Fill Out Your Soc 821 Form
The SOC 821 form is a critical tool within California's In-Home Supportive Services (IHSS) program, designed to assess an individual's need for Protective Supervision. This form is integral for ensuring that vulnerable populations, particularly those who are non self-directing, mentally impaired, or mentally ill, receive the supervision necessary to protect them from potential hazards. It serves as a structured mechanism for medical professionals to express their assessments regarding the patient’s memory, orientation, and judgment. By detailing specific aspects of the patient’s mental state and condition, the SOC 821 enables counties to make informed decisions about eligibility for supervision services. The form emphasizes what Protective Supervision encompasses — monitoring and observing behaviors that might lead to accidents — while clearly delineating scenarios where this service cannot be provided. For example, it cannot be utilized in instances where the need arises strictly from physical conditions, medical emergencies, or social activities. Completing this form requires a thorough understanding from the medical professional of the patient’s current cognitive state, which includes evaluating any prior injuries related to cognitive deficits. By requiring detailed explanations and specific checkboxes regarding cognitive impairments, the form ensures a comprehensive approach to patient assessment. It underscores the urgency of timely completion and submission, as delays could hinder vital services for the individuals who depend on them.
Soc 821 Example

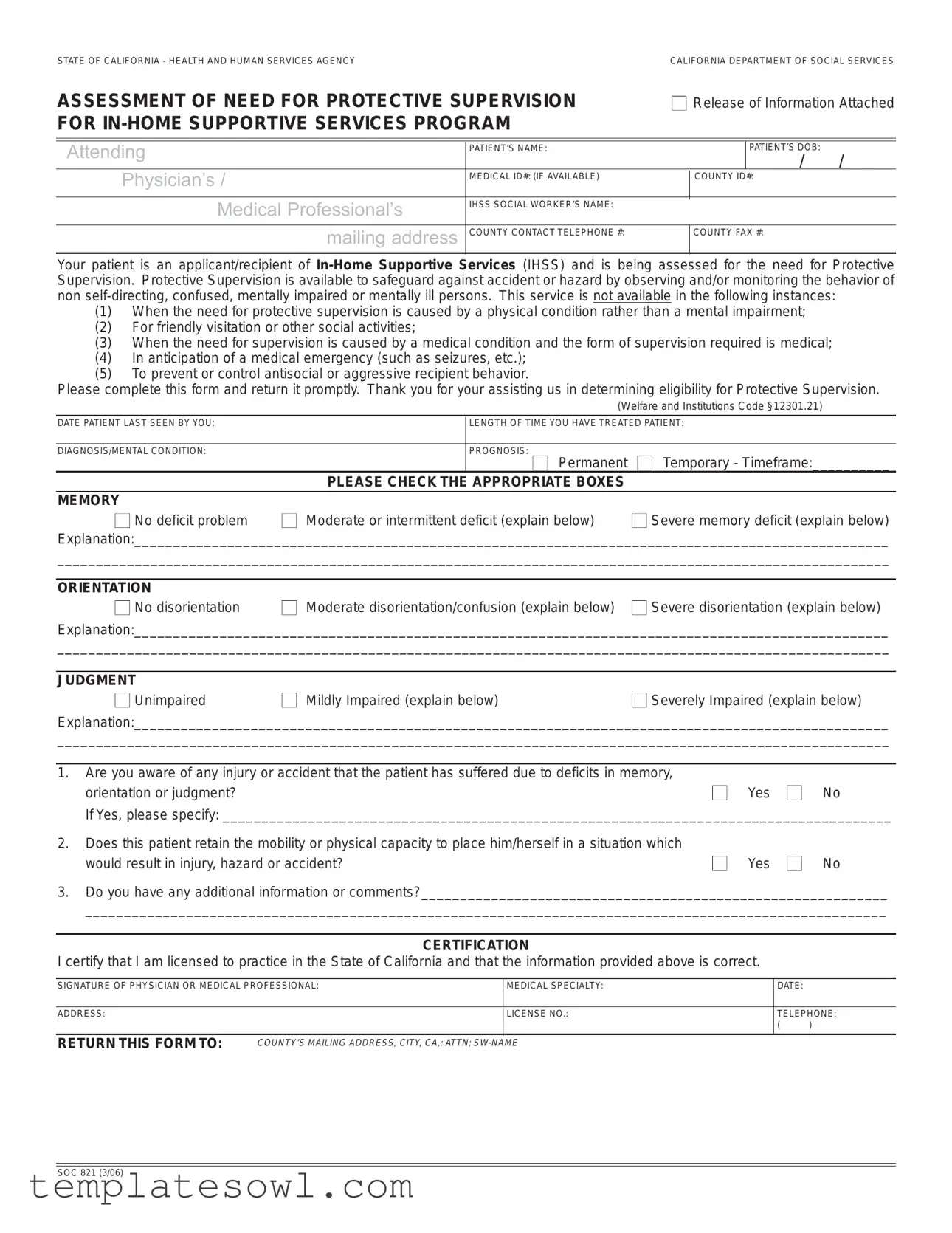
STATE OF CALIFORNIA - HEALTH AND HUMAN SERVICES AGENCYCALIFORNIA DEPARTMENT OF SOCIAL SERVICES
ASSESSMENT OF NEED FOR PROTECTIVE SUPERVISION |
■ Release of Information Attached |
|||||
FOR |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Attending |
|
|
PATIENT’S NAME: |
|
|
PATIENT’S DOB: |
|
|
|
|
|
|
/ / |
Physician’s / |
|
MEDICAL ID#: (IF AVAILABLE) |
|
COUNTY ID#: |
||
|
|
|
|
|||
|
|
|
|
|
|
|
|
Medical Professional’s |
IHSS SOCIAL WORKER’S NAME: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
mailing address |
COUNTY CONTACT TELEPHONE #: |
|
COUNTY FAX #: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Your patient is an applicant/recipient of
(1)When the need for protective supervision is caused by a physical condition rather than a mental impairment;
(2)For friendly visitation or other social activities;
(3)When the need for supervision is caused by a medical condition and the form of supervision required is medical;
(4)In anticipation of a medical emergency (such as seizures, etc.);
(5)To prevent or control antisocial or aggressive recipient behavior.
Please complete this form and return it promptly. Thank you for your assisting us in determining eligibility for Protective Supervision.
(Welfare and Institutions Code §12301.21)
DATE PATIENT LAST SEEN BY YOU: |
|
LENGTH OF TIME YOU HAVE TREATED PATIENT: |
|
|
|
|
|
DIAGNOSIS/MENTAL CONDITION: |
|
PROGNOSIS: ■ Permanent |
■ Temporary - Timeframe:__________ |
|
PLEASE CHECK THE APPROPRIATE BOXES |
|
|
MEMORY |
|
|
|
■ No deficit problem |
