Fill Out Your Trip Log Mtm Form
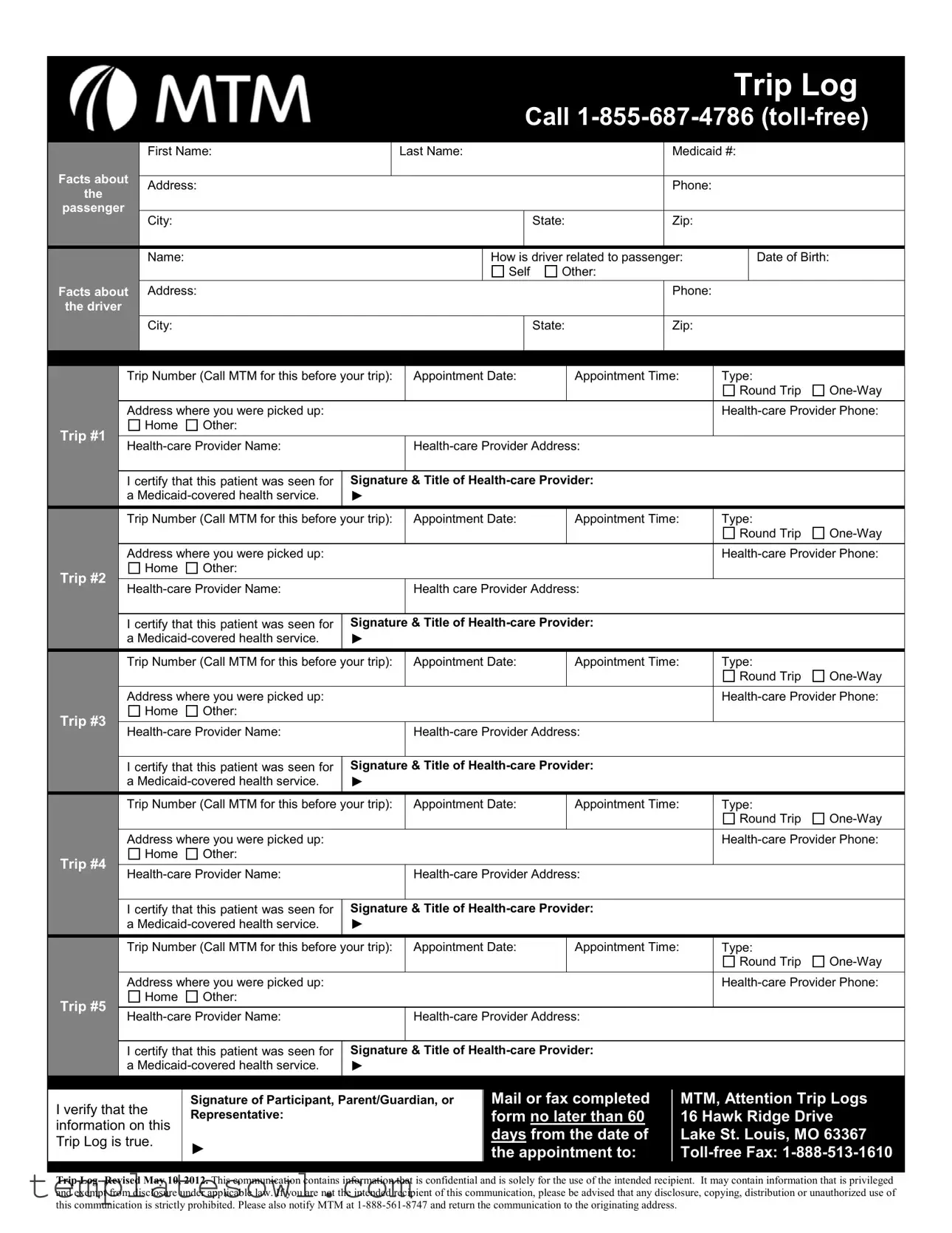
The Trip Log MTM form plays a vital role in ensuring that individuals covered by Medicaid can access necessary transport to their healthcare appointments. This form facilitates the documentation of multiple trips, allowing users to clearly record essential information about each journey. Each section of the form requires details about both the passenger and the driver, including names, Medicaid numbers, and contact information, thereby establishing the connection between the transport service and the passenger receiving services. Additionally, the form prompts users to provide trip specifics such as appointment dates, times, and locations, enabling administrative efficacy in processing transportation needs. Healthcare providers are also required to certify the services rendered, ensuring adherence to Medicaid regulations. Notably, the signed verification by participants or guardians emphasizes the accuracy and truthfulness of the provided information, underscoring the form's significance in safeguarding participants' rights and benefits. As a comprehensive tool, the Trip Log MTM form not only streamlines the transportation request process but also supports Medicaid's mission to facilitate healthcare access for those in need.
