Fill Out Your Ri Accident Report Form
The Ri Accident Report form is an essential document for anyone involved in a vehicle accident in Rhode Island. This form must be filled out accurately and submitted to the Division of Motor Vehicles, specifically the Accident Office, located in Cranston. It serves several critical functions. First, it captures detailed information about the accident, including the involved vehicles' specifications and any property damages. If the damage exceeds $1,000, the responsible party must provide itemized estimates and repair documents. It also requires specifics about the injured parties, including medical expenses and lost wages, which helps in processing claims effectively. The form emphasizes precise instructions to ensure proper completion, such as the proper use of black or blue ink and the necessity of signatures. Failing to provide comprehensive and truthful information may lead to complications or rejections of claims. Understanding the nuances of the Ri Accident Report form can greatly aid individuals in navigating the aftermath of a vehicle accident smoothly, ensuring that their rights and responsibilities are upheld.
Ri Accident Report Example
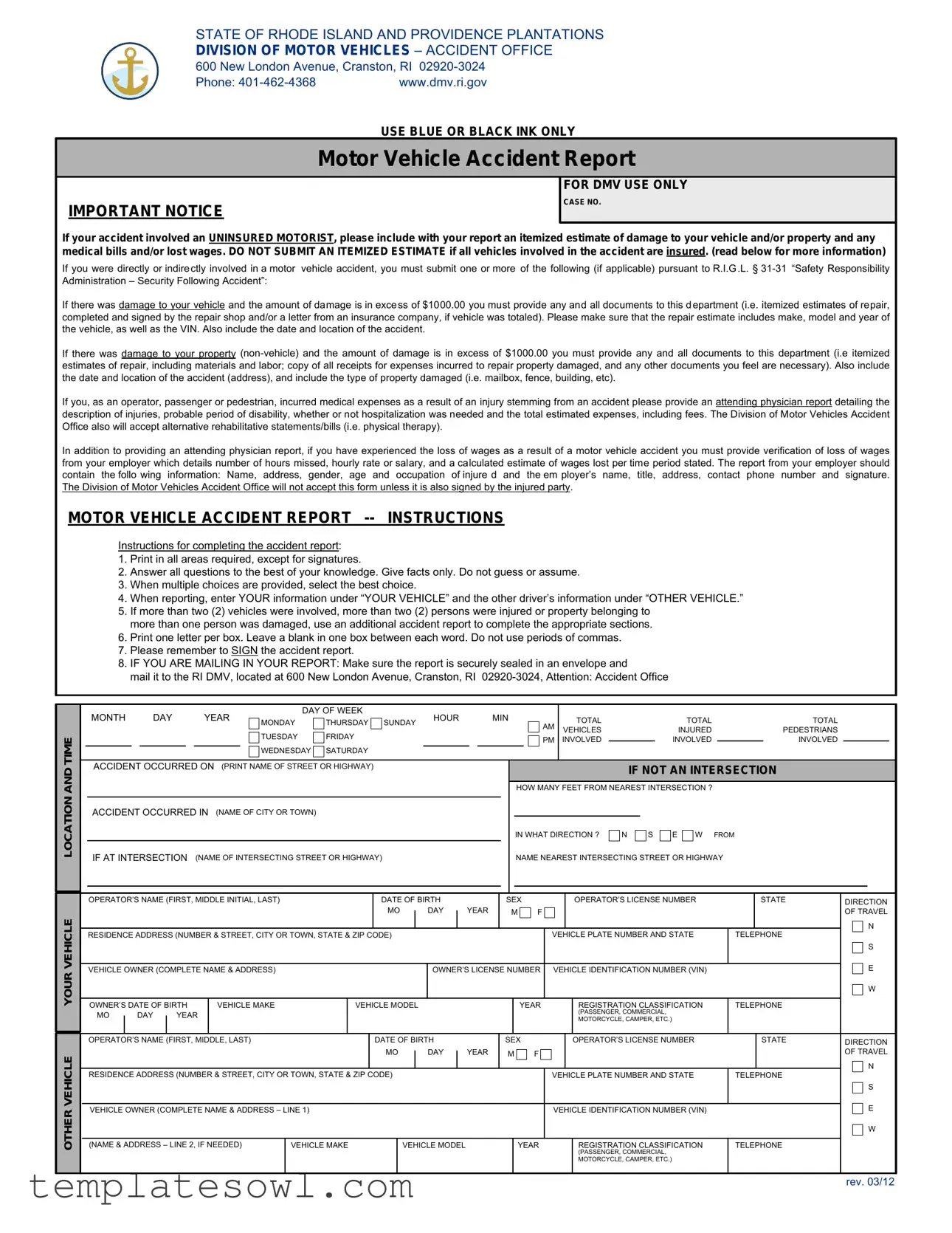
STATE OF RHODE ISLAND AND PROVIDENCE PLANTATIONS DIVISION OF MOTOR VEHICLES – ACCIDENT OFFICE
600 New London Avenue, Cranston, RI
Phone: |
www.dmv.ri.gov |
|
USE BLUE OR BLACK INK ONLY |
Motor Vehicle Accident Report
IMPORTANT NOTICE
FOR DMV USE ONLY
CASE NO.
If your accident involved an UNINSURED MOTORIST, please include with your report an itemized estimate of damage to your vehicle and/or property and any medical bills and/or lost wages. DO NOT SUBMIT AN ITEMIZED ESTIMATE if all vehicles involved in the accident are insured. (read below for more information)
If you were directly or indirectly involved in a motor vehicle accident, you must submit one or more of the following (if applicable) pursuant to R.I.G.L. §
If there was damage to your vehicle and the amount of damage is in excess of $1000.00 you must provide any and all documents to this department (i.e. itemized estimates of repair, completed and signed by the repair shop and/or a letter from an insurance company, if vehicle was totaled). Please make sure that the repair estimate includes make, model and year of the vehicle, as well as the VIN. Also include the date and location of the accident.
