Fill Out Your Scif E3067 Form
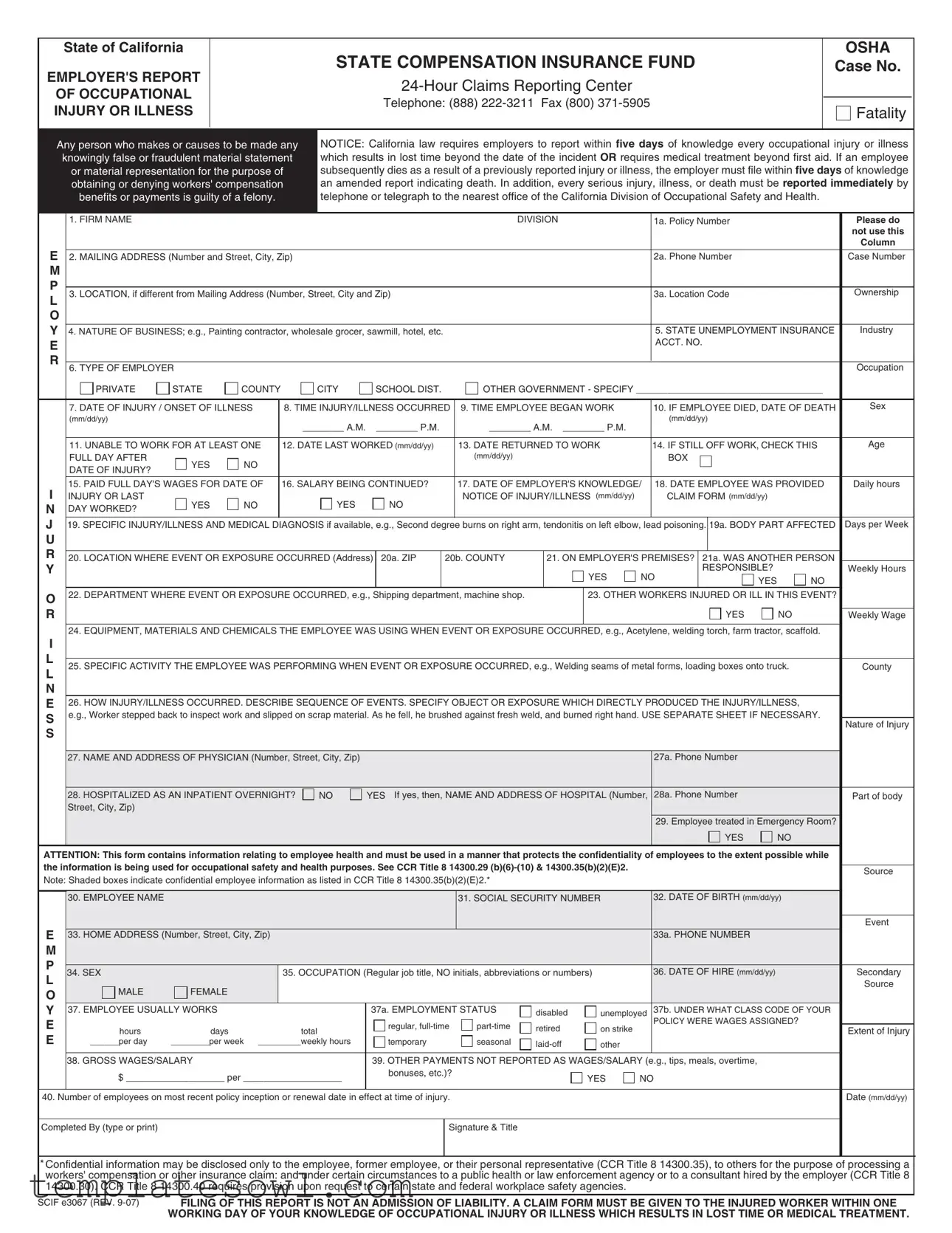
In California, when an employee suffers an occupational injury or illness, employers are required to report the incident using the SCIF E3067 form. This form is essential in documenting various details regarding the incident, including the nature of the injury or illness, the employee's treatment, and the circumstances surrounding the event. Employers must fill out sections that capture vital information such as the date and time of the incident, the employee's job title, and whether the employee required medical assistance. Timeliness is crucial; California law mandates that employers report injuries within five days of learning about them. In cases of fatalities or serious injuries, immediate notification to the California Division of Occupational Safety and Health is required. The form also seeks information on how the injury or illness occurred, thus providing a comprehensive picture to ensure proper handling of workers' compensation claims. It emphasizes the importance of confidentiality regarding the employee's personal information and outlines certain responsibilities regarding disclosures. Completing this form accurately and promptly is a critical step in protecting both the rights of the injured employee and the employer's obligations under state law.
