Fill Out Your Tennessee First Report Form
When an employee experiences a work-related injury or illness in Tennessee, the Tennessee First Report form plays a critical role in documenting the details and initiating the workers' compensation claims process. This form is essential for employers, as it must be completed and submitted to the insurance carrier immediately following notice of the injury, particularly for claims related to medical-only injuries or those resulting in lost time from work. The First Report form collects vital information, including the individual’s personal details, employment status, and specifics related to the injury, such as the date, time, and nature of the incident. Additionally, it requires descriptions of how the injury occurred, the body parts affected, and the treatment the employee received or will require. Notably, there are strict legal implications associated with this form; knowingly providing false or misleading information can result in serious consequences, including criminal charges and denial of claims benefits. Understanding how to accurately fill out the Tennessee First Report form is essential for employers to ensure compliance and protect the rights of injured employees. By adhering to the requirements outlined in this document, employers can facilitate a smoother claims process and better support their workforce during challenging times.
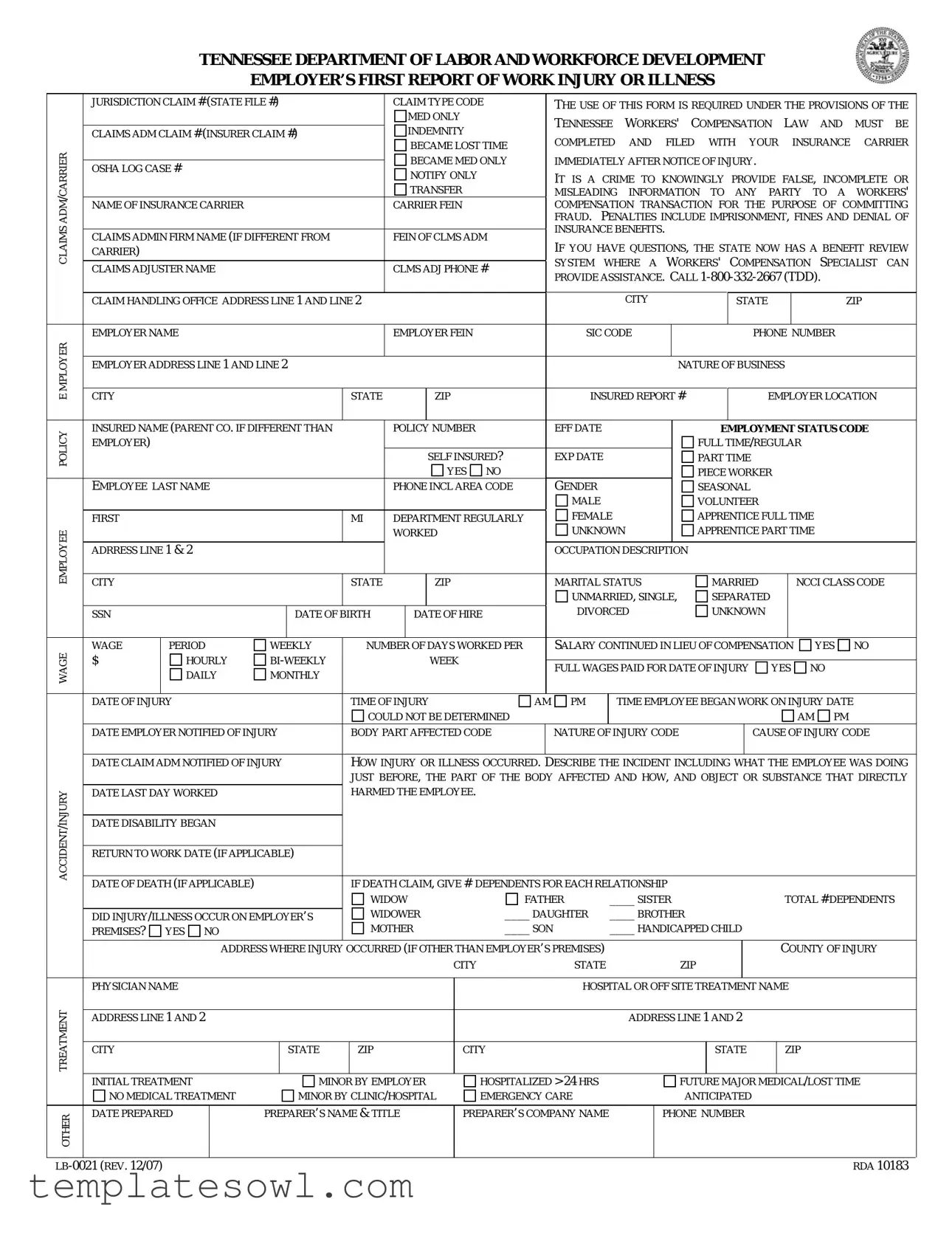
Tennessee First Report Example
TENNESSEE DEPARTMENT OF LABOR AND WORKFORCE DEVELOPMENT
EMPLOYER’S FIRST REPORT OF WORK INJURY OR ILLNESS
|
JURISDICTION CLAIM # (STATE FILE #) |
|
|
|
CLAIM TYPE CODE |
|
THE USE OF THIS FORM IS REQUIRED UNDER THE PROVISIONS OF THE |
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
MED ONLY |
|
|
TENNESSEE |
WORKERS' |
|
COMPENSATION |
LAW |
AND |
MUST |
BE |
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
INDEMNITY |
|
|
|
|||||||||||||||||||||
|
CLAIMS ADM CLAIM # (INSURER CLAIM #) |
|
|
|
|
|
||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
COMPLETED |
AND |
FILED WITH |
YOUR |
|
|
INSURANCE |
CARRIER |
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
BECAME LOST TIME |
|
|
|
|||||||||||||||||||||
CARRIER |
|
|
|
|
|
|
|
|
|
|
|
|
IT IS A CRIME TO KNOWINGLY PROVIDE FALSE, INCOMPLETE OR |
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
TRANSFER |
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
BECAME MED ONLY |
|
IMMEDIATELY AFTER NOTICE OF INJURY. |
|
|
|
|
|
|
||||||||||||||||
|
OSHA LOG CASE # |
|
|
|
|
|
|
|
NOTIFY ONLY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MISLEADING INFORMATION TO ANY PARTY TO A WORKERS' |
|||||||||||||||||||
ADM |
NAME OF INSURANCE CARRIER |
|
|
|
|
|
|
CARRIER FEIN |
|
|
COMPENSATION TRANSACTION FOR THE PURPOSE OF COMMITTING |
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FRAUD. |
PENALTIES INCLUDE IMPRISONMENT, FINES AND DENIAL OF |
|||||||||||||||||||
CLAIMS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
INSURANCE BENEFITS. |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
CLAIMS ADMIN FIRM NAME (IF DIFFERENT FROM |
|
|
|
FEIN OF CLMS ADM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
IF YOU HAVE QUESTIONS, THE STATE NOW HAS A BENEFIT REVIEW |