If there was damage to your property
If you, as an operator, passenger or pedestrian, incurred medical expenses as a result of an injury stemming from an accident please provide an attending physician report detailing the description of injuries, probable period of disability, whether or not hospitalization was needed and the total estimated expenses, including fees. The Division of Motor Vehicles Accident Office also will accept alternative rehabilitative statements/bills (i.e. physical therapy).
In addition to providing an attending physician report, if you have experienced the loss of wages as a result of a motor vehicle accident you must provide verification of loss of wages from your employer which details number of hours missed, hourly rate or salary, and a calculated estimate of wages lost per time period stated. The report from your employer should contain the follo wing information: Name, address, gender, age and occupation of injure d and the em ployer’s name, title, address, contact phone number and signature. The Division of Motor Vehicles Accident Office will not accept this form unless it is also signed by the injured party.
MOTOR VEHICLE ACCIDENT REPORT
OTHER VEHICLE YOUR VEHICLE LOCATION AND TIME
Instructions for completing the accident report:
1.Print in all areas required, except for signatures.
2.Answer all questions to the best of your knowledge. Give facts only. Do not guess or assume.
3.When multiple choices are provided, select the best choice.
4.When reporting, enter YOUR information under “YOUR VEHICLE” and the other driver’s information under “OTHER VEHICLE.”
5.If more than two (2) vehicles were involved, more than two (2) persons were injured or property belonging to more than one person was damaged, use an additional accident report to complete the appropriate sections.
6.Print one letter per box. Leave a blank in one box between each word. Do not use periods of commas.
7.Please remember to SIGN the accident report.