Scif E3067 Example
State of California
EMPLOYER'S REPORT
OF OCCUPATIONAL INJURY OR ILLNESS
STATE COMPENSATION INSURANCE FUND
Telephone: (888)
OSHA
Case No.
Fatality
Any person who makes or causes to be made any |
|
NOTICE: California law requires employers to report within five days of knowledge every occupational injury or illness |
||||||||||||||||||||
|
knowingly false or fraudulent material statement |
|
which results in lost time beyond the date of the incident OR requires medical treatment beyond first aid. If an employee |
|||||||||||||||||||
|
|
or material representation for the purpose of |
|
subsequently dies as a result of a previously reported injury or illness, the employer must file within five days of knowledge |
||||||||||||||||||
|
|
obtaining or denying workers' compensation |
|
an amended report indicating death. In addition, every serious injury, illness, or death must be reported immediately by |
||||||||||||||||||
|
|
benefits or payments is guilty of a felony. |
|
|
telephone or telegraph to the nearest office of the California Division of Occupational Safety and Health. |
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1. FIRM NAME |
|
|
|
|
|
|
|
|
DIVISION |
|
|
1a. Policy Number |
|
|
|
Please do |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
not use this |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Column |
E |
2. MAILING ADDRESS (Number and Street, City, Zip) |
|
|
|
|
|
|
|
|
|
|
2a. Phone Number |
|
|
|
Case Number |
||||||
M |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
P |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3. LOCATION, if different from Mailing Address (Number, Street, City and Zip) |
|
|
|
|
|
|
3a. Location Code |
|
|
|
Ownership |
||||||||||
L |
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
O |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Y |
4. NATURE OF BUSINESS; e.g., Painting contractor, wholesale grocer, sawmill, hotel, etc. |
|
|
|
|
|
|
5. STATE UNEMPLOYMENT INSURANCE |
Industry |
|||||||||||||
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ACCT. NO. |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
R |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6. TYPE OF EMPLOYER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Occupation |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
PRIVATE |
STATE |
COUNTY |
|
CITY |
|
SCHOOL DIST. |
|
OTHER GOVERNMENT - SPECIFY ____________________________________ |
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
7. DATE OF INJURY / ONSET OF ILLNESS |
8. TIME INJURY/ILLNESS OCCURRED |
9. TIME EMPLOYEE BEGAN WORK |
|
10. IF EMPLOYEE DIED, DATE OF DEATH |
Sex |
|||||||||||||||
|
|
(mm/dd/yy) |
|
|
|
________ A.M. |
|
________ P.M. |
|
|
|
|
|
|
(mm/dd/yy) |
|
|
|
|
|||
|
|
|
|
|
|
|
|
________ A.M. ________ P.M. |
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
11. UNABLE TO WORK FOR AT LEAST ONE |
12. DATE LAST WORKED (mm/dd/yy) |
|
13. DATE RETURNED TO WORK |
|
14. IF STILL OFF WORK, CHECK THIS |
Age |
||||||||||||||
|
|
FULL DAY AFTER |
YES |
NO |
|
|
|
|
|
|
(mm/dd/yy) |
|
|
|
|
BOX |
|
|
|
|
||
|
|
DATE OF INJURY? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
15. PAID FULL DAY'S WAGES FOR DATE OF |
16. SALARY BEING CONTINUED? |
|
17. DATE OF EMPLOYER'S KNOWLEDGE/ |
18. DATE EMPLOYEE WAS PROVIDED |
Daily hours |
|||||||||||||||
I |
|
INJURY OR LAST |
YES |
NO |
|
|
YES |
|
NO |
|
NOTICE OF INJURY/ILLNESS (mm/dd/yy) |
|
CLAIM FORM (mm/dd/yy) |
|
|
|
||||||
N |
|
DAY WORKED? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
J |
19. SPECIFIC INJURY/ILLNESS AND MEDICAL DIAGNOSIS if available, e.g., Second degree burns on right arm, tendonitis on left elbow, lead poisoning. |
