Fill Out Your Uft Welfare Fund Contact Form
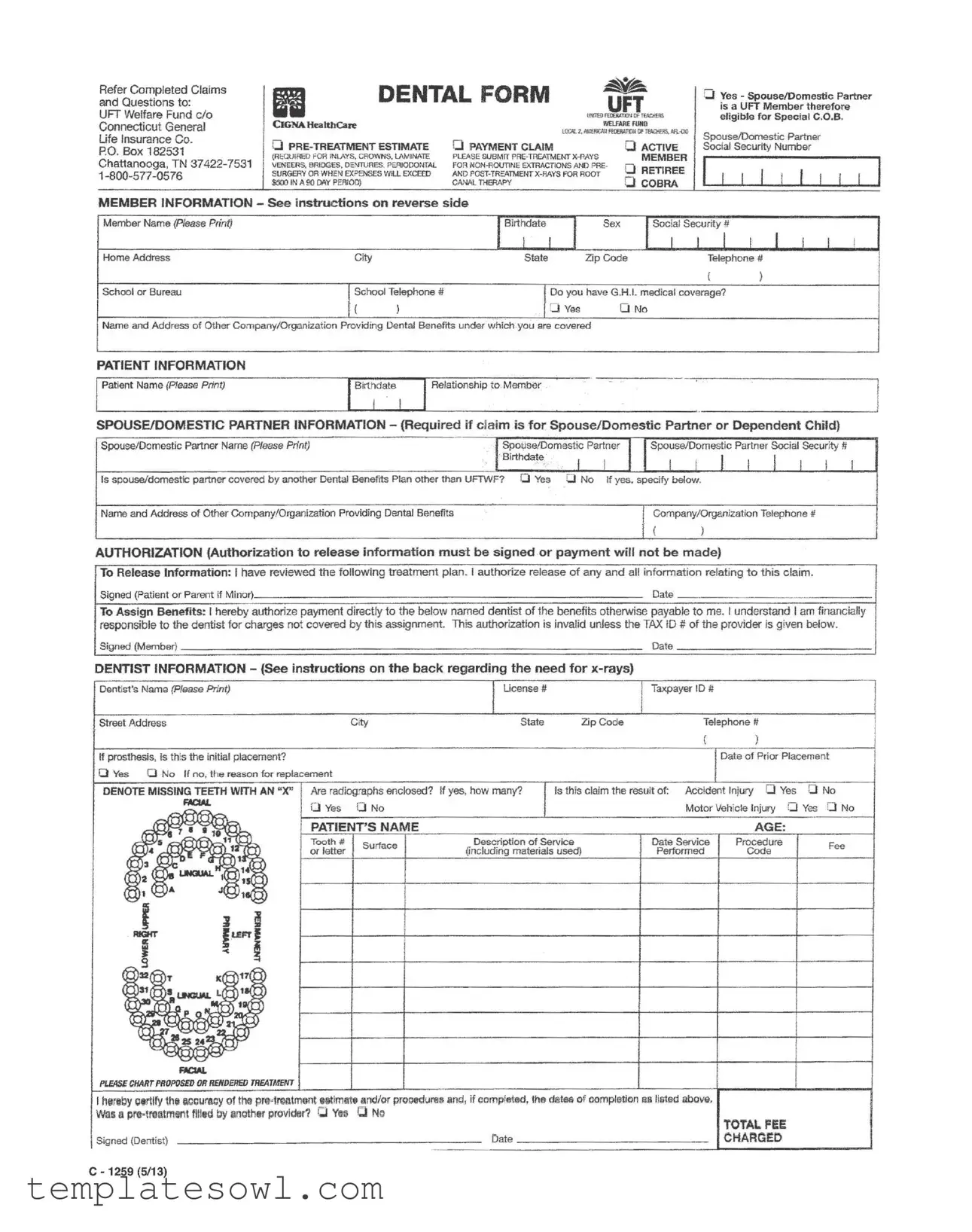
When navigating the UFT Welfare Fund Contact form, it’s important to understand the essential components that help facilitate dental claims for members and their families. This form is designed for various dental procedures, ensuring that members can submit claims for treatments like crowns, veneers, dentures, and more. Whether you're a current member or a retiree, details about your coverage, alongside the specific treatment you received, must be included. Members must provide personal information such as their name, address, and school affiliation, as well as the details of any dependents involved in the claim. Authorization for releasing information is critical; without the necessary signatures, claims cannot be processed. To ensure the claim is properly managed, it is also required to list the dentist's information, including their tax identification number. Members are encouraged to attach relevant radiographs when necessary to support their claims. With this form, patients can keep track of their dental expenses while accessing the benefits afforded to them by the UFT Welfare Fund.
