Fill Out Your Print Va 21 4192 Form
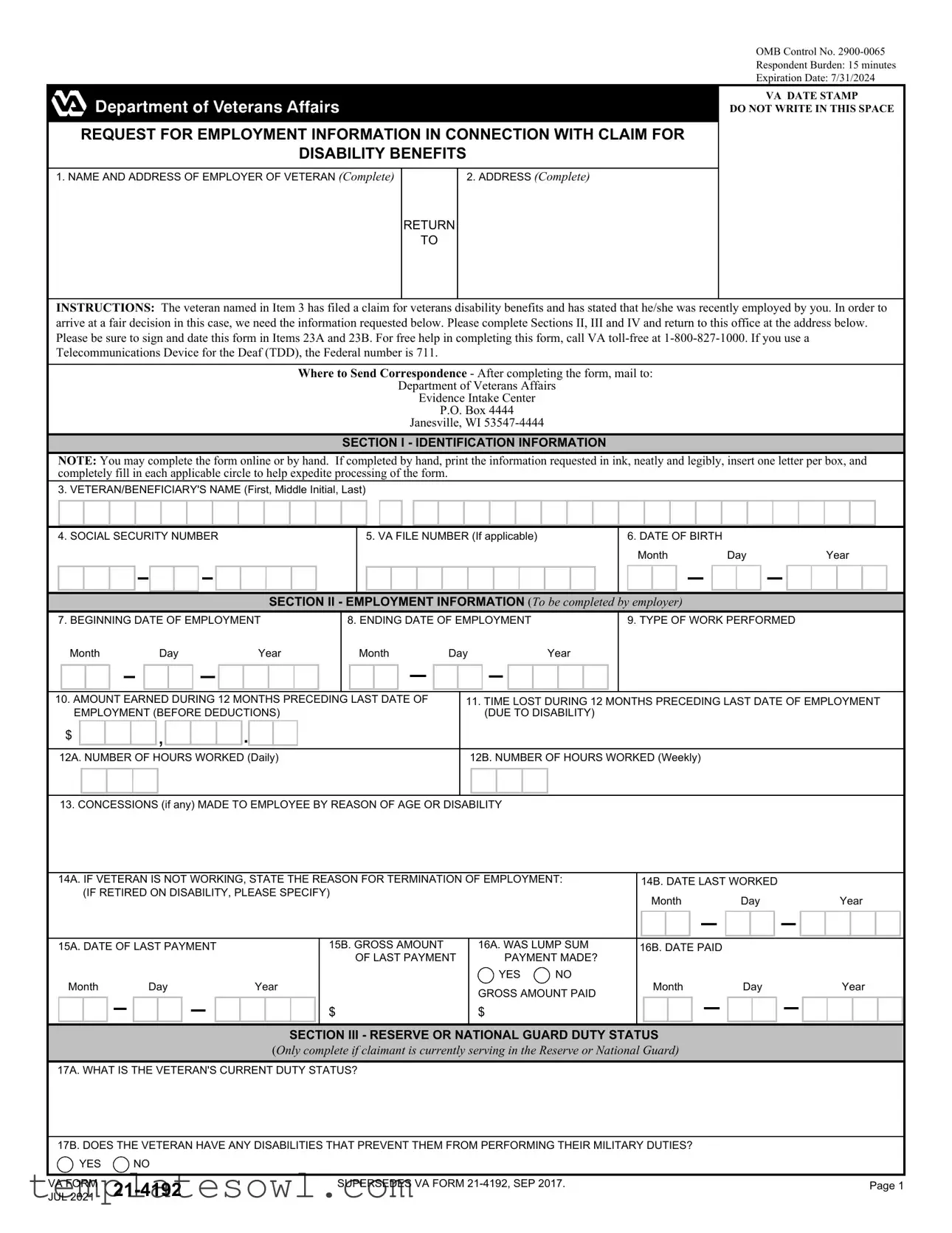
The Print VA 21-4192 form plays a crucial role in the process of applying for disability benefits for veterans. Specifically designed for employers, this form is a request for employment information related to a veteran's claim. It seeks to gather detailed data about the veteran's work history, including dates of employment, types of duties performed, earnings, and any disabilities that might have impacted their work. Furthermore, the document prompts employers to provide information regarding any sick or retirement benefits that the veteran may be entitled to due to their employment. Along with collecting pertinent employment details, it ensures the accuracy and integrity of the information submitted—holding employers accountable for their declarations. The form serves not only to facilitate fair decisions concerning benefit eligibility but also to maintain privacy and confidentiality, as mandated by federal law. With a respondent burden estimated at 15 minutes, the form is straightforward in its structure, allowing for completion either online or by hand, making the process accessible for all involved. This form must be returned to the VA with all required signatures, creating a vital link in the support and assistance provided to those who have courageously served the nation.