19a. BODY PART AFFECTED |
Days per Week |
|||||||||||||||||||
U |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
R |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
20. LOCATION WHERE EVENT OR EXPOSURE OCCURRED (Address) |
20a. ZIP |
20b. COUNTY |
|
21. ON EMPLOYER'S PREMISES? |
21a. WAS ANOTHER PERSON |
|
|||||||||||||||
Y |
|
|
|
|
|
|
|
|
|
|
|
|
|
YES |
NO |
RESPONSIBLE? |
|
|
Weekly Hours |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
YES |
NO |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
O |
|
22. DEPARTMENT WHERE EVENT OR EXPOSURE OCCURRED, e.g., Shipping department, machine shop. |
|
|
23. OTHER WORKERS INJURED OR ILL IN THIS EVENT? |
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
R |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
YES |
|
NO |
Weekly Wage |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
24. EQUIPMENT, MATERIALS AND CHEMICALS THE EMPLOYEE WAS USING WHEN EVENT OR EXPOSURE OCCURRED, e.g., Acetylene, welding torch, farm tractor, scaffold. |
|
|||||||||||||||||||
I |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
L |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
25. SPECIFIC ACTIVITY THE EMPLOYEE WAS PERFORMING WHEN EVENT OR EXPOSURE OCCURRED, e.g., Welding seams of metal forms, loading boxes onto truck. |
County |
||||||||||||||||||||
L |
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
E |
|
26. HOW INJURY/ILLNESS OCCURRED. DESCRIBE SEQUENCE OF EVENTS. SPECIFY OBJECT OR EXPOSURE WHICH DIRECTLY PRODUCED THE INJURY/ILLNESS, |
|
|||||||||||||||||||
S |
|
e.g., Worker stepped back to inspect work and slipped on scrap material. As he fell, he brushed against fresh weld, and burned right hand. USE SEPARATE SHEET IF NECESSARY. |
|
|||||||||||||||||||
|
Nature of Injury |
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
S |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
27. NAME AND ADDRESS OF PHYSICIAN (Number, Street, City, Zip) |
|
|
|
|
|
|
|
|
27a. Phone Number |
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
28. HOSPITALIZED AS AN INPATIENT OVERNIGHT? |
|
NO |
YES If yes, then, NAME AND ADDRESS OF HOSPITAL (Number, |
28a. Phone Number |
|
|
|
Part of body |
||||||||||||
|
|
Street, City, Zip) |
|
|
|
|
|
|
|
|
(Number, Street, City, Zip) |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
29. Employee treated in Emergency Room? |
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
YES |
|
NO |
|
|
ATTENTION: This form contains information relating to employee health and must be used in a manner that protects the confidentiality of employees to the extent possible while |
|
|||||||||||||||||||||
the information is being used for occupational safety and health purposes. See CCR Title 8 14300.29 |
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
Source |
|||||||||||||||
Note: Shaded boxes indicate confidential employee information as listed in CCR Title 8 14300.35(b)(2)(E)2.* |
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
30. EMPLOYEE NAME |
|
|
|
|
|
|
|
|
31. SOCIAL SECURITY NUMBER |
|
32. DATE OF BIRTH (mm/dd/yy) |
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Event |
E |
|
33. HOME ADDRESS (Number, Street, City, Zip) |
|
|
|
|
|
|
|
|
|
|
|
33a. PHONE NUMBER |
|
|
|
|
||||
M |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
P |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
34. SEX |
|
|
35. OCCUPATION (Regular job title, NO initials, abbreviations or numbers) |
|
36. DATE OF HIRE (mm/dd/yy) |
|
|
Secondary |
|||||||||||||
L |
|
|
|
|
|
|
||||||||||||||||
|
MALE |
FEMALE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Source |
|
O |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Y |