||||||||||||||||||||||||||||||||
|
|
|
|
|
||||||||||||||||||||||||||||||||
|
CARRIER) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SYSTEM |
WHERE A |
WORKERS' COMPENSATION |
SPECIALIST |
CAN |
|||||||||||||||
|
CLAIMS ADJUSTER NAME |
|
|
|
|
|
|
CLMS ADJ PHONE # |
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
PROVIDE ASSISTANCE. CALL |
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CITY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
CLAIM HANDLING OFFICE ADDRESS LINE 1 AND LINE 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
STATE |
|
|
|
ZIP |
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
EMPLOYER NAME |
|
|
|
|
|
|
EMPLOYER FEIN |
|
|
SIC CODE |
|
|
|
|
|
|
|
PHONE NUMBER |
|
|
|||||||||||||||
MPLOYERE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
CITY |
|
|
|
|
|
|
STATE |
ZIP |
|
|
INSURED REPORT # |
EMPLOYER LOCATION |
|
|||||||||||||||||||||||
|
EMPLOYER ADDRESS LINE 1 AND LINE 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NATURE OF BUSINESS |
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
POLICY |
INSURED NAME (PARENT CO. IF DIFFERENT THAN |
|
|
|
POLICY NUMBER |
|
EFF DATE |
|
|
|
|
|
|
EMPLOYMENT STATUS CODE |
|
|||||||||||||||||||||
EMPLOYER) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FULL TIME/REGULAR |
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
SELF INSURED? |
|
EXP DATE |
|
|
|
|
|
PART TIME |
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
YES |
NO |
|
GENDER |
|
|
|
|
|
|
|
PIECE WORKER |
|
|
|
|
|
|
||||||
|
EMPLOYEE LAST NAME |
|
|
|
|
|
|
PHONE INCL AREA CODE |
|
|
|
|
|
|
|
|
SEASONAL |
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MALE |
|
|
|
|
|
|
|
VOLUNTEER |
|
|
|
|
|
|
|||||
|
FIRST |
|
|
|
|
|
|
MI |
|
DEPARTMENT REGULARLY |
|
FEMALE |
|
|
|
|
|
APPRENTICE FULL TIME |
|
|
|
|||||||||||||||
EMPLOYEE |
|
|
|
|
|
|
|
|
|
|
WORKED |
|
|
UNKNOWN |
|
|
|
APPRENTICE PART TIME |
|
|
|
|||||||||||||||
ADRRESS LINE 1 & 2 |
|
|
|
|
|
|
|
|
|
|
|
|
OCCUPATION DESCRIPTION |
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
CITY |
|
|
|
|
|
|
STATE |
ZIP |
|
|
MARITAL STATUS |
|
|
|
|
MARRIED |
|
|
NCCI CLASS CODE |
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
UNMARRIED, SINGLE, |
|
|
SEPARATED |
|
|
|
|
|
|
||||||||||
|
SSN |
|
|
|
|
DATE OF BIRTH |
|
|
DATE OF HIRE |
|
DIVORCED |
|
|
|
|
UNKNOWN |
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
WAGE |
WAGE |
|
PERIOD |
WEEKLY |
|
NUMBER OF DAYS WORKED PER |
|
SALARY CONTINUED IN LIEU OF COMPENSATION |
|
YES |
NO |
|
||||||||||||||||||||||||
$ |
|
HOURLY |
|
|
|
|
|
WEEK |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
FULL WAGES PAID FOR DATE OF INJURY |
YES NO |
|
|
||||||||||||||||||||||||
|
|
|
DAILY |
MONTHLY |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
DATE OF INJURY |
|
|
|
|
TIME OF INJURY |
|
AM PM |
|
|
TIME EMPLOYEE BEGAN WORK ON INJURY DATE |
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
COULD NOT BE DETERMINED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
AM |
PM |
|
|
||||||
|
DATE EMPLOYER NOTIFIED OF INJURY |
|
BODY PART AFFECTED CODE |
|
NATURE OF INJURY CODE |
|
|
|
|
|
CAUSE OF INJURY CODE |
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
DATE CLAIM ADM NOTIFIED OF INJURY |