8.IF YOU ARE MAILING IN YOUR REPORT: Make sure the report is securely sealed in an envelope and
mail it to the RI DMV, located at 600 New London Avenue, Cranston, RI
|
|
MONTH |
|
DAY |
|
|
YEAR |
|
DAY OF WEEK |
|
|
|
HOUR |
|
|
|
MIN |
|
|
|
|
TOTAL |
|
|
|
|
TOTAL |
|
|
|
|
TOTAL |
|
|
|
|
||||||||||||||
|
|
|
|
|
MONDAY |
THURSDAY SUNDAY |
|
|
|
AM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
TUESDAY |
FRIDAY |
|
|
|
|
|
|
|
|
|
|
|
|
VEHICLES |
|
|
|
|
INJURED |
|
|
|
|
PEDESTRIANS |
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PM |
INVOLVED |
|
|
|
|
INVOLVED |
|
|
|
|
INVOLVED |
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
WEDNESDAY |
SATURDAY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
ACCIDENT OCCURRED ON (PRINT NAME OF STREET OR HIGHWAY) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
IF NOT AN INTERSECTION |
|
|
|
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
HOW MANY FEET FROM NEAREST INTERSECTION ? |
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
ACCIDENT OCCURRED IN |
(NAME OF CITY OR TOWN) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
IN WHAT DIRECTION ? |
N |
|
S |
E |
W |
FROM |
|
|
|
|
||||||||||
|
|
IF AT INTERSECTION (NAME OF INTERSECTING STREET OR HIGHWAY) |
|
|
|
|
|
|
|
|
|
|
|
NAME NEAREST INTERSECTING STREET OR HIGHWAY |
|
|
|
|
||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OPERATOR’S NAME (FIRST, MIDDLE INITIAL, LAST) |
|
|
|
DATE OF BIRTH |
|
|
|
|
SEX |
|
|
|
|
OPERATOR’S LICENSE NUMBER |
|
|
|
STATE |
|
DIRECTION |
||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MO |
|
|
|
DAY |
|
|
YEAR |
|
|
M |
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OF TRAVEL |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
N |
|
|
|
RESIDENCE ADDRESS (NUMBER & STREET, CITY OR TOWN, STATE & ZIP CODE) |
|
|
|
|
|
|
|
|
|
|
|
|
|
VEHICLE PLATE NUMBER AND STATE |
|
|
|
TELEPHONE |
|
|
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
E |
||||||||||||
|
|
VEHICLE OWNER (COMPLETE NAME & ADDRESS) |
|
|
|
|
|
|
|
|
OWNER’S LICENSE NUMBER |
VEHICLE IDENTIFICATION NUMBER (VIN) |
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
W |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
OWNER’S DATE OF BIRTH |
VEHICLE MAKE |
|
VEHICLE MODEL |
|
|
|
|
|
|
|
|
YEAR |
|
|
REGISTRATION CLASSIFICATION |
|
|
TELEPHONE |
|
|
|
|
||||||||||||||||||||||||||
|
|
MO |
|
DAY |
|
YEAR |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(PASSENGER, COMMERCIAL, |
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MOTORCYCLE, CAMPER, ETC.) |
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
OPERATOR’S NAME (FIRST, MIDDLE, LAST) |
|
|
|
|
|
DATE OF BIRTH |
|
|
|
|
SEX |
|
|
|
|
OPERATOR’S LICENSE NUMBER |
|
|
|
|
STATE |
|
DIRECTION |
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MO |
|
|
|
DAY |
|
|
YEAR |
|
M |
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OF TRAVEL |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
N |
|
|
|
RESIDENCE ADDRESS (NUMBER & STREET, CITY OR TOWN, STATE & ZIP CODE) |