Trip Log Mtm Example
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Trip Log |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Call |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
First Name: |
|
|
Last Name: |
|
|
Medicaid #: |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Facts about |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
Address: |
|
|
|
|
|
|
|
|
|
|
Phone: |
|
|
|
||||
|
the |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
passenger |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
City: |
|
|
|
|
|
|
|
|
State: |
|
Zip: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name: |
|
|
|
|
|
|
How is driver related to passenger: |
|
Date of Birth: |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Self |
Other: |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Facts about |
|
Address: |
|
|
|
|
|
|
|
|
|
|
Phone: |
|
|
|
|||
|
the driver |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
City: |
|
|
|
|
|
|
|
|
State: |
|
Zip: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
Trip Number (Call MTM for this before your trip): |
|
Appointment Date: |
|
Appointment Time: |
Type: |
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Round Trip |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
Address where you were picked up: |
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
Home |
Other: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Trip #1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
I certify that this patient was seen for |
Signature & Title of |
|
|
|
||||||||||||
|
|
|
|
a |
► |
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
Trip Number (Call MTM for this before your trip): |
|
Appointment Date: |
|
Appointment Time: |
Type: |
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Round Trip |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
Address where you were picked up: |
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
Home |
Other: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Trip #2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Health care Provider Address: |
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
I certify that this patient was seen for |
Signature & Title of |
|
|
|
||||||||||||
|
|
|
|
a |
► |
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
Trip Number (Call MTM for this before your trip): |
|
Appointment Date: |
|
Appointment Time: |
Type: |
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Round Trip |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
Address where you were picked up: |
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
Home |
Other: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Trip #3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
I certify that this patient was seen for |
Signature & Title of |
|
|
|
||||||||||||
|
|
|
|
a |
► |
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
Trip Number (Call MTM for this before your trip): |
|
Appointment Date: |
|
Appointment Time: |
Type: |
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Round Trip |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
Address where you were picked up: |
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
Home |
Other: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Trip #4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
I certify that this patient was seen for |
Signature & Title of |
|
|
|
||||||||||||
|
|
|
|
a |
► |
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
Trip Number (Call MTM for this before your trip): |
|
Appointment Date: |
|
Appointment Time: |
Type: |
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Round Trip |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
Address where you were picked up: |
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
Home |
Other: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Trip #5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
I certify that this patient was seen for |
Signature & Title of |
|
|
|
||||||||||||
|
|
|
|
a |
► |
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I verify that the |
Signature of Participant, Parent/Guardian, or |
Mail or fax completed |
MTM, Attention Trip Logs |
|
Representative: |
form no later than 60 |
16 Hawk Ridge Drive |
||
information on this |
||||
|
days from the date of |
Lake St. Louis, MO 63367 |
||
Trip Log is true. |
► |
|||
the appointment to: |
||||
|
Trip Log- Revised May 10, 2012. This communication contains information that is confidential and is solely for the use of the intended recipient. It may contain information that is privileged and exempt from disclosure under applicable law. If you are not the intended recipient of this communication, please be advised that any disclosure, copying, distribution or unauthorized use of this communication is strictly prohibited. Please also notify MTM at