37. EMPLOYEE USUALLY WORKS |
|
|
|
|
37a. EMPLOYMENT STATUS |
disabled |
unemployed |
37b. UNDER WHAT CLASS CODE OF YOUR |
|
||||||||||||
E |
|
|
|
|
|
|
|
|
regular, |
retired |
on strike |
|
POLICY WERE WAGES ASSIGNED? |
|
||||||||
|
hours |
days |
|
|
total |
|
|
Extent of Injury |
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
______per day |
________per week _________weekly hours |
|
temporary |
|
seasonal |
other |
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
38. GROSS WAGES/SALARY |
|
|
|
|
39. OTHER PAYMENTS NOT REPORTED AS WAGES/SALARY (e.g., tips, meals, overtime, |
|
|
|
|
|||||||||||
|
|
$ ___________________ per ___________________ |
|
bonuses, etc.)? |
|
|
|
YES |
NO |
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
40. Number of employees on most recent policy inception or renewal date in effect at time of injury. |
|
|
|
|
|
|
|
|
|
|
|
Date (mm/dd/yy) |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Completed By (type or print) |
|
|
|
|
|
|
|
Signature & Title |
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
* Confidential information may be disclosed only to the employee, former employee, or their personal representative (CCR Title 8 14300.35), to others for the purpose of processing a workers' compensation or other insurance claim: and under certain circumstances to a public health or law enforcement agency or to a consultant hired by the employer (CCR Title 8 14300.30). CCR Title 8 14300.40 requires provision upon request to certain state and federal workplace safety agencies.
SCIF e3067 (REV. |
FILING OF THIS REPORT IS NOT AN ADMISSION OF LIABILITY. A CLAIM FORM MUST BE GIVEN TO THE INJURED WORKER WITHIN ONE |
|
WORKING DAY OF YOUR KNOWLEDGE OF OCCUPATIONAL INJURY OR ILLNESS WHICH RESULTS IN LOST TIME OR MEDICAL TREATMENT. |
Form Characteristics
| Fact Name | Details |
|---|---|
| Form Purpose | The SCIF E3067 form is used by employers in California to report occupational injuries or illnesses to the State Compensation Insurance Fund. |
| Reporting Timeline | California law mandates that employers report any work-related injury or illness within five days of knowing about it. |
| Employer Responsibilities | Employers must provide a claim form to the injured worker within one working day of the injury or illness. |
| Deadline for Amended Reports | If an employee dies due to a previously reported injury, an amended report must be filed within five days of knowledge. |
| Notification Requirements | Serious injuries, illnesses, or deaths must be reported immediately to the California Division of Occupational Safety and Health. |
| Protecting Confidentiality | Care should be taken to maintain the confidentiality of employee health information when using this form. |
| Employer Identification | Employers must provide detailed identification such as firm name, mailing address, and policy number on the form. |
| Occupational Injury Details | Specific descriptions of the injury, illness, and the sequence of events leading to it are required on the form. |
| Legal Consequences | Filing knowingly false information or failing to report injuries can result in felony charges. |
| California Code References | The form aligns with California Code of Regulations Title 8, specifically regarding injury reporting and confidentiality. |
Guidelines on Utilizing Scif E3067
Completing the SCIF E3067 form is an important step in reporting an occupational injury or illness in California. This form needs accurate and timely information to ensure compliance with state regulations and to facilitate the claims process. Below are the steps required to fill out this form correctly.
