extension (if applicable, e.g., Jr., Sr.)
- Provide your mother’s maiden name and, if applicable, your spouse’s name.
- Fill out your date and place of birth, ensuring proper format.
- Indicate your Sex, Civil Status, and Citizenship.
- If you have a Taxpayer Identification Number (TIN), include that as well (optional).
- In the Address and Contact Details section, provide your permanent home address and mailing address, if different.
- Enter your home phone number, mobile number (required), and email address (required for overseas Filipino workers).
- If you have dependents, fill out the Declaration of Dependents section, listing their names, relationship, and dates of birth.
- In the Member Type section, check the appropriate box that describes your membership status.
- If applicable, specify your profession and monthly income in the provided fields.
- Sign and date the form, ensuring the signature matches the printed name.
- If you cannot write, affix your right thumbprint where indicated.
- Attach any required supporting documents based on the reason for filling out the form.
After completing the form, submit it along with any required documents to the nearest PhilHealth office for processing. Ensure that you keep a copy for your records.
What You Should Know About This Form
What is the PhilHealth Identification Number (PIN) and why is it important?
The PhilHealth Identification Number (PIN) is a unique and permanent number assigned to each member. It serves as your personal identifier for all transactions with PhilHealth. Using your PIN ensures that your records are accurately maintained and helps streamline any processes related to benefits and claims.
How do I fill out the PhilHealth Registration form?
When filling out the form, use uppercase letters for all information. Ensure that each mandatory field is completed accurately. If some information does not apply to you, indicate “N/A.” Pay close attention to the personal details section, where your name should match exactly how it appears on your birth certificate. Review the instructions on the back of the form before submission to avoid mistakes.
What should I do if I need to update or amend my information?
If you need to update your personal details, check the appropriate box on the form and provide the necessary new information. You will also need to submit supporting documents that verify the changes. Common updates include changes to your name, date of birth, or contact details.
Are there requirements for declaring dependents on the form?
Yes, when declaring dependents, you should include your spouse, children under 21, and parents aged 60 and above who are fully dependent on you. Provide their full names, relationships, and birth dates. If any dependents have a permanent disability, they may be registered as principal members under specific regulations.
What kind of proofs are accepted when declaring income as a Direct Contributor?
As a Direct Contributor, you must provide valid proof of income, which could include payslips, tax returns, or any official document that demonstrates your monthly earnings. If you are self-employed or under a special classification, specify your monthly income directly on the form.
What should I do if I cannot write my signature?
If you are unable to write your signature, you may affix your right thumbmark on the designated space on the form. Ensure that your printed name is provided right next to your thumbmark to validate your identity.
Common mistakes
Filling out the PhilHealth Registration Form is a crucial step for individuals seeking health insurance coverage in the Philippines. However, mistakes can lead to delays or complications. One common mistake is not providing a complete or accurate PhilHealth Identification Number (PIN). The PIN is essential for identification and must be used in all transactions. Leaving this field blank, or entering an incorrect number, can result in errors that later affect an individual's eligibility or access to services.
Another frequent error occurs in the personal details section. It is important that all names are written exactly as they appear on the birth certificate or legal identification. Miswriting someone's name, particularly the middle name or suffix, can lead to significant verification issues. This misalignment can cause delays in processing and may require individuals to submit additional documents to correct the information.
Many applicants also fail to indicate their permanent and mailing addresses correctly. Omissions or inaccuracies in these details may affect communication from PhilHealth regarding membership status, benefits, or updates. A complete address, including vital components such as the proper ZIP code, is necessary to ensure timely correspondence. It is advisable to double-check these entries to avoid confusion and ensure compliance with PhilHealth's requirements.
Finally, an oversight in declaring dependents can lead to challenges. Applicants must accurately declare their living spouse, children under 21, and parents over 60 who are financially dependent. Failing to include relevant dependents may result in denied coverage or reduced benefits. Ensuring that all information is precise and comprehensive is key to a successful registration process.
Documents used along the form
The Philhealth Registration Form (PMRF) is essential for individuals seeking membership or making updates to their information within the Philippine health insurance system. However, there are several other important documents that may accompany the PMRF. Each serves a specific purpose in the registration process or in the updating of member information.
- Proof of Identity: This document is required for first-time registrants to confirm their identity. Acceptable forms often include government-issued IDs such as a passport or driver's license, which must contain a photograph and personal details.
- Certificate of Birth: A birth certificate serves to verify the member's identity and date of birth. This is particularly important when there is a need to establish the correct name and age of dependents.
- Proof of Relationship: When registering dependents, documentation that establishes the relationship between the member and the dependent is necessary. This could be a marriage certificate for a spouse or a birth certificate for children.