Uft Welfare Fund Contact Example
Refer Completed Claims and Questions to:
UFT Welfare Fund c/o Connecticut General Life Insurance Co.
PO. Box 182531
Chattanooga, TN
II |
DENTAL FORM |
セ |
||
|
UFT |
|||
|
|
|
||
|
umro FEOERATD!I Of TEACtiERS |
|||
|
|
WElFARE RRtD |
||
CIGNA HcaltbCare |
|
lQO,l. Z. N.:EfICAIl FroEMTDH Of セ AA.:O<l |
||
|
|
|||
Q |
o PAYMENT CLAIM |
|
o ACTIVE |
|
(REQUIRED FOR INlAYS, CROWNS. LAMINATE |
PLEASE SUBMIT |
|
MEMBER |
|
VENEERS, BRIDGES, DENTURES. PERIODONTAL FOR |
o RETIREE |
|||
SURGERY OR WHEN EXPENSES WIlL EXCEED |
AND POST·TREATMENT |
|
||
$500 IN A 90 DAY PERIOD) |
|
CANAl. THERAPY |
|
o COBRA |
|
|
|
|
|
QYes - Spouse/Domestic Partner is a UFT Member therefore eligible for Special C.O.B.
SpouselDomestic Partner
Social Security Number
ILLJ
MEMBER INFORMATION - See instructions on reverse side |
Ibゥイエセ、。エ・I |
|
|
Isoc;al ウ・セイゥエケi |
|
|
|
|
|||
Member Name (Please Print) |
|
|
I |
Sex |
I |
I |
I I |
I |
|||
Home Address |
City |
|
State |
|
Zip Code |
|
Telephone # |
|
|
|
|
|
|
|
|
|
|
|
( |
) |
|
|
|
School or Bureau |
ISchool Telephone # |
IDo you have G.H.L medical coverage? |
|
|
|
|
|||||
|
|
|
|
|
|||||||
|
{ |
) |
DYes |
0 |
No |
|
|
|
|
|
|
Name and Address of Other Company/Organization Providing Dental Benefits under which you are covered |
|
|
|
|
|
|
|||||
PATIENT INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
Patient Name (Please Print) |
|
Relationship to Member |
|
|
|
|
|
|
|
|
|
SPOUSE/DOMESTIC PARTNER INFORMATION - (Required if claim is for Spouse/Domestic Partner or Dependent Child) |
|
||||||||||
Spouse/Domestic Partner Name (please Print) |
|
|
I.sセッエゥウ・Odッュ・ウエゥ」 |
Partner |
I ISpouselDomestic Partner Social Security II |
|
|||||
|
|
. |
. Xiイエィ、。Aセ |
.' I |
I |
I I |
I |
I |
I |
I I |
I |
Is spouse/domestic partner covered by another Dental Benefits Plan other than UFTWF? o Yes |
o No If yes. specify below. |
|
|
|
|
|
|||||
Name and Address of Other Company/Organization Providing Dental Benefits |
|
|
|
ICompany/Organization Telephone # |
|
||||||
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
( |
) |
|
|
|
|
AUTHORIZATION (Authorization to release information must be signed or payment will not be made)
To Release Information: I have reviewed the following treatment plan. I authorize release of any and all information relating to this claim.
Signed (Patient or Parent if Minor) |
Date |
To Assign Benefits: I hereby authorize payment directly to the below named dentist of the benefits otherwise payable to me. I understand I am financially responsible to the dentist for charges not covered by this assignment. This authorization is invalid unless the TAX 10 # of the provider is given below.