- Firm Name: Enter the name of your business or organization.
- Policy Number: Fill in your workers' compensation policy number.
- Mailing Address: Write the complete mailing address, including street, city, and zip code.
- Phone Number: Provide a contact number for your organization.
- Location: If different from the mailing address, include the address where the injury occurred.
- Location Code: Indicate the location code, if applicable.
- Nature of Business: Describe the type of business or industry your company operates in.
- State Unemployment Insurance Account Number: Enter your account number if you have one.
- Type of Employer: Check the appropriate box for your type of employer (private, public, etc.).
- Date of Injury: Fill in the date when the injury or illness occurred.
- Time of Injury: Record the time the injury happened, indicating AM or PM.
- Date Employee Last Worked: Provide the date the injured employee last worked.
- Specific Injury/Illness: Describe the injury or illness along with a medical diagnosis if available.
- Location of Event: Include the specific location where the incident took place.
- Department: State the department where the event or exposure occurred.
- Name and Address of Physician: Fill in the physician’s name and contact details.
- Employee Name: Enter the full name of the injured employee.
- Social Security Number: Record the employee's social security number.
- Date of Birth: Provide the employee's date of birth.
- Home Address: Include the employee’s home address.
- Occupation: Write the employee’s job title.
- Date of Hire: Document the date when the employee was hired.
- Gross Wages/Salary: Enter the employee’s gross salary or wage details.
- Completed By: Type or print your name and title in the designated area.
- Signature: Include a signature to certify the accuracy of the information submitted.
After completing the form, ensure it is submitted to the appropriate authorities as mandated. Attention to detail is critical in this process, and the form must be submitted within the required time frame to adhere to California state laws.
What You Should Know About This Form
What is the purpose of the SCIF E3067 form?
The SCIF E3067 form, known as the Employer's Report of Occupational Injury or Illness, is designed to report incidents of workplace injuries or illnesses that result in lost time or require medical treatment beyond first aid. This report assists in fulfilling California's legal obligations regarding workers' compensation and ensuring proper tracking of workplace safety incidents.
Who is required to fill out the SCIF E3067 form?
Employers in California must complete the SCIF E3067 form if an employee experiences an occupational injury or illness that meets specific criteria. This includes situations where the injury results in lost workdays, requires medical treatment, or in cases of a fatality. The employer has a responsibility to report these incidents within five days of being aware of them.
When should the SCIF E3067 form be submitted?
The form should be submitted within five days of the employer’s knowledge of the injury or illness that results in lost time or requires more than first aid. If an injury leads to an employee's death, an amended report must also be submitted within five days of knowledge of the death.
What information is required on the form?
The SCIF E3067 form requires detailed information, including the firm’s name and address, date and time of the injury, nature of the business, specifics of the injury or illness, treatments provided, and employee details such as name and social security number. Accurate and complete information is essential for effective reporting and compliance.
Is there a penalty for failing to file the SCIF E3067 form on time?
Yes, failure to comply with the reporting requirements can result in penalties. Employers may face legal repercussions for not submitting timely and accurate reports of occupational injuries or illnesses, as this neglect can impact their workers’ compensation claims and safety compliance.
Are there any confidentiality concerns when using the SCIF E3067 form?
Confidentiality is paramount when handling the SCIF E3067 form. This report contains sensitive employee health information that must be protected. Employers are required to use this information solely for occupational safety and health purposes and must disclose such information only to authorized individuals, such as the injured employee or relevant safety agencies.
What should an employer do if an employee dies as a result of an injury?
If an employee dies as a result of a previously reported injury, the employer must file an amended report within five days of becoming aware of the death. This report must include all relevant details surrounding the incident and any additional information required for compliance with workers' compensation regulations.
Can the SCIF E3067 form be used for non-work-related injuries?
No, the SCIF E3067 form is specifically intended for reporting occupational injuries or illnesses that occur in the course of employment. Non-work-related injuries or illnesses should not be reported using this form, as it is designed solely for workplace incidents that impact employee work performance or require medical attention.