|
HOW INJURY OR ILLNESS OCCURRED. |
DESCRIBE THE INCIDENT INCLUDING WHAT THE EMPLOYEE WAS DOING |
||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
JUST BEFORE, THE PART OF THE BODY AFFECTED AND HOW, AND OBJECT OR SUBSTANCE THAT DIRECTLY |
|||||||||||||||||||||||||||
INJURY |
DATE LAST DAY WORKED |
|
|
|
|
HARMED THE EMPLOYEE. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DATE DISABILITY BEGAN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
ACCIDENT/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RETURN TO WORK DATE (IF APPLICABLE) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
IF DEATH CLAIM, GIVE # |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
DATE OF DEATH (IF APPLICABLE) |
|
|
|
DEPENDENTS FOR EACH RELATIONSHIP |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
WIDOW |
|
|
|
FATHER |
|
____ SISTER |
|
|
|
|
|
|
|
TOTAL # DEPENDENTS |
||||||||||||
|
|
|
|
|
|
WIDOWER |
|
|
____ DAUGHTER |
|
____ BROTHER |
|
|
|
|
|
|
|
|
|||||||||||||||||
|
DID INJURY/ILLNESS OCCUR ON EMPLOYER’S |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
PREMISES? |
YES NO |
|
|
|
|
|
MOTHER |
|
|
____ SON |
|
____ HANDICAPPED CHILD |
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
ADDRESS WHERE INJURY |
OCCURRED (IF OTHER THAN EMPLOYER’S PREMISES) |
|
|
|
|
|
|
|
|
|
|
|
COUNTY OF INJURY |
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
CITY |
|
STATE |
|
|
|
|
ZIP |
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
PHYSICIAN NAME |
|
|
|
|
|
|
|
|
|
|
|
|
HOSPITAL OR OFF SITE TREATMENT NAME |
|
|
|
|||||||||||||||||||
TREATMENT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ADDRESS LINE 1 AND 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ADDRESS LINE 1 AND 2 |
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
CITY |
|
|
|
|
STATE |
|
ZIP |
|
CITY |
|
|
|
|
|
|
|
|
|
|
STATE |
|
|
ZIP |
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
INITIAL TREATMENT |
|
|
MINOR BY EMPLOYER |
|
|
HOSPITALIZED > 24 HRS |
|
|
|
|
|
|
FUTURE MAJOR MEDICAL/LOST TIME |
|
|||||||||||||||||||||
|
NO MEDICAL TREATMENT |
|
|
MINOR BY CLINIC/HOSPITAL |
EMERGENCY CARE |
|
|
|
|
|
|
ANTICIPATED |
|
|
|
|
|
|
||||||||||||||||||
OTHER |
DATE PREPARED |
|
PREPARER’S NAME & TITLE |
|
PREPARER’S COMPANY NAME |
|
|
PHONE NUMBER |
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RDA 10183 |
||||
Form Characteristics
| Fact Name | Details |
|---|---|
| Governing Law | The Tennessee First Report form is governed by the Tennessee Workers' Compensation Law. |
| Mandatory Use | This form must be completed and filed with the insurance carrier immediately after notice of an injury. |
| Legal Consequences | Providing false or misleading information is considered a crime, leading to potential fines, imprisonment, or denial of claims. |
| Assistance Available | A Benefit Review System is accessible for support, allowing employers and employees to consult with a Workers' Compensation Specialist by calling 1-800-332-2667. |
Guidelines on Utilizing Tennessee First Report
Completing the Tennessee First Report form is a crucial step in reporting an employee’s work-related injury or illness. When filling out this form, it's important to provide accurate and thorough information to ensure a seamless processing of the claim. Below are the detailed steps to assist you in accurately completing the form.