Signed (Member)Date
DENTIST INFORMATION - (See instructions on the back regarding the need for
Dentist's Name (please Print) |
|
|
IUcense# |
|
Taxpayer 10 II |
|
|
|
|
|
|
|
|
|
|
|
|
Street Address |
|
City |
State |
Zip Code |
Telephone II |
|
|
|
|
|
|
|
|
( |
) |
|
|
If prosthesis, is this the initial placement? |
|
|
|
|
|
Date of Prior Placement |
||
o Yes 0 No If no. the reason for replacement |
|
|
|
|
|
|
|
|
DENOTE MISSING TEETH WITH AN "X" |
Are radiographs enclosed? If yes, how many? 115 this claim the result of: Accident Injury 0 Yes |
0 No |
||||||
セ |
DVes ONo |
|
|
Motor Vehicle Injury |
0 |
Yes 0 No |
||
|
l |
|||||||
|
PATIENT'S NAME |
|
|
|
AGE: |
|
|
|
|
Tooth # |
Surtace |
Description of Service |
|
Date Service |
Procedure |
|
Fee |
|
or letter |
(including materials used) |
Performed |
Code |
|
|||
|
|
|
|
|||||
(
(
(
I herllby certify thllllcourAcy of tho prll'lrllAtmont Illitimlltlll!lnd/or ーイッcHャ、セイャャャャャゥャョ、L if eomplotod, the dliltelil of oompletion !lllillitli!d llbov!i, Was II pl'8>tl'llfttment filled by llnother provldllr7 Q Ya C No
|
|
TOTAL FEE |
Signed {Dentist) |
Oate |
CHARGED |
C - 1259 (5/13)
Form Characteristics
| Fact Name | Description |
|---|---|
| Contact Information | Completed claims and inquiries should be directed to the UFT Welfare Fund at Connecticut General Life Insurance Co., PO Box 182531, Chattanooga, TN 37422-7531. A dedicated phone line, 1-800-577-0576, is available for assistance. |
| Type of Claims | This form can be used for various dental procedures, including routine check-ups and specific treatments like crowns, bridges, and dentures. Additional requirements may apply based on the nature of the service. |
| Authorization Requirement | Patients must sign an authorization to release information for their claims to be processed. This is necessary to ensure compliance with health information regulations. |
| Coverage Options | The form allows users to specify if their spouse or domestic partner is a UFT member, which can impact eligibility for dental benefits, including COBRA options. |
| Dental Provider Details | Providers are required to fill in their license number and taxpayer ID on the form. This information is crucial for direct benefit assignments and ensures accurate billing. |
| State-Specific Regulations | In Connecticut, the form is governed by state insurance laws that oversee patient rights and insurance claims processing, ensuring fair treatment of all claims. |
Guidelines on Utilizing Uft Welfare Fund Contact
Once the UFT Welfare Fund Contact form is completed, the next step is to submit it to the appropriate address mentioned in the instructions. Be sure to include all necessary documents related to your claim. This ensures that your request is processed efficiently and accurately.
- Gather all relevant information and documents before starting to fill out the form.
- Clearly print your Member Name, Home Address, and Contact Information in the designated fields.
- Complete the section for Social Security Number and School or Bureau details.
- Indicate whether you have G.H.L medical coverage by checking 'Yes' or 'No'.
- Enter the Name and Address of any other company providing dental benefits.
- Fill out the patient information, including Patient Name and Relationship to the member.
- If claiming for a spouse or domestic partner, provide their Name and relevant details.
- Check if the spouse or partner is covered by another dental benefits plan.
- Sign the authorization sections for releasing and assigning benefits.
- Enter the Dentist's Information, including the dentist's Name, License Number, and address.
- Indicate if the claim is due to an accident or injury.
- Complete the section detailing the services provided, including Description of Service and Procedure Fee.
- Finally, ensure all signatures are in place, and check that all sections are filled out completely.
What You Should Know About This Form
What is the UFT Welfare Fund Contact form used for?
The UFT Welfare Fund Contact form is utilized to submit claims related to dental procedures, request pre-treatment estimates, and address questions regarding dental benefits. Proper completion of the form ensures timely processing of claims and inquiries.
Where do I send the completed UFT Welfare Fund Contact form?
You should send the completed form to the following address: UFT Welfare Fund c/o Connecticut General Life Insurance Co., PO Box 182531, Chattanooga, TN 37422-7531. It is important to mail your documents to this address to ensure they are received by the appropriate department.
What information do I need to provide on the form?
The form requires personal details such as your name, address, phone number, and the name of your school or bureau. Additionally, you must provide information regarding the patient’s relationship to you, details of dental services rendered, and any prior benefits or insurance coverage.
Is there a specific format for submitting x-rays for dental claims?
Yes, if your claim involves certain procedures such as implants or crowns, you will need to include x-rays. Ensure that these x-rays are enclosed with your claim to avoid delays in processing.
Can I assign benefits directly to my dentist?
Yes, you can assign benefits directly to your dentist by signing the authorization section on the form. It's important to provide the dentist's Tax ID number, as this will validate the assignment of benefits.
What if my spouse or domestic partner is also a UFT member?
If your spouse or domestic partner is a UFT member, they may be eligible for special COBRA benefits. Make sure to check the appropriate box on the form and provide their Social Security number for verification.
What do I do if my claim is for a minor?
