Fill Out Your Remistart Enrollment Form
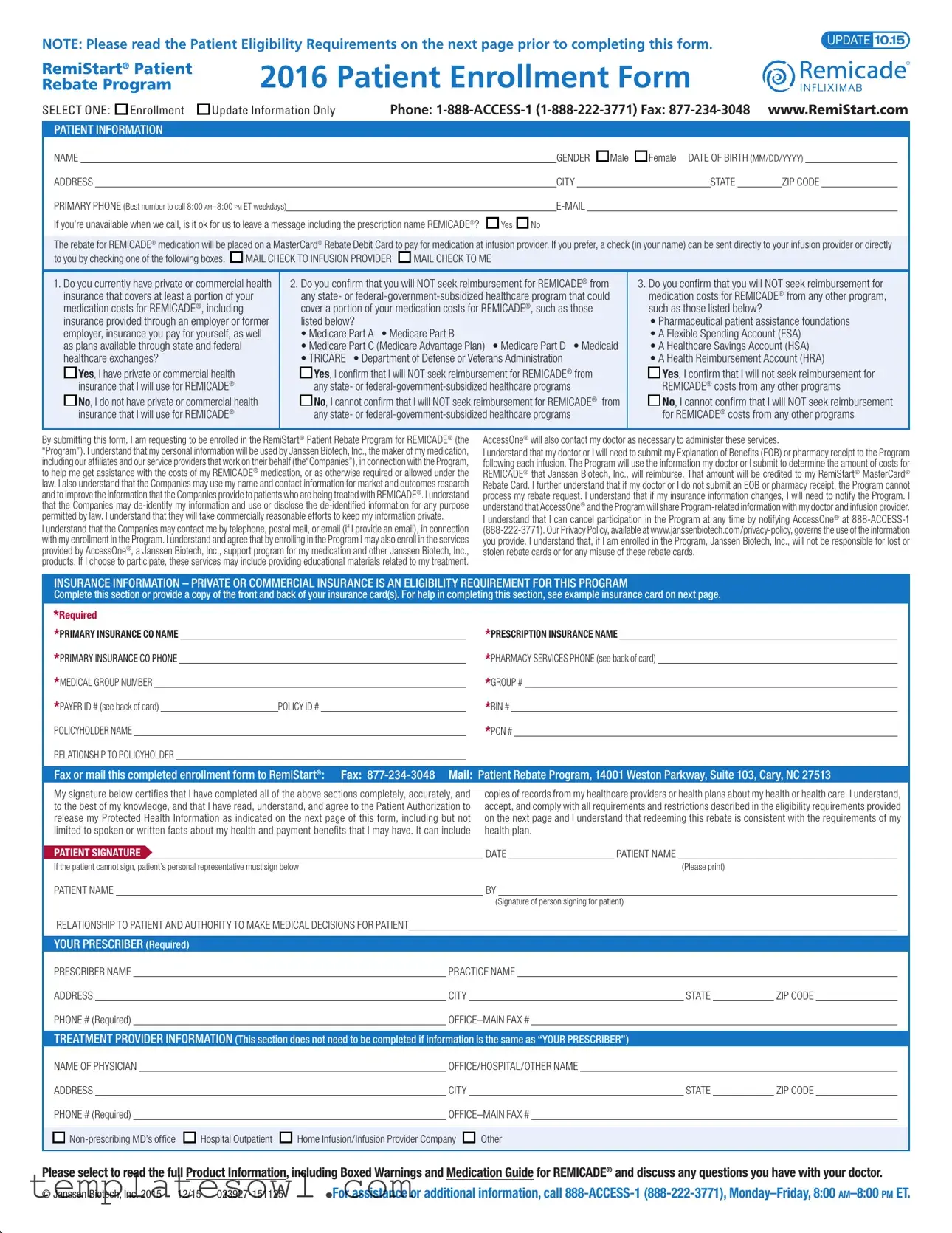
The RemiStart Enrollment form serves as a crucial gateway for patients seeking financial assistance through the RemiStart® Patient Rebate Program for REMICADE®. Before filling out this form, patients are advised to review the Patient Eligibility Requirements, which outline necessary conditions for participation. The form collects essential patient information, including name, date of birth, contact details, and health insurance specifics, while also prompting participants to specify their preferred method for receiving rebates—either through a MasterCard® Rebate Debit Card or a direct check sent to their infusion provider or themselves. Importantly, the form ensures that individuals have private or commercial health insurance for REMICADE®, and it requires patients to confirm that they will not seek reimbursement from government-subsidized programs like Medicare or Medicaid. By signing the form, patients agree to share relevant health information with Janssen Biotech, Inc., the medication manufacturer, for the purpose of facilitating program assistance. They also grant permission for their data to be used in market research, with a promise that their information will be kept private. The enrollment process is straightforward, requiring submission of the completed form via fax or mail, and emphasizes that participation can be cancelled at any time should circumstances change.