- Begin by entering the Claim Number and the Claim Type Code at the top of the form.
- Provide the Name of Insurance Carrier and the corresponding FEIN.
- If applicable, fill in the Claims Adjuster Name and Phone Number.
- Enter your Employer Name, FEIN, SIC Code, and Phone Number.
- Fill in the Employer Location and Employer Address lines.
- Describe the Nature of Business and provide the Policy Number and Effective Date.
- Select the Employment Status Code that applies (Full Time, Part Time, Seasonal, etc.).
- Complete the employee's information, including Last Name, First Name, Middle Initial, Date of Birth, and Social Security Number.
- Specify the employee's Gender, Department, and Occupation Description.
- Fill in the Date of Hire and the WageWage Period.
- Document the Date of Injury and Time of Injury, and specify if the injury occurred on employer's premises.
- Provide a detailed description of how the injury or illness occurred, including what the employee was doing before the injury.
- If there are dependents involved, list them with their Relationships.
- Complete the Physician Name and Treatment Address if medical treatment is involved.
- Indicate whether the injury required hospitalization and what type of treatment was administered.
- Don’t forget to include the date the form was prepared and the name and title of the preparer.
After filling out the form, make sure to review all entries for accuracy. Once confirmed, submit the completed form to your insurance carrier as required. Keeping a copy for your records is also a good practice.
What You Should Know About This Form
What is the purpose of the Tennessee First Report form?
The Tennessee First Report form is used to report work-related injuries or illnesses. It is necessary for both medical-only claims and indemnity claims as required by Tennessee's Workers' Compensation Law. Employers must complete and submit this form to their insurance carrier immediately after notifying about the injury. Failure to do so can lead to penalties.
Who is required to fill out and submit this form?
Employers in Tennessee are responsible for filling out and submitting the First Report form. This includes both regular and temporary employers in all industries. If an employee suffers a work-related injury or illness, the employer must provide this report to their insurance carrier without delay.
What information is required on the form?
The form requires detailed information, including the employer's and insurance carrier's details, the employee's personal information, nature and cause of the injury, and medical treatment provided. Key areas include the employee's name, date of injury, wage details, and specifics about the nature of the injury and treatment received.
What happens if a false report is submitted?
Submitting a false, incomplete, or misleading report is a crime. Penalties for this action can include imprisonment, fines, and denial of insurance benefits. Employers must ensure the information provided is accurate to avoid facing serious consequences.
How can employers get assistance with the First Report form?