If the claim is for a dependent child, a parent or guardian must sign the authorization section on their behalf. This ensures that information is properly handled and that payment can be processed for the minor's dental services.
How will I know if my claim has been received?
You may contact the UFT Welfare Fund at 1-800-577-0576 for confirmation once you have sent your claim. Keeping a copy of your submitted form may also help you track your request.
What happens if my claim is denied?
If your claim is denied, the UFT Welfare Fund will provide you with a written explanation. You can appeal the decision if you believe the denial was incorrect. Detailed instructions will typically accompany the denial notice.
What should I do if I have further questions about the form?
If you have additional questions regarding the UFT Welfare Fund Contact form or your claims, it is advisable to contact their office directly. They can provide clear guidance and support to address your specific concerns.
Common mistakes
Filling out the UFT Welfare Fund Contact form can be a straightforward process, but there are several common mistakes that people often make. Addressing these errors can help ensure that claims are processed efficiently.
One frequent mistake is not providing complete contact information. It's essential to fill in the member’s home address, telephone number, and school or bureau details accurately. Missing or incorrect information can lead to delays in communication and the processing of claims.
Another common error is neglecting to sign the authorization section. A signature is crucial for releasing information related to the claim. Without it, the claim may be denied, causing unnecessary frustration for everyone involved.
Many individuals also forget to include the tax identification number (TIN) of the dentist. This detail is mandatory for the authorization to be valid. Omitting it can result in payment delays, as insurance companies require this information for processing.
Some people incorrectly assume that all dental claims are routine. When filling out the form, it's important to indicate if the claim is for non-routine procedures. Such details can impact the approval process and help ensure that appropriate coverage is applied.
Another mistake involves the patient relationship information. In instances where the claim is submitted for a spouse or dependent child, the member must provide correct relationship details. Failing to do so can lead to misclassification of the claim, which complicates processing.
The description of service is another area where mistakes often occur. Clear and accurate descriptions, including procedure codes, are essential. Vague or incomplete descriptions can prevent timely approvals and payments.
People also frequently overlook completing the section regarding other dental benefits. Informing the UFT Welfare Fund about any other dental plans is necessary. This helps determine primary and secondary coverage, which is key for processing claims correctly.
Lastly, many claimants forget to include or indicate x-ray submissions when required. If the treatment involves complex procedures like crowns or bridges, x-rays might be necessary. Not providing these can slow down the claims process or lead to denial altogether.
Documents used along the form
When dealing with the UFT Welfare Fund Contact form, several additional documents may be required to ensure a comprehensive response to claims and inquiries. These documents work in conjunction with the contact form to provide necessary information regarding healthcare benefits.
- Dental Claim Form: This form captures detailed information about dental procedures received, including costs associated with treatment, and is essential for filing reimbursement claims.
- Pre-Treatment Estimate Form: Prior to receiving dental work, this form serves to estimate the costs involved. It allows members to understand their financial responsibility before services are rendered.
- Authorization Form: This document grants permission for the release of personal medical information pertinent to the claim. It is crucial that members sign this to avoid delays in payment.
- COBRA Notification Form: For those eligible for continued health insurance coverage under COBRA, this form details rights and responsibilities, ensuring that members are aware of their options following employment changes.
- Dependent Information Form: This form collects necessary details about dependents for whom healthcare benefits are being claimed. It ensures that all eligible family members receive coverage.
- Claim Appeal Form: If a claim is denied, this form is used to formally request a review. It is essential for members who wish to contest the decision and seek appropriate benefits.
Members should ensure that all required documents are accurately completed and submitted in a timely manner to facilitate smooth processing of their claims and inquiries. Prompt action can significantly affect the outcome of benefit requests.
Similar forms
-
Health Insurance Claim Form: This document is used by patients to request payment from their health insurance provider. Just like the UFT Welfare Fund Contact form, it requires detailed information about the member, the medical services received, and typically includes an authorization section for the release of pertinent information.
-
Dental Treatment Plan Authorization: This form is presented to members before dental procedures and secures consent for treatment. Similar to the UFT form, it requires a member’s signature to authorize information sharing regarding treatment plans, which might be necessary for coverage determination.
-
COBRA Election Notice: This document assists individuals in maintaining health coverage after leaving employment. Like the UFT Welfare Fund Contact form, it contains sections to collect relevant member information and guide them through the specifics of their healthcare options.
-
Medicare Enrollment Application: This application is crucial for qualifying seniors to enroll in Medicare. It shares similarities with the UFT form in that it collects personal and eligibility information, ensuring that the application process is seamless and serves the members' healthcare needs directly.