- Tax Identification Number (TIN): Though optional, providing a TIN is useful for members, especially for those who are employed or self-employed. It helps streamline the processing of benefits and contributions within the Philhealth system.
Having these documents ready can facilitate a smoother registration process. It is important to ensure that all provided information is accurate and complete, as this will avoid potential issues when accessing healthcare services covered by Philhealth.
Similar forms
The PhilHealth Registration Form shares similarities with several important documents that aid in health coverage and identification. Here’s how it compares to each of these documents:
- Social Security Administration Form: Like the PhilHealth form, the Social Security Administration (SSA) form collects personal identification details such as name, birth date, and contact information. Both forms require proof of identity and provide unique identification numbers for tracking and services.
- Health Insurance Marketplace Application: This application is akin to the PhilHealth form because it gathers comprehensive personal information to determine eligibility for health coverage. Both forms include sections for dependents and offer guidance on how to correct or update information.
- Medicare Application Form: Similar to the PhilHealth Registration Form, the Medicare application requires detailed personal and demographic information. Both are essential for accessing health care services and require the applicant's signature to confirm the correctness of provided information.
- Employer Health Benefits Enrollment Form: This document, like the PhilHealth form, captures personal and dependent information for enrollment in a workplace health plan. Both require individuals to indicate their preferred provider and accurately report their circumstances, such as marital status and dependents.
Dos and Don'ts
When filling out the PhilHealth Registration form, being precise and attentive can make a significant difference. Here are ten essential dos and don’ts to keep in mind:
- Do write all information in UPPER CASE/CAPITAL LETTERS.
- Do ensure your PhilHealth Identification Number (PIN) is entered correctly.
- Do check the appropriate box for registration or updating/amendment purposes.
- Do provide valid proof of identity if you are a first-time registrant.
- Do include all required personal details, like your mother’s maiden name and spouse name if married.
- Don't leave any mandatory fields blank; write “N/A” if a section does not apply to you.
- Don't use nicknames or casual names; use names exactly as they appear on official documents.
- Don't forget to list dependents who are eligible for coverage.
- Don't submit the form without a proper signature or thumbmark if you cannot sign.
- Don't discard the instructions; they provide guidance on each part of the form.
Following these guidelines can lead to a smoother registration process and better service from PhilHealth.
Misconceptions
- Misconception 1: The PhilHealth Identification Number (PIN) can change over time.
- Misconception 2: You don’t need to submit any documents when filling out the registration form.
- Misconception 3: Filling out the form is optional for all members.
- Misconception 4: You can fill out the form in any format.
- Misconception 5: Only individuals in specific job categories can register.
This is not true. Your PIN is unique and permanent. It remains the same for all your transactions with PhilHealth, providing a consistent identifier for your records.
Actually, it's important to provide supporting documents. First-time registrants must attach a valid proof of identity. If you're updating your information, you should also include documents that establish relationships with dependents.
While some information may seem non-essential, completing the registration form is crucial for ensuring proper coverage. Missing details can lead to issues when you need to access healthcare services.
This is incorrect. All information must be written in uppercase letters. Consistency ensures that your information is read easily and reduces errors during processing.
This is a common misunderstanding. PhilHealth supports a variety of member types, including employed individuals, self-earning individuals, and even family drivers. Everyone qualifies for registration, regardless of employment status.
Key takeaways
Filling out and using the PhilHealth Registration form is a crucial step to access health benefits in the Philippines. Here are some key takeaways to streamline your registration process.
- Your PhilHealth Identification Number (PIN) is unique. This number stays with you for life, so always keep it handy.
- Your PIN is essential. Use it in all interactions with PhilHealth.
- Be aware of **updating and amendments**. If you need to change any information, check the appropriate box on the form and provide the necessary details.
- Read the instructions carefully. Understanding the guidelines at the back of the form can prevent mistakes.
- When filling out personal details, make sure to include your full mother’s maiden name and spouse's details if married.
- Be thorough with contact information. Ensure that you provide accurate permanent and mailing addresses, along with your contact numbers.
- Declare your dependents accurately. List all eligible dependents including spouses and children under 21 years.
- Remember to sign the form. Your signature confirms the accuracy of the information provided.
Browse Other Templates
Nyc Doe Hr Connect Phone Number - Shifting to electronic statements contributes to a more sustainable work environment.
Osha Fire Prevention Plan Template - Your Fire Safety Plan must demonstrate awareness of surrounding risks and resources.
Baseball Batting Order Strategy - Empowers managers to make informed decisions on the field.