Remistart Enrollment Example
NOTE: Please read the Patient Eligibility Requirements on the next page prior to completing this form. |
UPDATE 10.15 |
|
RemiStart® Patient Rebate Program
2016 Patient Enrollment Form
SELECT ONE: Enrollment |
Update Information Only |
Phone: |
www.RemiStart.com |
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
PATIENT INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
NAME |
|
|
|
|
|
|
|
|
GENDER Male |
Female DATE OF BIRTH (MM/DD/YYYY) |
|
|
||||||||
ADDRESS |
|
|
|
|
|
|
|
|
CITY |
|
|
STATE |
|
ZIP CODE |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
PRIMARY PHONE (Best number to call 8:00 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
||||||||||
If you’re unavailable when we call, is it ok for us to leave a message including the prescription name REMICADE®? |
|
Yes |
|
No |
|
|
|
|
|
|
|
|
||||||||
The rebate for REMICADE® medication will be placed on a MasterCard® Rebate Debit Card to pay for medication at infusion provider. If you prefer, a check (in your name) can be sent directly to your infusion provider or directly
to you by checking one of the following boxes.  MAIL CHECK TO INFUSION PROVIDER
MAIL CHECK TO INFUSION PROVIDER  MAIL CHECK TO ME
MAIL CHECK TO ME
1.Do you currently have private or commercial health insurance that covers at least a portion of your medication costs for REMICADE®, including insurance provided through an employer or former employer, insurance you pay for yourself, as well as plans available through state and federal healthcare exchanges?
 Yes, I have private or commercial health insurance that I will use for REMICADE®
Yes, I have private or commercial health insurance that I will use for REMICADE®
 No, I do not have private or commercial health insurance that I will use for REMICADE®
No, I do not have private or commercial health insurance that I will use for REMICADE®
2.Do you confirm that you will NOT seek reimbursement for REMICADE® from any state- or
• Medicare Part A • Medicare Part B
• Medicare Part C (Medicare Advantage Plan) • Medicare Part D • Medicaid
• TRICARE • Department of Defense or Veterans Administration

 Yes, I confirm that I will NOT seek reimbursement for REMICADE® from any state- or
Yes, I confirm that I will NOT seek reimbursement for REMICADE® from any state- or

 No, I cannot confirm that I will NOT seek reimbursement for REMICADE® from any state- or
No, I cannot confirm that I will NOT seek reimbursement for REMICADE® from any state- or
3.Do you confirm that you will NOT seek reimbursement for medication costs for REMICADE® from any other program, such as those listed below?