-
Authorization for Release of Health Information Form: Patients use this form to allow healthcare providers to share their medical information. Like the UFT form, it emphasizes the necessity for patient consent before any information related to their healthcare is disclosed to third parties.
-
Claim of Insurance Benefits Form: This is utilized for various insurance benefits, ensuring that members can claim reimbursements for expenses incurred. The structure parallels that of the UFT form, which also serves a similar purpose for dental claims.
-
Dependent Care Claim Form: This document allows members to request reimbursement for childcare expenses under a flexible spending account. Its purpose aligns with the UFT form as it necessitates completing member and dependent information to successfully process the claim.
-
Vision Insurance Claim Form: This document is specific to claims related to eye care. Like the UFT Welfare Fund Contact form, it includes sections requesting patient information, treatment details, and payment authorizations to facilitate a smooth claims process.
-
Flexible Spending Account Claim Form: This form is used for reimbursing qualified medical expenses. Similar in nature to the UFT form, it requires detailed expense information, member identification, and proof of payment to process claims accurately.
-
Personal Injury Protection (PIP) Claim Form: This is necessary after an automobile accident for members seeking coverage for medical expenses. Like the UFT form, it includes sections for comprehensive details on the claim, including authorization to access relevant information regarding the incident.
Dos and Don'ts
When filling out the UFT Welfare Fund Contact form, consider the following:
- Read the entire form carefully before beginning.
- Use clear and legible handwriting or fill out the form online if possible.
- Provide accurate contact information, including your phone number.
- Enter all required fields to avoid delays in processing your claim.
- Double-check that you have signed the form where required.
Avoid these common mistakes:
- Do not leave any required fields blank.
- Don’t forget to submit any required supporting documents.
- Avoid using abbreviations or shorthand that may confuse the reader.
- Don’t send the form to the wrong address. Verify the mailing details.
- Refrain from providing incorrect or outdated insurance information.
Misconceptions
When it comes to the UFT Welfare Fund Contact Form, there are several misconceptions that can lead to confusion. Let’s clear the air on some common myths.
- Myth 1: Only active UFT members can use the contact form.
- Myth 2: Claims must be submitted in person for processing.
- Myth 3: The form is only for dental claims.
- Myth 4: You cannot submit a claim without prior authorization.
- Myth 5: You need to provide photocopies of your dental records.
- Myth 6: Claims take months to process.
This is not true. Both active members and retirees can submit claims and questions using the form. The support is available for everyone covered under the UFT Welfare Fund.
This is a misunderstanding. Claims can be mailed to the UFT Welfare Fund’s designated address. In fact, many members choose to submit their forms by post for convenience.
While the form prominently features dental claims, it can be used for other types of inquiries related to the welfare fund. Always check the specific instructions provided with the form.
In many cases, you can submit a claim after receiving treatment. However, certain procedures do require a pre-treatment estimate to ensure coverage. It’s good to be aware of these requirements.
This is misleading. You are often only required to submit x-rays if specifically requested. Always read the instructions thoroughly to understand what documentation is necessary.
While processing times can vary, many claims are handled efficiently. Following all instructions and submitting complete information can speed up the process significantly.
Understanding these misconceptions can help you navigate the UFT Welfare Fund Contact Form with confidence. Always refer to the official materials for the most accurate information.
Key takeaways
Using the UFT Welfare Fund Contact form effectively can help ensure that your dental claims are processed smoothly. Here are some key takeaways to consider:
- Accurate Information: Fill out all sections carefully. Complete member and patient details to avoid delays. Treat this form as foundational in your claims process.
- Submission Requirement: Pre-treatment estimating and additional x-rays are necessary for specific procedures over $500. Submit these as outlined to expedite your claim.
- Authorization Is Key: Always sign the authorization section. Without your signature, the claim cannot be processed, which means potential out-of-pocket expenses for you.
- Multiple Insurance Plans: If you or your spouse/domestic partner have other dental coverage, include that information. This may affect payment and should be disclosed on the form.
By paying close attention to these details, you will help ensure that your interactions with the UFT Welfare Fund are efficient and effective.
Browse Other Templates
Shiekh Shoes Job Application,Employment Inquiry Form,Shiekh Footwear Career Application,Application for Shiekh Shoes Position,Shiekh Shoes Employment Request,Job Candidate Information Sheet,Shiekh Shoes Hiring Application,Career Opportunity Applicati - Being honest about past convictions can demonstrate transparency and integrity.
Parking Accommodations - Eligible applicants may utilize the placards in various parking scenarios across Texas.