|
|
|
|
|
|
|
|
|
|
|
|
|
VEHICLE PLATE NUMBER AND STATE |
|
|
|
TELEPHONE |
|
|
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
E |
||||||||||||||
|
|
VEHICLE OWNER (COMPLETE NAME & ADDRESS – LINE 1) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VEHICLE IDENTIFICATION NUMBER (VIN) |
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
W |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
(NAME & ADDRESS – LINE 2, IF NEEDED) |
|
VEHICLE MAKE |
|
VEHICLE MODEL |
|
|
|
|
|
YEAR |
|
|
REGISTRATION CLASSIFICATION |
|
|
TELEPHONE |
|
|
|
|
||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(PASSENGER, COMMERCIAL, |
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MOTORCYCLE, CAMPER, ETC.) |
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
rev. 03/12
STATE PROPERTY
CITY/TOWN PROPERTY
PRIVATE PROPERTY
OWNER’S NAME |
OWNER’S ADDRESS (NUMBER & STREET, CITY OR TOWN, STATE & ZIP CODE) |
HOME PHONE
CELL PHONE
WORK PHONE
DAMAGE DESCRIPTION
VEHICLE DAMAGE
APPROXIMATE COST TO REPAIR |
|
APPROXIMATE COST TO REPAIR |
|
YOUR VEHICLE (VEHICLE 1) |
$ ____________________ |
OTHER VEHICLE (VEHICLE 2) |
$ ____________________ |
INJURED
ACCIDENT CONDITIONS
|
|
|
|
|
|
|
|
NAME $1'$''5(66OF INJURED (FIRST, MIDDLE INITIAL, LAST) |
NUMBER & STREET |
CITY/TOWN |
STATE ZIP |
INJURED WAS RIDING |
|||
|
|
|
|
|
|||
|
|
|
|
|
IN VEHICLE # |
||
|
|
|
|
|
|
|
|
|
AGE |
SEX |
|
ACCIDENT SEVERITY CONDITION AT SCENE OF ACCIDENT |
|
PERSON INJURED |
|||||||
|
|
M |
F |
1 |
FATAL |
3 |
BRUISES OR ABRASIONS |
1 |
PEDESTRIAN |
5 |
VEHICLE OPERATOR |
||
|
|
|
|
2 |
PEDALCYCLIST |
6 |
VEHICLE PASSENGER |
||||||
|
|
|
|
2 |
BLEEDING OR BROKEN BONES |
4 |
COMPLAINT OF PAIN |
||||||
|
|
|
|
3 |
PASSENGER IN BUS |
7 |
MOTORCYCLE OPERATOR |
||||||
|
|
|
|
|
|
|
|
4 |
OTHER |
8 |
MOTORCYCLE PASSENGER |
||
NAME AND ADDRESS OF INJURED (FIRST, MIDDLE INITIAL, LAST)180%(5 |
675((7CITY/TOWN |
STATE=,3 |
|
INJURED WAS RIDING |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
IN VEHICLE # |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
AGE |
SEX |
|
ACCIDENT SEVERITY CONDITION AT SCENE OF ACCIDENT |
|
PERSON INJURED |
|||||||
|
|
M |
F |
|
|
|
|
|
|
|
|
|
|
1 |
FATAL |
3 |
BRUISES OR ABRASIONS |
1 |
PEDESTRIAN |
5 |
VEHICLE OPERATOR |
||||||
|
|
|
|
2 |
PEDALCYCLIST |
6 |
VEHICLE PASSENGER |
||||||
|
|
|
|
2 |
BLEEDING OR BROKEN BONES |
4 |
COMPLAINT OF PAIN |
||||||
|
|
|
|
3 |
PASSENGER IN BUS |
7 |
MOTORCYCLE OPERATOR |
||||||
|
|
|
|
|
|
|
|
4 |
OTHER |
8 |
MOTORCYCLE PASSENGER |
||
ACCIDENT INVOLVED COLLISION WITH ...
1 |
PEDESTRIAN |
4 |
MOVING VEHICLE |
7 |
FIXED OBJECT |
10 OTHER _______________ |
2 |
PEDALCYCLE |
5 |
VEHICLE STOPPED IN ROAD |
8 |
OBJECT IN ROAD |
|
3 |
NO COLLISION – RAN OFF ROAD |
6 |
PARKED MOTOR VEHICLE |
9 |
NO COLLISION - OVERTURNED |
|
IN YOUR OWN WORDS, PLEASE DESCRIBE WHAT HAPPENED ...
I, THE UNDERSIGNED, DECLARE UNDER PENALTY OF PERJURY THAT ALL STATEMENTS MADE ON THIS REPORT ARE TRUE AND COMPLETE TO THE BEST OF MY KNOWLEDGE AND BELIEF.