•Pharmaceutical patient assistance foundations
•A Flexible Spending Account (FSA)
•A Healthcare Savings Account (HSA)
•A Health Reimbursement Account (HRA)

 Yes, I confirm that I will not seek reimbursement for REMICADE® costs from any other programs
Yes, I confirm that I will not seek reimbursement for REMICADE® costs from any other programs

 No, I cannot confirm that I will NOT seek reimbursement for REMICADE® costs from any other programs
No, I cannot confirm that I will NOT seek reimbursement for REMICADE® costs from any other programs
By submitting this form, I am requesting to be enrolled in the RemiStart® Patient Rebate Program for REMICADE® (the “Program”). I understand that my personal information will be used by Janssen Biotech, Inc., the maker of my medication, including our affiliates and our service providers that work on their behalf (the“Companies”), in connection with the Program, to help me get assistance with the costs of my REMICADE® medication, or as otherwise required or allowed under the law. I also understand that the Companies may use my name and contact information for market and outcomes research and to improve the information that the Companies provide to patients who are being treated with REMICADE®. I understand that the Companies may
I understand that the Companies may contact me by telephone, postal mail, or email (if I provide an email), in connection with my enrollment in the Program. I understand and agree that by enrolling in the Program I may also enroll in the services provided by AccessOne®, a Janssen Biotech, Inc., support program for my medication and other Janssen Biotech, Inc., products. If I choose to participate, these services may include providing educational materials related to my treatment.
AccessOne® will also contact my doctor as necessary to administer these services.
I understand that my doctor or I will need to submit my Explanation of Benefits (EOB) or pharmacy receipt to the Program following each infusion. The Program will use the information my doctor or I submit to determine the amount of costs for REMICADE® that Janssen Biotech, Inc., will reimburse. That amount will be credited to my RemiStart® MasterCard® Rebate Card. I further understand that if my doctor or I do not submit an EOB or pharmacy receipt, the Program cannot process my rebate request. I understand that if my insurance information changes, I will need to notify the Program. I understand that AccessOne® and the Program will share
I understand that I can cancel participation in the Program at any time by notifying AccessOne® at
INSURANCE INFORMATION – PRIVATE OR COMMERCIAL INSURANCE IS AN ELIGIBILITY REQUIREMENT FOR THIS PROGRAM
Complete this section or provide a copy of the front and back of your insurance card(s). For help in completing this section, see example insurance card on next page.
*Required |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
*PRIMARY INSURANCE CO NAME |
|
|
|
|
|
|
|
*PRESCRIPTION INSURANCE NAME |
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
*PRIMARY INSURANCE CO PHONE |
|
|
|
|
|
|
|
*PHARMACY SERVICES PHONE (see back of card) |
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
*MEDICAL GROUP NUMBER |
|
|
|
|
|
|
|
|
|
*GROUP # |
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
*PAYER ID # (see back of card) |
|
|
POLICY ID # |
|
|
|
|
*BIN # |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
POLICYHOLDER NAME |
|
|
|
|
|
|
|
|
*PCN # |
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
RELATIONSHIP TO POLICYHOLDER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
||||||||||||||||||||||||||||||||
Fax or mail this completed enrollment form to RemiStart®: Fax: |
Mail: Patient Rebate Program, 14001 Weston Parkway, Suite 103, Cary, NC 27513 |
||||||||||||||||||||||||||||||||
My signature below certifies that I have completed all of the above sections completely, accurately, and |
copies of records from my healthcare providers or health plans about my health or health care. I understand, |
||||||||||||||||||||||||||||||||
to the best of my knowledge, and that I have read, understand, and agree to the Patient Authorization to |
accept, and comply with all requirements and restrictions described in the eligibility requirements provided |
||||||||||||||||||||||||||||||||
release my Protected Health Information as indicated on the next page of this form, including but not |
on the next page and I understand that redeeming this rebate is consistent with the requirements of my |
||||||||||||||||||||||||||||||||
limited to spoken or written facts about my health and payment benefits that I may have. It can include |
health plan. |
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
PATIENT SIGNATURE |
|
|
|
|
|
|
|
DATE |
|
PATIENT NAME |
|
|
|
|
|||||||||||||||||||
If the patient cannot sign, patient’s personal representative must sign below |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(Please print) |
|
|
|
|||||||||||||||
PATIENT NAME |
|
|
|
|
|
|
|
BY |
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(Signature of person signing for patient) |
|
|
|
|||||||||||||
RELATIONSHIP TO PATIENT AND AUTHORITY TO MAKE MEDICAL DECISIONS FOR PATIENT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
YOUR PRESCRIBER (Required) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
PRESCRIBER NAME |
|
|
|
|
PRACTICE NAME |
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
ADDRESS |
|
|
|
|
CITY |
|
|
|
|
|
|
|
|
|
|
|
|
|
STATE |
|
ZIP CODE |
|
|
||||||||||
PHONE # (Required) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
TREATMENT PROVIDER INFORMATION (This section does not need to be completed if information is the same as “YOUR PRESCRIBER”)
NAME OF PHYSICIAN |
|
OFFICE/HOSPITAL/OTHER NAME |
|
|
|
|
|
||||
ADDRESS |
|
|
CITY |
|
|
STATE |
|
ZIP CODE |
|
||
PHONE # (Required) |
|
|
|
|
|
|
|
|
|||
Hospital Outpatient
Home Infusion/Infusion Provider Company
Other
Please select to read the full Product Information, including Boxed Warnings and Medication Guide for REMICADE® and discuss any questions you have with your doctor.