If employers have questions about the First Report form or the workers' compensation process, they can contact the Benefit Review System. Assistance is available through a workers' compensation specialist by calling 1-800-332-2667 (TDD). This resource can help clarify any uncertainties regarding the completion and submission of the form.
Common mistakes
Completing the Tennessee First Report form can seem straightforward, but many individuals stumble along the way. One common mistake is providing incomplete or inaccurate information about the employer. Key details like the employer’s name, address, and Federal Employer Identification Number (FEIN) must be correct. A simple typo or missing data can lead to delays in processing the claim.
Another frequent error lies in how the injury details are described. When filling out the form, it is crucial to detail how the injury occurred clearly. Vague descriptions can leave room for interpretation, which may complicate the claims process. Ensure you specify what the employee was doing, the exact body parts affected, and where the injury happened. This precision can significantly impact the legitimacy of the claim.
Many also overlook the importance of providing accurate information regarding the employee's status at the time of the injury. It’s essential to indicate whether the employee was full-time, part-time, or seasonal. Misclassifying their employment status can alter eligibility for benefits and result in unnecessary confusion. Always double-check this section to avoid any costly misunderstandings.
Filing dates can also be a source of confusion. The form requires specific dates, including the date of injury and the date the employer was notified. Failing to list these correctly or providing conflicting dates could raise red flags during the investigation of the claim. It's advisable to keep a precise record of these events to ensure accuracy.
Finally, individuals sometimes neglect the section concerning wage details. Inaccurate wage information, such as wage amounts or periods, can lead to complications in processing the claim. For instance, not indicating whether the employee was paid full wages for the date of injury can jeopardize benefits. It's wise to verify that these figures reflect the employee’s actual wages.
Documents used along the form
When filing a claim for a work-related injury or illness in Tennessee, several key documents are often required alongside the Tennessee First Report form. These documents provide essential information to ensure the claim is handled accurately and efficiently. Here’s a list of forms commonly used in conjunction with the First Report:
- Employer's Injury Report: A detailed account of the injury that includes specifics about what happened and any immediate actions taken by the employer.
- Employee Claim Form: This form is filled out by the injured employee to provide their personal details and additional information regarding the injury.
- Authorization for Release of Medical Records: This document allows medical professionals to share the employee's treatment records with the employer or insurance carrier.
- Medical Treatment Report: Prepared by healthcare providers, this report outlines the nature of the injury, diagnoses, and treatment plans.
- Workers' Compensation Claim Form: This formal document is submitted to the state’s workers' compensation board to initiate the process of receiving benefits.
- Return to Work Form: After receiving treatment, this document certifies the employee's fitness to return to their job or details any work restrictions.
- OSHA Incident Report: If applicable, this report details workplace incidents that may require OSHA notification and addresses safety concerns.
- Dependent Information Form: In case of a fatality, this form collects necessary information about dependents who may be eligible for benefits.
Submitting these documents, alongside the Tennessee First Report form, helps ensure that all necessary information is available for a smooth claims process. It is crucial to maintain accuracy and completeness to avoid delays or potential issues with claims approval.
Similar forms
- Workers' Compensation Claim Form: Similar to the Tennessee First Report form, this document is used by employers to report work-related injuries or illnesses to the insurance carrier. Both forms require details such as employee information, nature of injury, and claims handling information.
- OSHA Incident Report (OSHA Form 301): Like the Tennessee First Report, this form documents work-related injuries and illnesses. It includes specifics about the incident, what the employee was doing at the time, and the injury sustained.
- Employee Injury Report: Employers use this report to document the circumstances of an employee's injury at the workplace. Similar to the Tennessee form, it captures relevant details about the employee and the nature of the incident.
- First Aid Treatment Record: This record documents cases where first aid was administered for work-related injuries. Both forms require information about the incident and the employee but differ in the severity of the injury reported.
- Incident Investigation Report: This report records findings from an investigation into a workplace incident. It includes details of the injured party and actions taken, mirroring the information gathering aspect of the Tennessee First Report.
- Employer's Report of Injury Form: Used in various states, this form helps document and report work-related injuries. Its purpose aligns closely with that of the Tennessee First Report, focusing on the facts surrounding the incident.
- Health and Safety Incident Report: Similar in purpose, this report details health and safety incidents at work. It requires similar information about the employee and the nature of the incident, serving as a record for compliance and safety evaluations.