OPERATOR’S SIGNATURE(THIS REPORT MUST BE SIGNED): |
PRINT YOUR NAME: |
|
|||||
|
|
|
|
|
|
|
|
YOUR INSURANCE |
|
INFORMATION |
WAS YOUR VEHICLE OR |
NAME OF YOUR INSURANCE COMPANY (NOT AGENT) |
POLICY NUMBER |
||
|
|
|
|
||||
|
THE VEHICLE YOU WERE |
|
|
|
|||
|
OPERATING INSURED |
|
|
|
|||
|
(LIABILITY INSURANCE) |
|
|
|
|||
|
AT THE TIME OF |
|
|
|
|||
|
THE ACCIDENT? |
|
|
|
|||
|
IF “YES”, COMPLETE |
NAME OF POLICYHOLDER |
STREET ADDRESS |
||||
|
ATTACHED FORM |
|
|
|
|||
|
YES |
NO |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
DATE: |
|
|
|
|
|
|
POLICY EFFECTIVE DATES |
|
|
|
FROM: __________________________ |
|
|
|
|
TO: _________________________ |
CITY/TOWN |
|
|
STATE/ZIP |
|
|||
YOUR MOTOR VEHICLE INSURANCE INFORMATION
DATE OF ACCIDENT: |
PLACE OF ACCIDENT: |
FOR DMV USE ONLY
CASE NO.
DESCRIPTION OF VEHICLE INVOLVED IN ACCIDENT MUST CORRESPOND TO “YOUR VEHICLE” ON ACCIDENT REPORT
VEHICLE MAKE: |
TYPE: |
YEAR: |
VIN: |
|
|
|
|
|
|
NAME OF OPERATOR: |
STREET ADDRESS: |
|
CITY / TOWN: |
STATE / ZIP: |
|
|
|
|
|
NAME OF OWNER: |
STREET ADDRESS: |
|
CITY / TOWN: |
STATE / ZIP: |
|
|
|
|
|
NAME OF INSURANCE COMPANY (NOT AGENT): |
|
POLICY NUMBER: |
EFFECTIVE PERIOD: |
|
|
|
|
FROM: ____________________ |
TO: ____________________ |
NAME OF POLICYHOLDER: |
STREET ADDRESS: |
|
CITY / TOWN: |
STATE / ZIP: |
|
|
|
|
|
NAME OF INSURANCE AGENT |
STREET ADDRESS: |
|
CITY / TOWN: |
STATE / ZIP: |
WHO ISSUED POLICY: |
|
|
|
|
|
|
|
|
|
YOUR SIGNATURE: |
|
|
DATE SIGNED: |
|
|
|
|
|
|
FOR USE BY INSURANCE COMPANY ONLY - DO NOT WRITE IN THIS AREA
RETURN THIS FORM ONLY IF NO STANDARD POLICY WAS IN EFFECT AS ALLEGED BY MOTORIST
WITH REGARD TO AN AUTOMOBILE LIABILITY INSURANCE POLICY FOR THE POLICYHOLDER NAMED ON THE REVERSE SIDE HEREOF, THE UNDERSIGNED INSURANCE COMPANY ADVISED YOU IN ACCORDANCE WITH THE ITEMS CHECKED BELOW:
1 |
No policy was in effect on the date of the accident. |
|
2 |
Our policy for the named policyholder applies to him/her as the operator but it does not apply to the owner of the vehicle involved in the accident. |
|
3 |
Our policy applies to the owner of the vehicle, but does not apply to the operator of the vehicle involved in the accident. |
|
4 |
Our policy affords bodily injury coverage only. |
Remarks: |
|
|
|
5 |
Our policy affords property damage coverage only. |
|
To: STATE OF RHODE ISLAND AND PROVIDENCE PLANTATIONS DIVISION OF MOTOR VEHICLES
600 NEW LONDON AVENUE
CRANSTON, RI
DATE: _______________________________________
Name of Insurance Company
By:
Authorized Representative
Form Characteristics
| Fact Name | Description |
|---|---|
| Governing Law | This form is governed by Rhode Island General Laws, specifically R.I.G.L. § 31-31, which relates to Safety Responsibility Administration. |
| Required Documentation | If damages exceed $1,000, an itemized estimate of repairs must be submitted along with relevant documents. |
| Medical Bills | Injured parties must provide an attending physician report detailing their injuries, expenses, and any necessary rehabilitation. |
| Missing Wages | Verification from the employer is necessary if the individual has lost wages due to the accident. This document needs specific information about the employee and the employer. |
| Sealing and Mailing | If submitting the report by mail, ensure it is sealed securely in an envelope addressed to the DMV Accident Office. |
| Signature Requirement | The form must be signed by the injured party for validation. Without this signature, it will not be accepted. |
Guidelines on Utilizing Ri Accident Report
Completing the Rhode Island Accident Report form can help ensure that all necessary information is documented accurately and submitted to the appropriate authorities. Submitting this form promptly is crucial for processing claims and can facilitate communication with insurance companies.