© Janssen Biotech, Inc. 2015 12/15 |
For assistance or additional information, call |
Patient Authorization (PA)
Patients must read this and sign the acknowledgment on the previous page before they can participate in the Program.
My signature on the previous page of this form confirms that I allow my doctor(s), any other healthcare providers, specialty pharmacy providers, and my health plan or insurers to share medical information relating to my use or potential use of REMICADE® (infliximab) with Janssen Biotech, Inc., including our affiliates and our service providers that work on their behalf, in connection with the Program (the ”Companies”).
The Companies administer AccessOne® and RemiStart® (the “Program”) for Janssen Biotech, Inc., maker of REMICADE®.
This information can include spoken or written facts about my health and payment benefits I may have. It may include copies of records from my healthcare providers or health plans about my health or health care.
The Companies may use and share this information to help find alternate funding sources for REMICADE®, and perform other related services. The Companies may also share my information with other related parties of this program or as otherwise set forth above.
The Companies will use and share this information to see if I qualify for the Programs and to run the Programs. In addition, the Companies may use and share my information to refer me to other programs, foundations, or alternate sources of funding or coverage that may be available to provide assistance to me with costs of my medication. Program management employees of the Companies may also see my information, but they may use it only in connection with the Program, to help me get assistance with the costs of my medication, or as otherwise required or allowed under the law. I understand that they will make every effort to keep my information private, but if it is accidentally shared with an associated party, federal privacy laws will not protect it.
This Authorization will last until I am no longer participating in the Program. If I change my mind, I can inform my healthcare providers and my insurers in writing that I do not want them to share any information with AccessOne® and RemiStart® (Janssen Biotech, Inc., including our affiliates and our service providers that work on their behalf, in connection with the Program), but will not change any information shared before I notified them of my desire to discontinue. I know that I have a right to see or copy the information my healthcare providers or insurers have given to the Companies.
I understand that I am not required to sign this form on the previous page. My choice about whether to sign this form will not change the way my healthcare providers or insurers treat me. If I refuse to sign on the previous page of this form, I know that this means I will not be able to receive assistance from the Program.
Patient Eligibility Requirements for the RemiStart® Program
RemiStart® is available to patients who:
•Are beginning or are currently receiving treatment with REMICADE®
•Currently have private or commercial health insurance that covers a portion of the medication costs for REMICADE®
Other Restrictions:
•This program is only available to individuals using private or commercial health insurance to cover a portion of their medication costs, including plans available through state and federal health care exchanges. This program is not available to individuals who use any state- or
•This offer may not be combined with any other coupon, discount, prescription savings card, free trial, or other offer
•The selling, purchasing, trading, or counterfeiting of this rebate card is prohibited
•Offer good only in the U.S. and Puerto Rico. Janssen Biotech, Inc. reserves the right to rescind, revoke, or amend this offer without notice at any time. Void where prohibited, taxed, or otherwise restricted by law
•Offer for new enrollment expires December 31, 2016. For Massachusetts residents only, this offer is subject to change per state legislation
•This program is not retroactive
How can I enroll?