- State-Specific Workers' Compensation Forms: Various states have tailored forms for reporting work-related incidents. These share similarities with the Tennessee First Report, focusing on injury details and claims management, though the specific requirements may differ slightly by jurisdiction.
Dos and Don'ts
When filling out the Tennessee First Report form, it is important to follow certain guidelines to ensure the report is completed accurately. Here are nine things to keep in mind:
- Provide complete and accurate information. Every field should be filled in as completely as possible.
- Submit the form promptly. It should be filed immediately after the notice of injury to avoid delays in processing.
- Use clear and concise language. When describing the incident, avoid jargon and be specific about how the injury occurred.
- Verify the names and details. Ensure that all names, dates, and addresses are correct before submission.
- Include all relevant medical information. If there are subsequent medical treatments, these details should be documented.
- Do not leave any mandatory fields blank. Every required section must be filled to prevent rejection of the form.
- Refrain from providing false information. Falsification can lead to serious legal consequences and denial of claims.
- Do not rush the completion of the form. Take the necessary time to ensure accuracy, especially when recounting the incident.
- Avoid using technical jargon or abbreviations. This ensures that all parties can understand the information provided.
These guidelines will help improve the accuracy and effectiveness of your submission. Take care to follow them closely for a smoother claims process.
Misconceptions
-
Misconception 1: The First Report form is optional for employers.
Many believe that submitting the Tennessee First Report form is a voluntary action. In reality, it is mandated by the Tennessee Workers' Compensation Law for any work-related injuries or illnesses. Timely submission is crucial.
-
Misconception 2: Only serious injuries require the form to be filed.
Some individuals think that they only need to file the report for severe injuries. However, all injuries, regardless of severity, must be reported if they are work-related. This includes minor injuries that may lead to complications later.
-
Misconception 3: The form is only for immediate medical treatment cases.
People often assume that the Tennessee First Report is only necessary for cases requiring immediate medical intervention. This is incorrect; it should be submitted for all incidents, even those that may require future medical care.
-
Misconception 4: Completion of the form guarantees claim approval.
Some may think that merely submitting the First Report form ensures that their claim will be approved. While it is a necessary step, approval will depend on various other factors, including the nature of the injury and compliance with state laws.
-
Misconception 5: Any format can be used for submission.
There is a belief that as long as the necessary information is provided, the format does not matter. However, the specific First Report form must be utilized as prescribed by the Tennessee Department of Labor and Workforce Development to ensure compliance.
-
Misconception 6: Only the employer is responsible for filing the report.
Some individuals think that only the employer carries the responsibility for submitting the First Report. In practice, employees also play a role. They must inform their employers of the injury promptly to facilitate the filing.
-
Misconception 7: There are no consequences for not filing the report.
Many might believe that failing to submit the First Report form carries no real consequences. This misunderstanding can be costly, as penalties may include claims denial, fines, and even criminal charges for fraud in cases of false information.
Key takeaways
Filling out the Tennessee First Report form is an essential step for employers and employees following a work-related injury or illness. Understanding this process can aid in efficient claims handling and compliance with state laws. Here are key takeaways to keep in mind:
- Mandatory Use: Employers must use this form to report workplace injuries as required by Tennessee's Workers' Compensation Law.
- Timely Filing: The report must be completed and filed with the insurance carrier immediately after notice of injury to avoid delays in claims processing.
- Honesty is Crucial: Providing false, incomplete, or misleading information can lead to serious penalties, including fines and potential imprisonment.
- Description of Injury: A clear and detailed description of how the injury occurred is crucial. Include what the employee was doing at the time and what body part was affected.
- Injury Location: Clearly state whether the injury occurred on the employer’s premises or elsewhere, as this can affect the claim's validity.
- Correct Codes: Ensure that you use the correct codes for claim types, causes of injury, and nature of injury. This precision helps streamline the claims process.
- Dependent Information: If applicable, provide details about dependents in the case of a fatal accident. This includes their relationships and total number.
- Contact Information: Always include accurate contact details for claim adjusters and preparers to facilitate communication and follow-up.
By following these guidelines, you can ensure that the Tennessee First Report form is filled out correctly, leading to a smoother claims process for everyone involved.
Browse Other Templates
Irs Notice of Levy - Taxpayers receive this notice when previous attempts to collect taxes have failed.
California Attorney General Registry of Charitable Trusts - Organizations must provide accurate contact and identification details in the RRF-1 form.