Common mistakes
When filling out the SCIF E3067 form, mistakes can lead to delays or complications in the claims process. One common error is missing critical information, such as the firm name or policy number. Completing all sections accurately is essential, as incomplete submissions can result in a rejection. Employers must ensure that they provide clear and correct details to avoid additional work.
Another frequent mistake is incorrectly stating the date of injury or onset of illness. It is crucial to enter the correct date to establish the timeline of the injury. Errors in this area may create confusion and complicate the claims process.
Many people overlook the specific injury or illness and medical diagnosis section. Providing a precise description of the incident can help medical professionals offer appropriate care. Leaving this blank could hinder treatment and affect claims validation.
Failing to indicate whether the employee was hospitalized is a vital mistake. This information plays an essential role in the claims process. If yes, the details regarding the hospital must also be included. Inaccurate reporting can impact workers’ compensation benefits.
Providing the wrong body parts affected can further complicate matters. Ensure the information aligns with medical reports or observations from the incident. This precision not only aids in medical treatment but also strengthens the claim's reliability.
Not specifying the sequence of events surrounding the injury is another error that can lead to problems. A clear narrative helps to illustrate how the injury occurred. Detailing this ensures that every aspect is communicated effectively.
Another common oversight is neglecting to fill out the date of the employer's knowledge of the injury. This date is crucial as it marks the timeline for reporting obligations. Failing to include it may delay necessary actions.
When listing the employees affected in the event, ensure accuracy. Missing this information can cause confusion and limit the investigation into workplace safety issues. Be precise and thorough in documenting all related employees.
Incorrectly filling out the employee’s employment status and classification is another mistake. Clarifying whether an employee is full-time, part-time, or temporary is critical for assessing eligibility for benefits. Wrong information here can lead to complications regarding the claim.
Lastly, missing the signature and title of the person completing the form is a significant oversight. This step verifies the submission and confirms that the information is accurate. Without it, the document may face delays or rejections. Always ensure that the form is complete before submission.
Documents used along the form
When dealing with occupational injuries or illnesses in California, several forms and documents are essential in addition to the Scif E3067 form. These documents help ensure that proper procedures are followed, and they facilitate timely communication between employers, employees, and insurance providers. Below are some commonly used forms that accompany the Scif E3067.
- Workers' Compensation Claim Form (DWC 1): This form is essential for initiating a workers' compensation claim. It allows injured employees to report their injury and seek benefits such as medical care and wage replacement.
- Employer's Report of Injury or Illness (Form 5020): Employers use this document to report occupational injuries or illnesses to their workers' compensation insurance carrier. It contains critical details about the incident and is usually required within a specific timeframe following an injury.
- Medical Provider's Report (Form 5021): This form serves as communication between the medical provider and the employer or insurance carrier. It documents the employee's medical findings and treatment recommendations following the injury.
- Return to Work Certification: After treatment, this document must be completed by a physician to certify whether an employee is fit to return to work. It indicates any restrictions or required accommodations that may be necessary for the employee's safe reinstatement.
Completing these forms accurately and in a timely manner is crucial for all parties involved. Employers should remain aware of their obligations to report and respond to workplace injuries, ensuring clear communication with employees about their rights and the processes in place. By adhering to these requirements, both employers and employees can navigate the complexities of workplace injury management more effectively.
Similar forms
- First Report of Injury (FROI): Similar to the SCIF E3067 form, the FROI serves as an initial report detailing an employee's work-related injury or illness. It includes essential information about the incident, such as the time and place of the injury, the nature of the injury, and the employee’s work status.
- Employee Claim Form (DWC-1): This form allows employees to formally initiate their workers' compensation claim. It includes personal details, a description of the injury, and the nature of the medical treatment sought, similarly capturing critical information relevant to the incident.
- OSHA 300 Log: This log records work-related injuries and illnesses as mandated by the Occupational Safety and Health Administration. Like the SCIF E3067, it must be updated within a specified time period following an incident.