|
|
|
Trip Number (Call MTM for this before your trip): |
Appointment Date: |
Appointment Time: |
|
|
|
Type: |
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Round Trip |
||
|
|
|
Address where you were picked up: |
|
|
|
|
|
|
|
|
||||
|
|
|
Home |
Other: |
|
|
|
|
|
|
|
|
|
|
|
|
Trip #6 |
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I certify that this patient was seen for |
Signature & Title of |
|
|
|
|
|
|
|||||
|
|
|
a |
► |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Trip Number (Call MTM for this before your trip): |
Appointment Date: |
Appointment Time: |
|
|
|
Type: |
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Round Trip |
||
|
|
|
Address where you were picked up: |
|
|
|
|
|
|
|
|
||||
|
|
|
Home |
Other: |
|
|
|
|
|
|
|
|
|
|
|
|
Trip #7 |
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
Health care Provider Address: |
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I certify that this patient was seen for |
Signature & Title of |
|
|
|
|
|
|
|||||
|
|
|
a |
► |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Trip Number (Call MTM for this before your trip): |
Appointment Date: |
Appointment Time: |
|
|
|
Type: |
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Round Trip |
||
|
|
|
Address where you were picked up: |
|
|
|
|
|
|
|
|
||||
|
|
|
Home |
Other: |
|
|
|
|
|
|
|
|
|
|
|
|
Trip #8 |
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I certify that this patient was seen for |
Signature & Title of |
|
|
|
|
|
|
|||||
|
|
|
a |
► |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Trip Number (Call MTM for this before your trip): |
Appointment Date: |
Appointment Time: |
|
|
|
Type: |
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Round Trip |
||
|
|
|
Address where you were picked up: |
|
|
|
|
|
|
|
|
||||
|
|
|
Home |
Other: |
|
|
|
|
|
|
|
|
|
|
|
|
Trip #9 |
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I certify that this patient was seen for |
Signature & Title of |
|
|
|
|
|
|
|||||
|
|
|
a |
► |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Trip Number (Call MTM for this before your trip): |
Appointment Date: |
Appointment Time: |
|
|
|
Type: |
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Round Trip |
||
|
|
|
Address where you were picked up: |
|
|
|
|
|
|
|
|
||||
|
|
|
Home |
Other: |
|
|
|
|
|
|
|
|
|
|
|
|
Trip #10 |
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I certify that this patient was seen for |
Signature & Title of |
|
|
|
|
|
|
|||||
|
|
|
a |
► |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Trip Number (Call MTM for this before your trip): |
Appointment Date: |
Appointment Time: |
|
|
|
Type: |
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Round Trip |
||
|
|
|
Address where you were picked up: |
|
|
|
|
|
|
|
|
||||
|
|
|
Home |
Other: |
|
|
|
|
|
|
|
|
|
|
|
|
Trip #11 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I certify that this patient was seen for |
Signature & Title of |
|
|
|
|
|
|
|||||
|
|
|
a |
► |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Trip Number (Call MTM for this before your trip): |
Appointment Date: |
Appointment Time: |
|
|
|
Type: |
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Round Trip |
||
|
|
|
Address where you were picked up: |
|
|
|
|
|
|
|
|
||||
|
|
|
Home |
Other: |
|
|
|
|
|
|
|
|
|
|
|
|
Trip #12 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I certify that this patient was seen for |
Signature & Title of |
|
|
|
|
|
|
|||||
|
|
|
a |
► |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I verify that the |
Signature of Participant, Parent/Guardian, or |
|
Mail or fax completed |
|
MTM, Attention Trip Logs |
|
||||||||
|
Representative: |
|
|
|
form no later than 60 |
|
16 Hawk Ridge Drive |
|
|||||||
|
information on this |
|
|
|
|
|
|||||||||
|
|
|
|
|
days from the date of |
|
Lake St. Louis, MO 63367 |
|
|||||||
|
Trip Log is true. |
► |
|
|
|
|
|
||||||||
|
|
|
|
the appointment to: |
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Trip Log- Revised May 10, 2012. This communication contains information that is confidential and is solely for the use of the intended recipient. It may contain information that is privileged and exempt from disclosure under applicable law. If you are not the intended recipient of this communication, please be advised that any disclosure, copying, distribution or unauthorized use of this communication is strictly prohibited. Please also notify MTM at
Form Characteristics
| Fact Name | Fact Description |