■ Moderate or intermittent deficit (explain below) |
■ Severe memory deficit (explain below) |
|
Explanation:_________________________________________________________________________________________________
___________________________________________________________________________________________________________
ORIENTATION |
|
■ No disorientation |
■ Moderate disorientation/confusion (explain below) ■ Severe disorientation (explain below) |
Explanation:_________________________________________________________________________________________________
___________________________________________________________________________________________________________
JUDGMENT |
|
|
■ Unimpaired |
■ Mildly Impaired (explain below) |
■ Severely Impaired (explain below) |
Explanation:_________________________________________________________________________________________________
___________________________________________________________________________________________________________
1.Are you aware of any injury or accident that the patient has suffered due to deficits in memory,
orientation or judgment?■ Yes ■ No
If Yes, please specify: ______________________________________________________________________________________
2.Does this patient retain the mobility or physical capacity to place him/herself in a situation which
would result in injury, hazard or accident? |
■ |
Yes ■ |
No |
3.Do you have any additional information or comments?____________________________________________________________
_______________________________________________________________________________________________________
CERTIFICATION
I certify that I am licensed to practice in the State of California and that the information provided above is correct.
SIGNATURE OF PHYSICIAN OR MEDICAL PROFESSIONAL: |
MEDICAL SPECIALTY: |
DATE: |
|
|
|
|
|
ADDRESS: |
LICENSE NO.: |
TELEPHONE: |
|
|
|
( |
) |
|
|
|
|
RETURN THIS FORM TO:
COUNTY’S MAILING ADDRESS, CITY, CA,: ATTN;
SOC 821 (3/06)
Form Characteristics
| Fact Name | Details |
|---|---|
| Purpose | The SOC 821 form assesses the need for Protective Supervision under the In-Home Supportive Services (IHSS) Program in California. |
| Eligibility | Protective Supervision is for individuals who are non self-directing, confused, mentally impaired, or mentally ill. |
| Exclusions | The service is not available for needs arising from physical conditions or for social activities, among other specified instances. |
| Governing Law | This form is governed by the Welfare and Institutions Code §12301.21 in California. |
| Medical Certification | A medical professional must certify the information provided on the form and confirm they are licensed in California. |
| Required Information | Details such as the patient’s name, diagnosis, and assessments of memory, orientation, and judgment are needed on the form. |
Guidelines on Utilizing Soc 821
Filling out the SOC 821 form is an important step in helping an individual apply for Protective Supervision through the In-Home Supportive Services (IHSS) Program. Properly completing this form will ensure a smoother review process by the county’s social services department. Below are the essential steps to guide you through the process.