- Use blue or black ink to fill out the form.
- Print clearly in all areas except for signatures.
- Answer all questions honestly and to the best of your knowledge. Provide only factual information.
- Select the best choice when there are multiple options available.
- Fill in your information under "YOUR VEHICLE" and the other driver’s information under "OTHER VEHICLE."
- If there are more than two vehicles involved, complete an additional report for any extra vehicles or damages.
- Write one letter per box, leaving a blank space between each word. Avoid using periods or commas.
- Ensure you sign the accident report before submitting.
- If mailing the report, secure it in an envelope and send it to the RI DMV—600 New London Avenue, Cranston, RI 02920-3024, Attention: Accident Office.
What You Should Know About This Form
What should I do if my accident involved an uninsured motorist?
If you were involved in an accident with an uninsured motorist, it is crucial to submit an itemized estimate of the damage to your vehicle and/or property along with your accident report. Additionally, you should include any medical bills and documentation for lost wages, if applicable. This information will support your claim and provide a clearer picture of your losses.
What is the damage threshold for reporting an accident to the DMV?
According to Rhode Island law, if the damage to your vehicle exceeds $1,000, you are required to submit all relevant documentation to the DMV. This can include itemized repair estimates from a professional shop, along with specifics like the vehicle's make, model, year, and VIN. Similarly, if your property damages exceed $1,000, you must provide estimates and receipts for repairs, specifying the type of property damaged and the location of the incident.
What medical documentation is necessary after an accident?
If you incurred medical expenses due to accident-related injuries, you need to provide an attending physician's report. This report should describe your injuries, detail any required hospitalization, and list your estimated medical expenses. Additionally, if you have lost wages because of the injury, you must provide evidence from your employer outlining the hours missed and the calculated losses.
Can I submit this form electronically or do I have to mail it?
The preferred method for submitting the Ri Accident Report is by mail. Make sure to securely seal your report in an envelope and send it to the Rhode Island DMV at the specified address. While electronic submissions may not be mentioned, confirm any updates or changes in submission policies directly through the DMV’s official website or by calling their office.
What happens if I do not submit the report on time?
Failing to submit the Ri Accident Report in a timely manner can result in penalties and may affect your driving record. The state requires this report to ensure compliance with safety and insurance regulations. To avoid any complications, it is advisable to complete and send your report as soon as possible following an accident.
Common mistakes
Filling out the RI Accident Report form can be a straightforward process, but many people still make common mistakes that can lead to confusion or delays. One frequent error occurs when individuals do not answer all the questions thoroughly. Each section of the form is designed to gather specific information that can be critical for processing the accident report. Omitting details or providing half-hearted answers can complicate matters, creating unnecessary back-and-forth communication with the DMV.