|---|---|
| Purpose | The Trip Log MTM form is used to document non-emergency medical transportation for Medicaid patients. |
| Required Information | The form requires personal information from both the passenger and the driver, including names, addresses, Medicaid numbers, and relationships. |
| Appointment Details | Passengers must provide specific details regarding their appointment, including the date, time, and type of trip (round trip or one-way). |
| Health-care Provider Verification | Health-care providers must certify that the patient received Medicaid-covered services, requiring their signature and title. |
| Submission Requirements | The completed form should be sent to MTM no later than 60 days after the appointment. This ensures timely processing of transportation requests. |
| Confidentiality Notice | The form includes a statement regarding the confidentiality and privileged information contained within, addressing unauthorized use or disclosure. |
Guidelines on Utilizing Trip Log Mtm
Completing the Trip Log Mtm form requires careful attention to detail to ensure all necessary information is accurately provided. Follow these steps closely to fill out the form correctly. Be prepared with the required information regarding the passenger, driver, and trip details as you proceed.
- Start by providing the First Name and Last Name of the passenger.
- Enter the Medicaid # associated with the passenger.
- Fill in the Address, Phone number, City, State, and Zip code for the passenger.
- Next, record the Name of the driver and indicate how the driver is related to the passenger.
- Provide the Date of Birth for the driver.
- Again, fill out the Address, Phone, City, State, and Zip code for the driver.
- Contact MTM to obtain the Trip Number before moving on.
- Input the Appointment Date and Appointment Time.
- Select the Type of trip: either Round Trip or One-Way.
- State the Address where you were picked up for the trip.
- Provide the Health-care Provider Phone number.
- Document the Health-care Provider Name and the Health-care Provider Address.
- In the designated space, include the Signature & Title of Health-care Provider to certify that the patient received a Medicaid-covered health service.
- If multiple trips are listed, repeat steps 7 through 15 for each trip, making sure to enter the correct Trip Number for each.
- Finally, ensure that the Signature of the participant, parent/guardian, or authorized individual is added. Mail or fax the completed form to MTM, Attention Trip Logs Representative, at the provided address.
- Remember to submit the form within 60 days from the date of the appointment to ensure timely processing.
Once the form is filled out, double-check all entries for accuracy and completeness. Submitting the completed form as instructed will help facilitate a smooth process for trip reimbursement or service validation. Maintain a copy for your records before sending it to MTM.
What You Should Know About This Form
What is the Trip Log MTM form used for?
The Trip Log MTM form serves as a documentation tool for tracking non-emergency medical transportation for Medicaid recipients. It captures essential details, including trip information, healthcare appointments, and verification of services provided. This helps ensure that individuals receive necessary transportation for their medical needs.
How do I complete the Trip Log MTM form?
To complete the form, provide personal details of the passenger and driver. This includes names, Medicaid numbers, contact information, and addresses. It is important to accurately fill in the appointment details, such as the date, time, and type of trip. Be sure to have the trip number, which can be obtained by calling MTM before your travel.
What are the requirements for submitting the Trip Log MTM form?
The completed form must be signed by the healthcare provider who confirms the Medicaid-covered service was provided. It is essential to submit the form within 60 days from the date of the appointment, ensuring that all information is accurate to avoid delays in processing.
Can I submit the form via email?
Email submission is not allowed. Instead, you can mail or fax the completed Trip Log MTM form to MTM's designated address or fax number, which is located on the form itself. This ensures that your privacy and confidentiality are maintained during the submission process.
What should I do if I need assistance while filling out the form?
If you require help with the form, you can reach out to MTM by calling the toll-free number provided, 1-855-687-4786. They can provide guidance on how to fill out the form correctly and answer any specific questions you may have.