1.Review the eligibility requirements above. Complete and sign the first page of this form.
2.Fax or mail this enrollment form to RemiStart® Fax:
Mail: Patient Rebate Program, 14001 Weston Parkway, Suite 103, Cary, NC 27513
NOTE: Your signature on the first page of this form certifies:
•That you understand, accept, and comply with all requirements and restrictions described above, and that redeeming this rebate is consistent with the requirements of your health plan.
•That you have read, understand, and agree to the Patient Authorization to release your Protected Health Information as indicated above, including but not limited to spoken or written facts about your health and payment benefits you may have. It can include copies of records from your healthcare providers or health plans about your health or health care.
Example Insurance Card
XYZ Insurance Company |
Plan Type |
||||||
|
|
|
|
|
|
||
XYX Company |
|
|
|
||||
Primary Insurance Information |
|||||||
GROUP |
123456 |
|
|
||||
|
|
||||||
PAYER ID |
612345 |
|
|
|
|
|
|
ID |
Submit All Claims to |
||||||
Name |
John Doe |
PO Box 123 |
|
|
|||
|
|
|
|
Cary, NC 27513 |
|||
COPAY: |
|
|
|
Payer ID 61234 |
|||
RXBIN 600123 RXPCN 00612345 |
|
|
|
||||
RXGROUP 00654321 |
|
Pharmacists Call |
|||||
RXID |
|
|
|
|
|||
|
|
|
|
|
|
|
|
The BIN will always be 6 numeric digits.
The PCN could contain numbers and letters. If your pharmacy insurance card does not have a PCN number, leave the field blank.
Please select to read the full Prescribing Information, including Boxed Warnings and Medication Guide for REMICADE®, and discuss any questions you have with your doctor.
Janssen Biotech, Inc., is not liable for unintended or unauthorized use of the RemiStart® Patient Rebate Program MasterCard® Rebate Card if it is lost or stolen. This card is issued by MetaBank®, Member FDIC, pursuant to license by MasterCard International. MasterCard is a registered trademark of MasterCard International. RemiStart® is not a MetaBank product and is not endorsed by them.
© Janssen Biotech, Inc. 2015 12/15 |
Form Characteristics
| Fact Name | Description |
|---|---|
| Enrollment Choices | Patients can select between enrolling in the program or providing an update to existing information. |
| Eligibility Requirements | Participants must have private or commercial health insurance; other funding sources like Medicare or Medicaid disqualify them. |
| Reimbursement Confirmation | Applicants must confirm they will not seek reimbursement from state or federal government programs for REMICADE® costs. |
| Communication Consent | By submitting the form, applicants consent to be contacted by the program via phone, email, or postal mail. |
| Privacy Policy | Personal information will be handled according to Janssen Biotech's Privacy Policy, available on their website. |
| Program Restrictions | This program is not retroactive and cannot be combined with other offers or discounts. |
Guidelines on Utilizing Remistart Enrollment
Filling out the RemiStart Enrollment form is an essential step for patients who are ready to start their journey with the RemiStart® Patient Rebate Program. This form collects vital information that will enable the processing of rebate requests and ensure you receive the necessary assistance with medication costs. Following the steps provided below will help streamline the process and minimize any potential delays.
- Read the Patient Eligibility Requirements. Before you begin, ensure you are eligible to enroll in the program.
- Select your enrollment type. Choose whether you are enrolling for the first time or updating your information.
- Fill out your patient information. Provide your name, gender, date of birth, and address details, including city, state, and zip code.
- Provide your primary phone number. This should be the best number for contact between 8:00 AM and 8:00 PM ET on weekdays.
- Enter your email address. It is optional, but providing it can facilitate communication.