- Gather necessary information: Before you start, collect the patient’s name, date of birth, medical ID (if available), and county ID.
- Fill in the attending physician or medical professional's details: Write down their name, mailing address, county contact telephone number, and fax number.
- Indicate the date the patient was last seen by you. This will provide the necessary context for the evaluation.
- Document the length of time you have treated the patient. This information helps establish your relationship and understanding of the patient’s condition.
- Specify the patient's diagnosis or mental condition clearly. Accurate information here is crucial.
- State the prognosis: Check either "Permanent" or "Temporary," and if temporary, provide a timeframe if known.
- Assess the patient’s memory: Check the appropriate box regarding their memory deficit and provide any necessary explanations.
- Evaluate the patient’s orientation: Again, select the appropriate designation and add any required explanations.
- Assess the patient’s judgment similarly, providing a selection and explanations where needed.
- Answer the two questions regarding the patient's risk of injury due to memory, orientation, or judgment deficits. Be detailed in your responses if you answer "Yes."
- If there are additional comments or information that could aid the assessment, include those in the specified section.
- Certify the form: The licensed physician or medical professional must sign, date, and provide their medical specialty, license number, and telephone number.
- Submit the completed form to the county's mailing address as indicated, ensuring it is directed to the attention of the assigned social worker by including the correct name.
After completing these steps, ensure that all information is accurate and legible. Timely submission of this form is crucial. This will help the patient receive the necessary assessment and support as soon as possible.
What You Should Know About This Form
1. What is the purpose of the SOC 821 form?
The SOC 821 form is used in California's In-Home Supportive Services (IHSS) program to assess the need for Protective Supervision for applicants and recipients. This service helps safeguard individuals who are non self-directing, confused, mentally impaired, or mentally ill by observing or monitoring their behavior.
2. Who is qualified to complete the SOC 821 form?
A licensed physician or medical professional must complete the SOC 821 form. This ensures that the information provided is accurate and credible for determining the patient’s eligibility for Protective Supervision.
3. What types of situations does Protective Supervision cover?
Protective Supervision is intended for individuals whose need arises from mental impairments, confusion, or related conditions. It does not cover cases where supervision is needed due to physical conditions, for social visits, or in anticipation of medical emergencies.
4. What information is required on the SOC 821 form?
The form requires details such as the patient’s name, date of birth, medical ID, diagnosis, prognosis, and assessments of memory, orientation, and judgment. The physician must also provide their signature and details of their medical specialty.
5. How does one determine if a patient qualifies for Protective Supervision?
To qualify for Protective Supervision, the physician must evaluate the patient's mental condition and the level of deficit in memory, orientation, and judgment. Documented injuries or accidents related to these deficits support the need for supervision.
6. Is there a specific time frame for the need for Protective Supervision?
Yes, the prognosis can be classified as either permanent or temporary. If temporary, the physician should indicate the expected timeframe for the patient's need for supervision.
7. What should be done if the physician has additional comments?
The physician should use the designated section on the SOC 821 form to provide any additional comments or relevant information that may assist in the assessment process.
8. How should the completed SOC 821 form be submitted?
The completed form must be returned promptly to the appropriate county mailing address listed at the bottom of the SOC 821 form. It should be addressed to the designated social worker.
9. What if the patient does not have a medical ID number?
If the patient does not have a medical ID number, the physician can leave that section blank. However, providing any other identifying information available is encouraged to assist with the processing of the application.
10. Can the SOC 821 form be used for patients who exhibit aggressive behavior?
No, the SOC 821 form does not apply to those whose need for supervision is primarily to control aggressive or antisocial behavior. Protective Supervision is meant to address deficits in mental capacity that lead to potential accidents or hazards.