What happens if I lose my Trip Log MTM form?
In case the form is lost, it is advisable to fill out a new one. Make sure to gather all necessary information again and submit the new form within the designated timeframe. Keeping a copy of the completed document for your records may also be beneficial.
What if my trip information changes after submission?
For changes in trip details after submission, it is essential to communicate directly with MTM. They can provide instructions on how to update your information and ensure that your transportation remains uninterrupted.
Is there a deadline for sending in the completed Trip Log MTM form?
The completed form must be submitted no later than 60 days from the date of the healthcare appointment. Adhering to this timeline is crucial to ensure that Medicaid benefits for transportation services are not adversely affected.
Common mistakes
When filling out the Trip Log MTM form, it is crucial to avoid common errors that can delay your processing. One typical mistake is failing to provide accurate trip numbers. Each trip requires a unique number that you can obtain by calling MTM before your appointment. If this step is overlooked, it could lead to your trip not being verified, which may affect your transportation arrangements.
Another frequent error is not including complete contact information for both the passenger and the driver. It's essential to fill out their first name, last name, phone number, and address thoroughly. Additionally, omitting details like the city or state can result in further delays in processing your request.
Many individuals also misinterpret the appointment date and time. Make sure the appointment details are current and correctly filled out on the form. If these details are inaccurate, it can lead to scheduling conflicts or, worse, a missed appointment entirely. Always double-check this information to ensure it aligns with your healthcare provider’s schedule.
Finally, signing the form is a step that some forget to complete. The signature and title of the health-care provider is mandatory for the form to be valid. Without it, the form lacks the necessary legitimacy to proceed. Ensure that all required signatures are present before submitting the form to avoid unnecessary complications.
Documents used along the form
The Trip Log MTM form is a crucial document for Medicaid transportation services, detailing essential trip information. To ensure proper processing and verification of these trips, a few additional forms and documents are typically used. Each plays a significant role in creating a complete record of transportation for Medicaid-covered health services.
- Medicaid Transportation Request Form: This form is used to formally request transportation services for a Medicaid-covered appointment. It outlines the patient's needs and specifies the type of service required.
- Provider Certification Form: A healthcare provider must complete this form to certify that the patient received a Medicaid-covered service. It's essential for ensuring that payment is authorized for the transportation services provided.
- Patient Information Release Form: This document allows for the sharing of a patient's health information necessary for processing transportation requests. It ensures compliance with privacy regulations while allowing the necessary providers to access information about the patient's healthcare needs.
- Appointment Verification Form: This form confirms the details of the patient's appointment with their healthcare provider. It includes the date, time, and location, which helps to avoid scheduling conflicts and ensures timely transportation.
These documents, when used alongside the Trip Log MTM form, streamline the process for patients utilizing Medicaid transportation services. Accurate completion of each form is vital for a seamless experience in securing transportation for healthcare appointments.
Similar forms
The following documents share similarities with the Trip Log MTM form. Each has its own function but involves capturing details about medical transportation, appointments, or service verification.
- Patient Transportation Request Form: Like the Trip Log MTM, this form requests information to arrange transportation for medical appointments, focusing on patient data, appointment times, and locations.
- Medicaid Transportation Reimbursement Form: This document is used to seek reimbursement for authorized medical transportation. It collected similar data such as trip details and provider information.
- Medical Appointment Verification Form: This form serves to confirm attendance at medical appointments. It requires similar identifying information of the patient and health care provider.
- Medicaid Provider Claim Form: It is used by health care providers to claim fees for services rendered. This document captures patient details and appointment specifics, paralleling the information on the Trip Log MTM.
- Service Coordination Log: This log tracks coordination of services for patients. It shares the need for detailed information about appointments and involved service providers.
- Patient Information and Consent Form: This form collects necessary information about patients, including demographics and appointment details, similar to what is gathered in the Trip Log MTM.
- Health Care Service Authorization Form: Used to authorize transport for medical services, this document often includes patient and provider information, resembling the Trip Log MTM.