Print Va 21 4192 Example
OMB Control No.
Respondent Burden: 15 minutes
Expiration Date: 7/31/2024
VA DATE STAMP
DO NOT WRITE IN THIS SPACE
REQUEST FOR EMPLOYMENT INFORMATION IN CONNECTION WITH CLAIM FOR
DISABILITY BENEFITS
1. NAME AND ADDRESS OF EMPLOYER OF VETERAN (Complete) |
2. ADDRESS (Complete) |
RETURN
TO
INSTRUCTIONS: The veteran named in Item 3 has filed a claim for veterans disability benefits and has stated that he/she was recently employed by you. In order to arrive at a fair decision in this case, we need the information requested below. Please complete Sections II, III and IV and return to this office at the address below. Please be sure to sign and date this form in Items 23A and 23B. For free help in completing this form, call VA
Where to Send Correspondence - After completing the form, mail to:
Department of Veterans Affairs
Evidence Intake Center
P.O. Box 4444
Janesville, WI
SECTION I - IDENTIFICATION INFORMATION
NOTE: You may complete the form online or by hand. If completed by hand, print the information requested in ink, neatly and legibly, insert one letter per box, and completely fill in each applicable circle to help expedite processing of the form.
3. VETERAN/BENEFICIARY'S NAME (First, Middle Initial, Last)
4. SOCIAL SECURITY NUMBER
5. VA FILE NUMBER (If applicable)
6. DATE OF BIRTH
Month |
Day |
|
Year |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SECTION II - EMPLOYMENT INFORMATION (To be completed by employer)
7. BEGINNING DATE OF EMPLOYMENT |
8. ENDING DATE OF EMPLOYMENT |
|
|
|
|
|
9. TYPE OF WORK PERFORMED |
|||||||||||||||||||||||||||||||||
|
Month |
|
|
|
Day |
|
|
|
|
Year |
|
Month |
Day |
|
Year |
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10. AMOUNT EARNED DURING 12 MONTHS PRECEDING |
|
LAST DATE OF |
|
11. TIME LOST DURING 12 MONTHS PRECEDING LAST DATE OF EMPLOYMENT |
||||||||||||||||||||||||||||||||||||
|
EMPLOYMENT (BEFORE DEDUCTIONS) |
|
|
|
|
|
|
|
|
|
(DUE TO DISABILITY) |
|||||||||||||||||||||||||||||
$ |
|
|
|
|
|
|
, |
|
|
|
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
12A. NUMBER OF HOURS WORKED (Daily) |
|
|
|
|
|
|
|
12B. NUMBER OF HOURS WORKED (Weekly) |
||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
13. CONCESSIONS (if any) MADE TO EMPLOYEE BY REASON OF AGE OR DISABILITY
|
14A. IF VETERAN IS NOT WORKING, STATE THE REASON FOR TERMINATION OF EMPLOYMENT: |
|
14B. DATE LAST WORKED |
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
|
(IF RETIRED ON DISABILITY, PLEASE SPECIFY) |
|
|
|
Month |
Day |
|
|
|
|
Year |
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
15A. DATE OF LAST PAYMENT |
|
|
|
|
|
15B. GROSS AMOUNT |
16A. WAS LUMP SUM |
16B. DATE PAID |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OF LAST PAYMENT |
PAYMENT MADE? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Month |
|
|
Day |
|
Year |
|
YES |
NO |
|
Month |
Day |
|
|
|
|
Year |
||||||||||||||||||||
|
|
|
|
|
GROSS AMOUNT PAID |
|
|
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
$ |
$ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SECTION III - RESERVE OR NATIONAL GUARD DUTY STATUS (Only complete if claimant is currently serving in the Reserve or National Guard)
17A. WHAT IS THE VETERAN'S CURRENT DUTY STATUS?