- Indicate your message preferences. State whether it is okay for them to leave a message regarding the prescription name REMICADE® if you are unavailable.
- Choose a payment method. Decide whether you prefer to receive a rebate payment via a MasterCard® Rebate Debit Card or a check sent to you or your infusion provider.
- Answer insurance-related questions. Confirm whether you currently have private or commercial health insurance, and respond to questions concerning your intent to seek reimbursement from various programs.
- Review your understanding of the program. Acknowledge that you understand how your information will be used and what your responsibilities are within the program.
- Complete the insurance information section. Provide details from your primary insurance card, including insurance company names, phone numbers, and policy IDs.
- Sign the form. Certify that all information is complete and accurate by signing and dating the document.
- Submit the enrollment form. Fax it to 877-234-3048 or mail it to the address provided.
By completing these steps, you will have submitted your enrollment application successfully. Stay tuned for further communication regarding your enrollment status and the next stages related to your medication assistance.
What You Should Know About This Form
1. What is the RemiStart Enrollment form used for?
The RemiStart Enrollment form is utilized for enrolling patients in the RemiStart® Patient Rebate Program for REMICADE®. This program offers financial assistance to individuals who have private or commercial health insurance that covers the costs of their REMICADE® medication. The form must be completed to receive rebates or checks for medication costs.
2. Who is eligible to enroll in the program?
Patients who are beginning or currently receiving treatment with REMICADE® and have private or commercial health insurance that contributes to their medication costs are eligible. However, individuals using government-subsidized healthcare programs, such as Medicare or Medicaid, cannot participate.
3. How do I submit the completed enrollment form?
You can submit the finalized enrollment form either by faxing it to 877-234-3048 or by mailing it to the address provided: Patient Rebate Program, 14001 Weston Parkway, Suite 103, Cary, NC 27513. Ensure that your form is signed correctly to facilitate processing.
4. What information is needed on the enrollment form?
The form requires personal information such as your name, gender, date of birth, contact details, and insurance information. You will also need to confirm your understanding and acceptance of the eligibility requirements and patient authorization regarding the use of your health information.
5. Can I receive both a rebate card and a check?
Yes, you can choose to receive your rebate for REMICADE® either on a MasterCard® Rebate Debit Card or via a check directly mailed to you or your infusion provider. This selection must be made on the enrollment form.
6. What happens if I change my insurance?
If your insurance information changes, it is your responsibility to inform the RemiStart program. Updating your information ensures you can continue receiving assistance without interruptions or issues with future rebate claims.
7. Can I opt out of the RemiStart program at any time?
Yes, participation in the program is voluntary, and you may withdraw at any time. To cancel your participation, notify AccessOne® by calling 888-ACCESS-1 (888-222-3771). Ensure you do this to avoid any further processing of your information.
8. How is my personal information used and protected?
Your personal information is used solely for the purposes of the RemiStart program, which includes assisting with your REMICADE® costs. While the company will take measures to protect your information, there is always a risk in sharing data. You have the right to see the information shared and may withdraw your consent to share said information with AccessOne® at any time.
Common mistakes
Filling out the RemiStart Enrollment form can be a straightforward process, but common mistakes can lead to delays or problems with your application. One frequent error is forgetting to read the Patient Eligibility Requirements before starting the form. This critical step ensures that applicants fully understand the qualifications for the program, helping to avoid unnecessary complications later in the process.
Another common mistake occurs when providing personal information. Many people accidentally omit their date of birth, gender, or contact details. It is important to remember that this information must be complete for the program to assess eligibility properly. Leaving out any of these sections can lead to rejection of the application or delays in processing.
Additionally, individuals sometimes fail to select the appropriate enrollment option at the beginning of the form. There are specific sections for enrollment, updates, or information requests, and selecting the wrong option could send applicants on the wrong path, leading to further confusion.
An equally significant issue arises when individuals do not specify their insurance information completely. It is crucial to provide accurate details about private or commercial insurance, as this is a requirement for enrollment. Insufficient or incorrect insurance data might result in ineligibility for the rebate program.