- Incident Report: An internal document generated by employers to detail the circumstances surrounding a workplace accident. This report may be similar in terms of documenting the specifics of the injury or illness and the events leading to it.
- Return to Work Form: Used to assess an injured employee's ability to return to work. This document includes details about any work restrictions and is connected to the recovery process, much like the follow-up information collected in the SCIF E3067.
- Medical Report: A document completed by a healthcare provider that outlines the diagnosis and treatment plan for an injured employee. It shares the same purpose of providing crucial medical information relevant to the nature of the injury.
- Workplace Injury Investigation Report: This report is generated after an investigation into workplace incidents. It examines the causes of the incident, similar to the descriptive sequence of events required in the SCIF E3067 form.
- Compensation Agreement: An agreement detailing the benefits and compensation for an injured employee. It encompasses the outcomes of the claims process, paralleling the SCIF E3067's role in reporting initial information about an incident.
- Blanket Claim Form: Used by employers to report multiple injuries or illnesses occurring within a specified timeframe. Similar to the SCIF E3067, it captures comprehensive information about each incident and the affected individuals.
Dos and Don'ts
When filling out the SCIF E3067 form, attention to detail is crucial. Here’s a guide on what to do and what to avoid.
- Do provide accurate and complete information in each section.
- Do report the injury within five days of learning about it.
- Do include a clear description of the injury or illness process and any relevant medical diagnosis.
- Do check all applicable boxes, ensuring that no important question is left unanswered.
- Don't use abbreviations or initials; always provide full names and job titles.
- Don't omit medical or hospital details if treatment was received, as this information is essential for processing the claim.
Misconceptions
- Misconception 1: The SCIF E3067 form only needs to be filed if an employee is seriously injured.
- Misconception 2: The form must be submitted immediately after an injury occurs.
- Misconception 3: Submitting the SCIF E3067 form is an admission of liability.
- Misconception 4: Only full-time employees are covered under this reporting requirement.
This is incorrect. Employers must file this form for any occupational injury or illness that results in lost time beyond the incident date or requires medical treatment beyond first aid.
While timely reporting is crucial, employers have up to five days from the date of knowledge about the injury or illness to file the form. Immediate reporting applies for serious injuries or fatalities, which must be reported without delay.
This is false. The filing of this report does not imply that the employer accepts liability for the injury or illness. It's simply a documentation requirement to facilitate the claims process.
This misconception overlooks the fact that all employees, regardless of their status—full-time, part-time, or temporary—are covered for occupational injuries or illnesses. Employers must report injuries for all employees.
Key takeaways
Filling out the SCIF E3067 form accurately is essential for effective reporting of occupational injuries or illnesses. Below are key takeaways to keep in mind:
- Timeliness is Crucial: Employers must report occupational injuries or illnesses within five days of becoming aware of the event, especially if it results in lost workdays or requires medical treatment beyond first aid.
- Immediate Reporting for Serious Cases: All serious injuries, illnesses, or fatalities need immediate notification to the California Division of Occupational Safety and Health.
- Complete All Required Fields: Pay special attention to fields such as the date of injury, specific injury details, and the employee's information to ensure a comprehensive report.
- Confidentiality Matters: This form contains sensitive employee health information. Use it responsibly and maintain confidentiality according to relevant regulations.
- Provide a Claim Form: Within one working day of knowing about the injury or illness, make sure to provide the injured employee with a claim form.
- Accurate Descriptions Help: Clearly describe the sequence of events that led to the injury or illness, including specifics such as the activity performed and equipment used.
- Seek Support When Needed: For any uncertainties while filling out the form, don’t hesitate to consult with a supervisor or legal counsel to clarify procedures.
Employing these guidelines ensures compliance and aids in the proper management of occupational safety and health concerns in the workplace.
Browse Other Templates
How to Change My Name on My Cna License - Candidates can check certificate status via a designated online link.
How Long Do You Have to File Workers Comp - Every completed form serves as a critical piece of the workers' compensation claim process.