17B. DOES THE VETERAN HAVE ANY DISABILITIES THAT PREVENT THEM FROM PERFORMING THEIR MILITARY DUTIES?
YES |
NO |
|
|
|
|
|
|
VA FORM |
SUPERSEDES VA FORM |
Page 1 |
|
JUL 2021 |
|
|
VETERAN'S SOCIAL SECURITY NO.
|
SECTION IV - INFORMATION ON BENEFIT ENTITLEMENT AND/OR PAYMENTS (To be completed by employer) |
18. IS VETERAN RECEIVING OR ENTITLED TO RECEIVE, AS A RESULT OF HIS/HER EMPLOYMENT WITH YOU, SICK, RETIREMENT OR OTHER BENEFITS? |
|
YES |
NO (If "Yes," complete Items 19 through 21C) |
19.TYPE OF BENEFIT
20.GROSS MONTHLY AMOUNT OF BENEFIT
$
,
.
21A. DATE BENEFIT BEGAN
21B. DATE FIRST PAYMENT ISSUED
21C. DATE BENEFIT WILL STOP (If known)
Month |
Day |
Year |
Month |
Day |
Year |
Month |
Day |
|
Year |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
22. REMARKS
I CERTIFY THAT the statements made in this form are true and complete to the best of my knowledge and belief.
23A. SIGNATURE OF EMPLOYER OR SUPERVISOR (Required)
23B. DATE SIGNED (MM/DD/YYYY)
PENALTY: The law provides severe penalties which include fine or imprisonment, or both, for the willful submission of any statement or evidence of a meterial fact, knowing it to be false, or for fraudulent acceptance of any payment to which you are not entitled.
PRIVACY ACT NOTICE: VA will not disclose information collected on this form to any source other than what has been authorized under the Privacy Act of 1974 or Title 38, Code of Federal Regulations 1.576 for routine uses (i.e., civil or criminal law enforcement, congressional communications, epidemiological or research studies, the collection of money owed to the United States, litigation in which the United States is a party or has an interest, the administration of VA programs and delivery of VA benefits, verification of identity and status, and personnel administration) as identified in the VA system of records, 58VA21/22/28, Compensation, Pension, Education and Vocational Rehabilitation and Employment Records - VA, published in the Federal Register. Your obligation to respond is voluntary. The requested information is considered relevant and necessary to determine maximum benefits under the law. The responses you submit are considered confidential (38 U. S.C. 5701). Information submitted is subject to verification through computer matching programs with other agencies.