Common mistakes
Filling out the SOC 821 form can be challenging, and many people make mistakes that can delay the process. One common error is leaving out critical information about the patient's diagnosis or medical condition. Incomplete data can hinder the assessment of eligibility for Protective Supervision, leading to further complications.
Another frequent mistake is failing to specify the patient’s date of birth. This information is essential for proper identification. Omitting the patient's date of birth could cause confusion and result in delays in processing the application.
Some applicants forget to provide the length of time they have treated the patient. This detail offers context about the medical professional's familiarity with the patient's condition. Without it, the evaluator may question the validity of the assessment.
It's also important to accurately assess the patient's memory and orientation. Some people mistakenly check “No deficit problem” when there’s evidence of impairment. Be precise in evaluating the patient’s abilities to ensure that the correct support is granted.
Confusion often arises around the certification section. Many individuals overlook signing the form or do not include their license number. This omission can render the document incomplete and may lead to rejection.
Providing vague explanations can lead to misunderstandings. If you select a level of impairment in memory, orientation, or judgment, be specific in your explanation. Failing to provide adequate details can compromise the assessment process.
When asked whether the patient retains mobility or physical capacity, some respondents answer without considering the situation fully. It’s crucial to think critically about this question, as an incorrect answer could risk the patient’s safety.
Neglecting to attach the release of information documents is another common issue. This attachment is vital for protecting patient confidentiality while allowing for the sharing of necessary information. Failing to submit it can stall the entire evaluation.
Sometimes individuals forget to return the form to the correct mailing address. Always verify the county's address and ensure that the document reaches the right department. Misaddressing can lead to further holds on the application.
Lastly, failing to keep a copy of the submitted form is a mistake that some make. Retaining a copy is essential for tracking your application and any future communications regarding the assessment. It serves as a record that can clarify discrepancies later on.
Documents used along the form
When assessing the need for Protective Supervision within the In-Home Supportive Services (IHSS) Program, the SOC 821 form is just one piece of the puzzle. There are several other important documents and forms that work in conjunction with it. Understanding these can help streamline the process and ensure that the necessary information is provided for effective decision-making.
- SOC 873: This is the Application for In-Home Supportive Services. It gathers essential information about the applicant's financial situation and personal details. Completing this application correctly is crucial for determining eligibility for the program.
- IHSS Provider Enrollment Form: This form is filled out by individuals wishing to become providers for IHSS recipients. It includes personal information and verification of qualifications, ensuring that only suitable candidates are approved to provide in-home care.
- Physician’s Statement for Protective Supervision: Sometimes required along with the SOC 821, this document details the medical professional's observations and supporting information regarding the individual’s need for protective supervision. It serves to back up the claims made in the SOC 821 form.
- Notice of Action: Once an application is reviewed, a Notice of Action may be issued to inform the applicant of the decision regarding their IHSS eligibility. This document provides crucial information that helps the recipient understand their rights and options moving forward.
- Service Plan: This document outlines the specific services and support that will be provided to the recipient once approved for IHSS. It details how these services will be delivered and helps establish clear expectations for both the provider and the recipient.
By being familiar with these additional documents, applicants and caregivers can more effectively navigate the process of obtaining the necessary supports. Each form plays a unique role, contributing to a comprehensive understanding of the recipient’s needs and ensuring that proper care is administered.
Similar forms
The SOC 821 form serves a specific purpose within California's In-Home Supportive Services (IHSS) Program, primarily focusing on assessing the need for Protective Supervision. However, it resembles several other important documents related to medical assessments and social services. Below are four forms that share similar characteristics with the SOC 821:
- State Medical Examination Form: This form requires health professionals to provide detailed information about a patient's physical and mental health conditions. Both documents emphasize the need for clear certification from a licensed practitioner to ensure accurate assessments.
- Functional Assessment Form: Used in many social service programs, this form gathers comprehensive data about an individual's daily living abilities. Like the SOC 821, it aims to evaluate the support needs of individuals, considering both their cognitive and physical capabilities.
- Disability Assessment Report: This report documents the extent of a person's disability, including mental impairments. Similar to the SOC 821, it requires detailed input from medical professionals and stresses the importance of understanding a patient’s limitations to determine eligibility for services.
- Caregiver Assessment Form: This form assesses the suitability of caregivers for individuals needing assistance. Both the SOC 821 and caregiver assessment focus on ensuring the safety and wellbeing of vulnerable populations, addressing potential risks and required oversight.