Moreover, some applicants neglect to confirm whether they will seek reimbursement from state or federal healthcare programs. The form explicitly asks for this confirmation. A "No" answer is essential, as stipulating otherwise may disqualify an applicant from the program.
Submitting the form without reviewing it thoroughly is another mistake often made. Typos or unclear information can impede the processing of applications, leading to additional follow-up requests and delays. Taking a few moments to double-check each field is advisable to prevent these setbacks.
Furthermore, people sometimes overlook the requirement for a physician’s signature, which is necessary for program participation. Without this critical endorsement, applications may be deemed incomplete and subsequently rejected.
Marking the wrong method of receiving funds can also create issues. Applicants need to specify whether they prefer to receive the rebate via a debit card or check. Failing to make this selection can lead to complications in receiving the rebate.
In addition, individuals can forget to update their information if their insurance or contact details change. Many forget this important step after their initial enrollment. Notifying the program of changes ensures ongoing eligibility for the rebate.
Lastly, leaving blank fields in the signature section may lead to automatic rejection since all signatures must correspond to the patient’s acknowledgement of the information shared. Ensuring that every required area of the form is filled out correctly is vital for a smooth enrollment process.
Documents used along the form
The RemiStart Enrollment Form is an important document for patients looking to participate in the RemiStart Patient Rebate Program for REMICADE®. However, to navigate the enrollment process smoothly, several other forms and documents may also be required. Here’s a concise overview of those documents to assist in completing your enrollment.
- Patient Authorization Form: This form grants permission for healthcare providers to share your medical information with Janssen Biotech, Inc. It is essential for participation in the program.
- Proof of Insurance: This document includes a copy of your health insurance card. It demonstrates that you have private or commercial insurance that covers medication costs for REMICADE®.
- Explanation of Benefits (EOB): After each treatment, an EOB from your insurer shows the amount covered for REMICADE®. This is crucial for rebate requests under the program.
- Prescriber Information Form: This form provides details about your prescribing physician. It's required to ensure that your treatment is properly documented and managed.
- Infusion Provider Information: Document detailing where you will receive your REMICADE® infusions. This helps the program coordinate the rebates with your treatment facility.
- Privacy Policy Acknowledgment: A statement confirming that you’ve read and understood the privacy policy related to the use of your personal information in the program.
- Patient Eligibility Requirements: You must read this to ensure that you meet all guidelines necessary for enrollment in the rebate program.
- Medical History Form: Some programs may require a brief medical history to assess qualifications for the REMICADE® treatment.
- Financial Assistance Request: If applicable, this form may help you apply for additional financial support if your insurance provides insufficient coverage.
- Contact Information Update: A form to report any changes in your contact details or insurance coverage after enrollment.
Having these documents ready can streamline your enrollment in the RemiStart Patient Rebate Program, ensuring you receive the support needed for your REMICADE® treatment. For any questions, feel free to reach out directly to the program hotline or your healthcare provider.
Similar forms
The RemiStart Enrollment form shares similarities with several other documents commonly used in healthcare and insurance contexts. Below is a list outlining five such documents and their respective comparisons.
- Patient Registration Form: Like the RemiStart Enrollment form, the patient registration form collects essential personal and contact information, including the patient's name, address, and phone number. Both forms aim to facilitate the patient's access to necessary medical services or programs.
- Insurance Claim Form: This form is similar in its need for patient insurance details, such as policyholder information and coverage specifics. They both serve to initiate processes for reimbursement or assistance related to healthcare services.
- Medication Reimbursement Request Form: This document is closely aligned with the RemiStart Enrollment form, as it requires information about the patient's treatment and the prescribed medication. Each form functions to request financial assistance or reimbursement related to healthcare expenses.
- HIPAA Authorization Form: Both forms emphasize the importance of patient consent regarding the release of personal health information. The HIPAA authorization form details what information can be shared and with whom, paralleling the RemiStart form's requirement for patient consent related to data use.