Another mistake people often make is submitting the report without their signature. This oversight might seem minor, but it renders the report invalid. The form explicitly states that the report must be signed by the injured party. If the necessary signature is missing, the DMV cannot accept the document, which could lead to additional frustrations for everyone involved.
Many forget to provide proper documentation for damages and expenses. If there were injuries or property damage exceeding the threshold of $1,000, it's necessary to include all relevant estimates and medical reports. The failure to submit this documentation can cause significant delays as the DMV may require additional follow-up requests, adding to the stress of an already challenging situation.
Another area of concern is the clarity of the information provided. Many individuals do not print their details clearly, leading to misinterpretations. The form requires that information be printed in a specific format. Mistakes like not leaving a blank space between words or using incorrect ink can cause confusion and slow down the processing times of the reports.
Finally, many individuals neglect to double-check the specific requirements related to the type of accident. If the involvement of an uninsured motorist is present, additional documentation is essential. Similarly, if there were multiple vehicles or injuries, an additional report may be needed. Not adhering to these guidelines can result in complications that could have easily been avoided with some careful reading and planning.
Documents used along the form
When filing an RI Accident Report, several supplementary forms and documents may be necessary to provide a comprehensive account of the incident. These documents help ensure that all relevant information is gathered for further investigation or insurance claims. Here is a list of commonly used documents alongside the RI Accident Report form:
- Uninsured Motorist Claim Form: This form is required if the accident involves an uninsured driver. It helps claim insurance coverage when damage occurs due to an uninsured motorist.
- Itemized Repair Estimates: This document outlines the estimated costs for vehicle or property repairs. It should include details on the repairs needed, their cost, and a breakdown of labor and materials.
- Medical Expense Reports: These reports detail the medical costs incurred due to injuries from the accident. They include hospital bills, physician reports, and itemized expenses relating to treatment.
- Employer Wage Verification Form: This document verifies lost wages if the injured party could not work due to the accident. It typically includes the employee's hours missed and their salary information.
- Property Damage Documentation: If any non-vehicle property was damaged, this documentation records the details of the damage and associated costs. It can include receipts and photographs of the damaged property.
- Accident Scene Photographs: Visual evidence from the accident scene can provide context. These photographs may include images of vehicle damage, road conditions, and other relevant environmental factors.
- Witness Statements: Statements from individuals who witnessed the accident can offer additional perspectives and corroborate the accounts of those involved in the incident.
- Insurance Company Correspondence: Any written correspondence with insurance companies regarding the accident should be included. This may show communications about claims or coverage related to the incident.
Collecting and submitting these additional documents can aid in the processing of the accident report and facilitate any subsequent claims or investigations. Providing complete and accurate documentation is essential for ensuring that all aspects of the incident are recorded and addressed appropriately.
Similar forms
- Personal Injury Report: Like the Ri Accident Report form, a personal injury report documents details surrounding an incident that caused injury. Both forms require specific information on the injured parties and injuries sustained, including medical bills and treatment details.
- Property Damage Report: This document, similar to the Ri Accident Report, outlines damages to property caused by an accident. Both reports require itemized lists of repairs and costs, ensuring clarity in damages sustained.
- Insurance Claim Form: Much like the Ri Accident Report, an insurance claim form captures details and circumstances of an incident to initiate a claim. Both forms gather information like accident location, involved parties, and insurance details to process claims efficiently.
- Workers' Compensation Claim Form: This form is similar to the Ri Accident Report in documenting injuries and circumstances surrounding work-related accidents. Both require detailed accounts of injuries, involved individuals, and medical treatment to assess eligibility for compensation.
- Motor Vehicle Report (MVR): The MVR parallels the Ri Accident Report as it contains vital information about the driver's history and incidents. Both documents share common elements, such as vehicle information, driver details, and accident specifics.
- Incident Report Form: Similar in nature, incident report forms capture detailed accounts of an unusual event or accident, often used in various settings, including schools and workplaces. Both forms require factual accounts and specifics about the incident and those involved.