RESPONDENT BURDEN: We need this information to determine eligibility for disability benefits based on unemployability (38 U.S.C. 1521). Title 38, United States Code, allows us to ask for this information. We estimate that you will need an average of 15 minutes to review the instructions, find the information, and complete this form. VA cannot conduct or sponsor a collection of information unless a valid OMB control number is displayed. You are not required to respond to a collection of information if this number is not displayed. Valid OMB control numbers can be located on the OMB Internet Page at www.reginfo.gov/public/do/PRAMain. If desired, you can call
VA FORM |
Page 2 |
Form Characteristics
| Fact Name | Description |
|---|---|
| Form Title | Request for Employment Information in Connection with Claim for Disability Benefits |
| OMB Control Number | 2900-0065 |
| Respondent Burden | 15 minutes to complete the form |
| Expiration Date | July 31, 2024 |
| Where to Send Completed Form | Department of Veterans Affairs, Evidence Intake Center, P.O. Box 4444, Janesville, WI 53547-4444 |
| Sections to Complete | Sections II, III, and IV must be completed by the employer |
| Privacy Act Compliance | Information collected is protected under the Privacy Act of 1974 |
| Legal Framework | Title 38, United States Code, governs the collection of information and disability benefits |
| Contact Information for Assistance | For help, call VA toll-free at 1-800-827-1000; TDD users can call 711 |
Guidelines on Utilizing Print Va 21 4192
Filling out the Print VA 21-4192 form requires careful attention to detail. This document gathers employment information related to a veteran's claim for disability benefits. After completing the form, it will be sent back to the Department of Veterans Affairs for processing.
- Obtain the Form: Access the Print VA 21-4192 form either online or through a printed copy.
- Identify the Employer: In Section I, enter the complete name and address of the veteran's employer in Items 1 and 2.
- Veteran's Information: Provide the veteran's full name, Social Security number, VA file number (if applicable), and date of birth in Items 3, 4, 5, and 6 respectively.
- Employment Dates: In Section II, fill in the veteran's beginning and ending dates of employment in Items 7 and 8.
- Job Details: Describe the type of work performed in Item 9 and list the total earnings for the 12 months leading up to the last date of employment in Item 10.
- Time Lost: Indicate any time lost due to disability in Item 11 and the number of hours worked daily and weekly in Items 12A and 12B.
- Concessions: Document any concessions made to the employee due to age or disability in Item 13.
- Employment Status: If the veteran is not currently working, provide the reason for termination in Item 14A and the last work date in Item 14B.
- Last Payment Information: Complete Items 15A and 15B with the date and gross amount of the last payment received.
- Lump Sum Payment: If applicable, answer whether a lump sum payment was made in Items 16A and 16B, and provide the relevant dates.
- Current Duty Status: If the veteran is in the Reserve or National Guard, fill in Item 17 with their current duty status and indicate whether they have disabilities in Item 17B.
- Benefit Information: In Section IV, provide details about any sick, retirement, or other benefits the veteran may be receiving in Items 18 through 21C.
- Additional Remarks: Enter any additional remarks in Item 22.
- Certification: Sign and date the form in Items 23A and 23B to certify the accuracy of the information provided.
After completing the form, ensure it is free of errors. The completed form should be mailed to the address provided by the Department of Veterans Affairs. Retaining a copy for your records is advisable.
What You Should Know About This Form
What is the purpose of the Print VA 21-4192 form?
The Print VA 21-4192 form is used to gather employment information from an employer regarding a veteran who has filed a claim for disability benefits. This information is crucial for the Department of Veterans Affairs (VA) to assess the veteran's eligibility for benefits. The form specifically focuses on aspects like the duration of employment, type of work performed, earnings, and any disabilities that might impact the veteran's ability to work.
How should employers fill out the Print VA 21-4192 form?
Employers should complete Sections II, III, and IV of the form. They need to provide accurate details such as the veteran's employment start and end dates, the nature of their job duties, earnings in the last 12 months, and any time lost due to disability. The form can be filled out either online or by hand. If completing by hand, it's essential to use ink and ensure legibility. Employers are required to sign and date the form in the designated areas before sending it back to the VA.
Where should the completed Print VA 21-4192 form be sent?
Once the form is completed, employers must mail it to the Department of Veterans Affairs Evidence Intake Center at P.O. Box 4444, Janesville, WI 53547-4444. It's important to ensure that the information is accurate and complete to avoid delays in processing the veteran’s claim.
What should I do if I need help filling out the form?