- Transport Delivery Confirmation Form: This form confirms that transportation was provided for a medical service, requiring details on the journey and provider, much like the Trip Log MTM.
Dos and Don'ts
When filling out the Trip Log MTM form, it’s essential to be careful and accurate. Here are some guidelines to help you avoid common mistakes:
- Do ensure that all required fields are completed. This includes names, addresses, and Medicaid numbers.
- Do verify the Trip Number with MTM before filling out subsequent sections. An incorrect trip number can lead to complications.
- Do check the appointment date and time carefully. Entering the wrong information can delay processing.
- Do get the signature of the healthcare provider. This certification is vital for validation.
- Do submit the form within 60 days of the appointment. Delays may affect payment for your trip.
- Don’t leave any sections blank. Incomplete submissions can result in rejections or requests for additional information.
- Don’t forget to contact MTM for clarification on any part of the form if you are unsure how to fill it out.
- Don’t ignore the confidentiality of the information provided. This data is sensitive; handle it with care.
- Don’t wait until the last minute to complete the form. Procrastination can lead to errors and missed deadlines.
- Don’t affix a stamp on the form if faxing it. Ensure you are using the correct method of submission.
Misconceptions
The Trip Log MTM form is essential for documenting transportation for Medicaid-covered services. However, several misconceptions can lead to confusion. Below are nine common misunderstandings about this form, along with clarifications to help you navigate its requirements.
- It's only for certain types of trips. Many believe the form only applies to specific Medicaid services. In reality, it covers all medically necessary transportation for Medicaid members.
- The form does not require a signature. Some think that a signature is unnecessary. However, a healthcare provider's signature is crucial to certify that services were rendered.
- You can submit the form anytime. There is a common misconception that timing is flexible. The form must be submitted within 60 days from the appointment date for reimbursement.
- Only the driver needs to be listed. Some individuals fail to include passenger information. Both the driver and passenger details are required for proper record-keeping.
- Round trips are not documented. It is a misconception that only one-way trips need to be noted. The form includes sections for both round trips and one-way trips, ensuring comprehensive documentation.
- Health provider information is optional. Many people think that including health provider details is not mandatory. In fact, this information is critical and must be accurately provided.
- You cannot amend the form once submitted. Some assume revisions are impossible after submission. Corrections can be made, but they must follow specific guidelines set by MTM.
- Only Medicaid members can fill out the form. A common error is believing only the member can complete it. Caregivers or guardians are also permitted to fill it out on the member’s behalf.
- There are no penalties for inaccuracies. Some people think it’s fine to make mistakes on the form. However, incorrect information can lead to delays in processing requests or even denials of reimbursement.
Understanding these misconceptions can help ensure a smoother experience when using the Trip Log MTM form. Accurate completion of the form spells a better outcome for those needing transportation services.
Key takeaways
Understanding the Trip Log Mtm form is crucial for ensuring proper documentation of Medicaid transportation services. Here are the key takeaways:
- The form requires basic personal information about both the passenger and the driver.
- It's essential to confirm the trip number before scheduling the appointment; call MTM for this.
- Provide accurate details about the appointment, including date, time, and type of trip (one-way or round trip).
- Document the address where the passenger was picked up clearly to avoid any confusion.
- Each trip requires certification from a healthcare provider confirming that a Medicaid-covered health service was rendered.
- Submit the completed form within 60 days from the appointment date to ensure valid processing.
- Use the specified contact information for submitting the form, including the fax number and MTM's attention line.
- Keep a copy of the submitted form for your records to verify compliance and track any issues that may arise.
By adhering to these points, you ensure a smoother experience with the Trip Log Mtm process.
Browse Other Templates
What Does a Court Summons Look Like - Legal representatives must be properly notified of the lawsuit as well.
Types of Health Savings Accounts - This form is a tool to help you access your qualified health expense reimbursements easily.
Florida Estate Tax Exemption 2023 - Be sure to detail the mailing address of the personal representative on the Fl Dr 312 form.