- Police Accident Report: Police accident reports share similarities with the Ri Accident Report since they serve to document the facts and circumstances of a traffic incident. Both need details on vehicles, drivers, and physical damage, although police reports typically carry official legal weight.
Dos and Don'ts
Filling out the RI Accident Report form can feel overwhelming, but adhering to certain guidelines can make the process smoother. Here’s a list of six key dos and don'ts to keep in mind.
- Do use blue or black ink only to ensure clarity.
- Do answer all questions accurately and honestly. Provide as many facts as possible without guessing.
- Do include all necessary documentation if the accident involved significant damage, injuries, or uninsured motorists.
- Do print one letter per box and leave a blank box between each word for easy reading.
- Don't forget to sign the report. An unsigned report will be rejected.
- Don't submit any itemized estimates for damages if all vehicles involved are insured, as this is not necessary.
By following these dos and don'ts, you're more likely to submit a complete and effective report, which can save you time and hassle in the event of an accident claim.
Misconceptions
Understanding the Ri Accident Report Form is crucial for anyone involved in a vehicle accident in Rhode Island. However, several misconceptions often lead to confusion. Here are seven common misconceptions regarding this form, accompanied by explanations to clarify them:
- Misconception 1: Only the driver needs to fill out the report.
- Misconception 2: Submitting an itemized estimate of damage is mandatory in every case.
- Misconception 3: Medical information isn’t necessary for the accident report.
- Misconception 4: The accident report can be submitted without a signature.
- Misconception 5: The order of information on the form does not matter.
- Misconception 6: You can submit the report in any ink color.
- Misconception 7: Handwritten notes are acceptable as substitution for the formal report.
This is incorrect. Anyone who was directly or indirectly involved in the accident, including passengers and pedestrians, may need to complete the report if there are damages or injuries to report.
Only if there is damage exceeding $1,000 to your vehicle or property, and when uninsured motorists are involved, should you submit an itemized estimate. For insured vehicles, this is not necessary.
This is a misunderstanding. If there are medical expenses stemming from injuries due to the accident, an attending physician's report detailing the injuries and expenses must be included.
The form will not be accepted unless signed by the injured party. A signature is an essential part of validating the information within the report.
It's vital to follow the order outlined in the instructions. The driver’s information should be listed under “YOUR VEHICLE” while the other driver’s information goes under “OTHER VEHICLE.”
This is false. The instructions specify the use of blue or black ink only. Using any other color may result in issues with processing your report.
This is not allowed. The formal Ri Accident Report form must be completed as indicated, and any handwritten notes will not be accepted as a substitute for the comprehensive documentation required by the DMV.
By understanding these misconceptions, individuals can ensure a smoother and more accurate reporting process following a motor vehicle accident. Familiarity with the requirements can prevent delays and complications when dealing with the Rhode Island Division of Motor Vehicles.
Key takeaways
1. Use Black or Blue Ink: Always fill out the Ri Accident Report form using only blue or black ink. This ensures clarity and legibility.
2. Attach Supporting Documentation: If involved in an accident with an uninsured motorist, include an itemized estimate of vehicle damage and any medical bills. Do not submit estimates if all vehicles are insured.
3. Report Damage Over $1000: Provide documentation for any vehicle or property damage exceeding $1000. Include details like the make, model, year of vehicles, and nature of property damage.
4. Complete All Sections Accurately: Fill in all areas of the form to the best of your knowledge. Avoid guessing and ensure you enter your details under “YOUR VEHICLE” and the other driver’s info under “OTHER VEHICLE.”
5. Sign the Report: The form must be signed by the party making the report. Ensure that it is also completed and signed by any injured parties if applicable.
6. Mail Your Report Correctly: If sending the report by mail, securely seal it in an envelope and send it to the RI DMV, ensuring it is addressed to the Accident Office.
Browse Other Templates
Dphs Chennai - The regulations surrounding the submission of the Convocation form uphold academic integrity.
Body Beast Bulk Back Worksheet - Each circuit set provides clear instructions on the exercises to complete.
What Is Jha - Utilize the JSA to foster a culture of safety.