If you need assistance with completing the Print VA 21-4192 form, you can contact the VA for help. Call the VA toll-free at 1-800-827-1000 for free support. For those using a Telecommunications Device for the Deaf (TDD), you can reach them at the Federal number 711. They can guide you through the process and answer any specific questions you may have regarding the form.
Common mistakes
Filling out the Print VA 21-4192 form can be straightforward, but many people make common mistakes. Addressing these issues can expedite processing and ensure accuracy. One prevalent error occurs in providing incomplete or inaccurate employer information. It’s crucial for employers to thoroughly fill in the sections related to their name and address. Missing details here can delay the claim.
Another mistake often seen is neglecting to sign and date the form in the specified places. Items 23A and 23B require both the signature of the employer or supervisor and the date of signing. Without these essential components, the form may be considered invalid and returned for correction.
Inaccurate employment dates are also a frequent oversight. The starting and ending employment dates must be precisely noted. Errors in these sections can lead to complications in verifying the veteran's employment status and benefits entitlement.
Providing incorrect financial figures is a significant error. Item 10 asks for the total amount earned during the last 12 months prior to the last date of employment. This figure should be filled out correctly, without deductions. Misreporting income affects benefit calculations and may result in serious ramifications.
People sometimes fail to complete Section III relating to reserve or national guard duty. If applicable, this section must be checked and filled. Incomplete information can lead to misunderstandings about the veteran’s current military responsibilities.
Omissions in Section IV about benefit entitlements are also common. If the veteran is receiving sick pay, retirement benefits, or other forms of compensation from the employer, this must be noted. Failure to provide such details can obscure the full picture of the veteran's financial situation.
Finally, mistakes in itemizing benefits information can also cause issues. It’s essential to clearly specify the type of benefit in Item 19, along with the gross monthly amount in Item 20. Without clear and correct data, the processing of the claim may be delayed or hindered.
Documents used along the form
When navigating the process of claiming veterans’ disability benefits, several forms accompany the Print VA 21-4192 form. Each of these documents serves a specific purpose in gathering essential information needed for a strong claim. Understanding what they are and how they relate to your claim can make the process smoother and more efficient.
- VA Form 21-526EZ: This form is used to apply for disability compensation and related benefits. It captures detailed information about your service, medical conditions, and how those conditions affect your daily life.
- VA Form 21-534EZ: Widows and dependents can use this form to apply for Dependency and Indemnity Compensation (DIC) and survivorship benefits. This document helps establish a connection between the veteran’s service and the survivor’s need for assistance.
- VA Form 21-4142: This authorization form allows the VA to obtain medical records from health care providers. Accessing your medical history can provide critical support for your disability claim, ensuring that all relevant information is considered.
- VA Form 21-4142a: A supplement to the previous form, this document requests information about private medical treatment you have received. It’s crucial for gathering additional evidence that backs up your claim.
- VA Form 27-2008: Used for veterans seeking assistance in appealing a decision related to their disability compensation, this form helps outline the specifics of the appeal, ensuring that all pertinent issues are presented clearly.
Each of these forms plays an integral role in supporting your claim for veterans’ benefits. Be sure to provide accurate and complete information when filling them out. This will not only aid in expediting the processing of your claim but also improve your chances of a favorable outcome.
Similar forms
- VA Form 21-526EZ: This form is also used in the claims process for veterans seeking disability benefits. Similar to the Print VA 21-4192, it collects critical information about the veteran’s service, condition, and employment history to assess eligibility.
- VA Form 21-8779: Known as the "Veteran's Application for Increased Compensation based on Unemployability," this document is required when veterans claim they cannot work due to service-related disabilities. Like the Print VA 21-4192, it examines the individual's work history and income.
- VA Form 21-4142: This is used to authorize the release of information from healthcare providers. It parallels the Print VA 21-4192 in seeking crucial information that supports a veteran's claim for benefits, though it focuses on medical records instead of employment details.
- VA Form 21-0845: This form is used to allow the VA to share information with a designated individual. It serves as a means of communication about claims, similar in purpose to how the Print VA 21-4192 communicates employment details but broader in scope.