Each of these documents plays a crucial role in ensuring that individuals receive appropriate care and supports. They collectively contribute to the broader framework of health and social services, ensuring comprehensive evaluations that prioritize patient safety and needs.
Dos and Don'ts
Filling out the Soc 821 form correctly is crucial for the assessment of an applicant's need for Protective Supervision under the In-Home Supportive Services program. Here’s a guide on what you should and shouldn’t do while completing this important document.
- Do ensure that all sections are filled out completely. Omissions can delay the process.
- Do provide clear and thorough explanations for any deficits noted in memory, orientation, or judgment.
- Do sign and date the form, certifying the accuracy of the information.
- Do check the patient's medical history for any injuries related to deficits, and provide specific details if applicable.
- Don't use medical jargon that may confuse the assessment team. Clarity is key.
- Don't forget to return the form promptly to the correct county mailing address indicated at the bottom.
By following these guidelines, you contribute significantly to a more effective assessment process while supporting your patient's eligibility for vital services.
Misconceptions
Understanding the SOC 821 form can be challenging due to various misconceptions surrounding it. Here are ten common myths and the truths that clarify them:
- Protective supervision is the same as regular supervision. Many believe that both terms are interchangeable. However, protective supervision specifically caters to individuals who are non self-directing or mentally impaired.
- This form is required for all IHSS applicants. Not every applicant needs to fill out the SOC 821. It is only necessary when assessing eligibility for protective supervision services.
- It covers individuals with physical conditions. The SOC 821 is designed for those with mental impairments. If a person’s need for supervision arises solely from physical health issues, this form does not apply.
- Completion of this form guarantees service approval. Submitting the SOC 821 does not automatically mean the recipient will be granted protective supervision. Each case undergoes a further review process.
- Protective supervision is available for social activities. This service is not intended for friendly visits or non-essential social interactions. It focuses on safety and prevention of hazards for vulnerable individuals.
- Medical emergencies can be addressed with this supervision. The form is not applicable for anticipating medical emergencies, such as seizures. Such situations require different types of medical support.
- Information on the SOC 821 is optional. Providing detailed information about the individual’s condition and needs on the form is crucial. Incomplete forms may delay the assessment process.
- The physician’s signature is not necessary. The SOC 821 must be signed by a licensed physician or medical professional, verifying that the information is accurate. This ensures accountability.
- Family members can fill out the form without professional input. The SOC 821 requires input from a qualified medical professional. Family members cannot complete this assessment without their involvement.
- Once submitted, the form can’t be updated. Changes can be made if new information becomes available. It’s important to communicate any updates that may influence the assessment of protective supervision.
By debunking these misconceptions, individuals seeking assistance can better understand the SOC 821’s purpose and the role it plays in the In-Home Supportive Services Program.
Key takeaways
Filling out and using the SOC 821 form requires attention to detail and an understanding of the patient's needs. Here are some key takeaways to keep in mind:
- This form is specifically designed for assessing the need for Protective Supervision under the In-Home Supportive Services (IHSS) program in California.
- Be sure to provide accurate patient information, including the patient's name, date of birth, and any identification numbers.
- The form needs to be completed by a qualified medical professional who can discuss the patient's mental and cognitive status.
- Clearly indicate the diagnosis and any mental conditions that may affect the patient's ability to care for themselves. This information is crucial for determining the eligibility for services.
- The patient's memory, orientation, and judgment should be assessed. Carefully evaluate and check the appropriate boxes for deficits related to each category.
- Provide detailed explanations wherever deficits are noted. This helps clarify the patient's condition and supports the request for Protective Supervision.
- Answer the specific questions about the patient's safety and past incidents, as this information will assist in evaluating their need for supervision.
- Certification must be completed by a licensed medical professional, affirming that the provided information is accurate.
- Submit the form promptly to the designated county mailing address to avoid delays in the evaluation process.
By following these points, you can ensure that the SOC 821 form is filled out correctly and expedites the assessment for your patient. This process plays an important role in securing much-needed support for individuals facing cognitive challenges.
Browse Other Templates
VA Education Benefits Application,VA Educational Assistance Form,VA Benefits Application Form,VA Training Benefits Request,Veterans Education Benefits Application,Application for Military Education Assistance,Educational Benefits Enrollment Form,GI B - Make sure to review the overview of programs provided in the form before deciding which one suits your situation best.
Ds 160 Appointment - Applicants need to specify their primary MOS/AOC on the form.