- Patient Assistance Program Application: Similar to the RemiStart Enrollment form, this application assists patients in obtaining medications at reduced costs. Both documents screen for eligibility requirements and document patient insurance information while facilitating cost assistance programs.
Dos and Don'ts
When completing the RemiStart Enrollment form, consider the following important points:
- Do read the Patient Eligibility Requirements carefully before starting the form.
- Do provide accurate and complete personal and insurance information to avoid delays.
- Do confirm that you will not seek reimbursement from any government-subsidized healthcare programs.
- Do sign and date the form after reviewing all information provided.
- Do contact the provided number if you have any questions before submitting the form.
However, there are also some things to avoid:
- Don’t leave any required fields blank; incomplete forms could lead to processing issues.
- Don’t forget to provide your doctor’s information, as it is essential for the enrollment process.
- Don’t attempt to enroll if you are using state- or federal-subsidized healthcare programs.
- Don’t ignore any requests for additional information after submission; they are vital for your enrollment.
- Don’t neglect to notify the program if your insurance information changes after submitting the form.
Misconceptions
Misconceptions about the RemiStart Enrollment form can lead to confusion or improper submission. Below are five common misconceptions:
- All patients are eligible to enroll in the RemiStart Program. Some patients may think they can enroll regardless of their insurance status. However, eligibility specifically requires private or commercial health insurance that covers a portion of REMICADE® costs.
- The RemiStart Program provides retroactive benefits. Many believe that the program can cover expenses incurred before enrollment. In reality, the offer is not retroactive, meaning it only applies to costs after enrollment.
- Patients can seek reimbursement from government programs and still enroll. Some might think they can enroll and also get reimbursement from Medicare, Medicaid, or other government-subsidized programs. The application clearly states that patients must confirm they will not seek such reimbursements to be eligible.
- Submitting the enrollment form guarantees a rebate. Individuals may assume that simply filling out and submitting the form will result in receiving a rebate. Rebate eligibility depends on meeting the program criteria, including submission of necessary documentation, such as Explanation of Benefits (EOB).
- Providing personal information is optional. Some might think sharing personal health information is not necessary for enrollment. However, the form requires permission to share health details with the program and its affiliates to process requests for assistance.
Understanding these points can help ensure that applicants complete the RemiStart Enrollment form correctly and without assumptions about the program.
Key takeaways
When filling out the RemiStart Enrollment form, it’s important to keep several key points in mind to ensure a smooth process.
- Confirm Patient Eligibility: Before completing the enrollment form, first review the patient eligibility requirements. This step helps ensure you meet the criteria for the program.
- Provide Complete Information: Accurately fill out all sections of the form, including patient information, insurance details, and prescriber information. Incomplete forms may delay your enrollment.
- Choose Your Payment Option: You can opt to receive rebates via a MasterCard® Rebate Debit Card or request a check sent directly to you or your infusion provider. Make a clear selection on the form.
- Insurance Information is Crucial: Include specific details about your private or commercial insurance coverage. A copy of your insurance card may be beneficial for reference.
- Understand Reimbursement Restrictions: Confirm that you will not seek reimbursement for REMICADE® expenses from certain government-funded programs. This is a requirement to enroll in the Rebate Program.
- Submit Required Documentation: Ensure that an Explanation of Benefits (EOB) or pharmacy receipt is submitted after each infusion to process your rebate. Failure to do so may hinder your ability to receive rebates.
- Contact Information is Key: Provide a valid email address and phone number. This will allow the program to reach you for any updates or necessary communications regarding your enrollment.
Understanding these points can simplify your experience when using the RemiStart Enrollment form. You can reach out for assistance if any questions arise during the process.
Browse Other Templates
Champva Providers - The form must be completed accurately to avoid complications.
Geico Premium Increase - Document the details of any damage to property other than vehicles.
New York Court Forms - Special skills and any licenses or certifications should be listed on the form.