- VA Form 21-0966: Known as the "Intent to File a Claim for Compensation and/or Pension," this form signals a veteran’s intent to seek benefits. It sets the stage for subsequent forms like the Print VA 21-4192, which requires detailed information to process the specific claim.
- VA Form 21-527EZ: This form is for veterans applying for pension benefits. It shares similarities with the Print VA 21-4192 in that both require comprehensive information regarding the applicant’s finances and previous employment to establish eligibility for benefits.
Dos and Don'ts
When completing the Print VA 21-4192 form, following certain guidelines can help ensure accuracy and compliance. Here are some key dos and don'ts:
- Do print neatly using ink if you are filling out the form by hand. This helps prevent any misinterpretation of your information.
- Do complete all sections fully. Missing information can lead to delays in processing your request.
- Do double-check your entries for accuracy, especially the veteran's name and social security number, as these details are critical.
- Do sign and date the form in Items 23A and 23B to validate your submission.
- Don’t use pencil or erasable ink. Changes may not be clearly visible, which can complicate your application.
- Don’t skip the privacy notice or any instructions provided. They are essential for understanding how your information will be used.
Following these guidelines will help facilitate a smoother process in evaluating disability benefits claims.
Misconceptions
Misconception 1: The Print VA 21-4192 form is only for veterans seeking job-related benefits.
This form is actually used to gather employment information for veterans filing disability claims. It addresses various situations, including work history and benefits related to employment.
Misconception 2: Completing the form is optional for employers.
Employers must complete and return the form once notified by a veteran. This information is critical for the VA to assess the veteran's disability claim fairly.
Misconception 3: The form requires a lot of complex legal knowledge to fill out.
In fact, the VA provides clear instructions, and the information requested is straightforward. Most employers can complete it without legal assistance.
Misconception 4: The VA does not protect the confidentiality of the information submitted.
The VA adheres to strict privacy regulations. Information collected is confidential and used solely for determining eligibility for benefits.
Misconception 5: The form can be submitted electronically without any concerns.
While the form can be completed online, it must be printed and mailed if the employer is submitting it physically. Ensure you follow the specific submission guidelines provided.
Misconception 6: Filing this form guarantees the veteran will receive benefits.
Completing the Print VA 21-4192 form does not guarantee approval of benefits. The VA reviews all submitted information before making a decision on the claim.
Key takeaways
When filling out and using the Print VA Form 21-4192, it is essential to keep the following key points in mind:
- Purpose of the Form: This form is primarily used to collect employment information from the employer of a veteran filing for disability benefits. Accurate completion is crucial for the veteran's claim to be fairly assessed.
- Identification Section: The first section requires detailed identification information about both the veteran and the employer. Make sure to provide complete and clear information to avoid any processing delays.
- Employer’s Responsibilities: Employers must fill out sections concerning employment dates, job performance, and any disability-related accommodations. These details help the VA understand the veteran's work history and current status.
- Signature Requirement: The form requires the signature of the employer or supervisor. This assures that all submitted information is certified as true and complete, which is important for legal and ethical accountability.
- Submission Instructions: After completing the form, send it to the Department of Veterans Affairs Evidence Intake Center in Janesville, Wisconsin. Ensure you follow the guidelines to facilitate a smooth process for the veteran's claim.
By understanding these key takeaways, those involved can better navigate the process of using the Print VA Form 21-4192, ensuring that veterans receive the benefits they deserve.
Browse Other Templates
Organization Report,Census Business Listing Form,Establishment Data Collection,Corporate Information Survey,Business Operations Outline,Economic Activity Report,U.S. Business Establishment Form,Corporate Data Submission,Ownership and Control Document - Businesses must report their establishment information for the Census Bureau using this form.
Maryland Rental Application - Enter your Social Security number for identification purposes.
How to Set Up Direct Deposit - Seek assistance from bank representatives if you need help filling out the form.