Fill Out Your Va 21 0779 Form
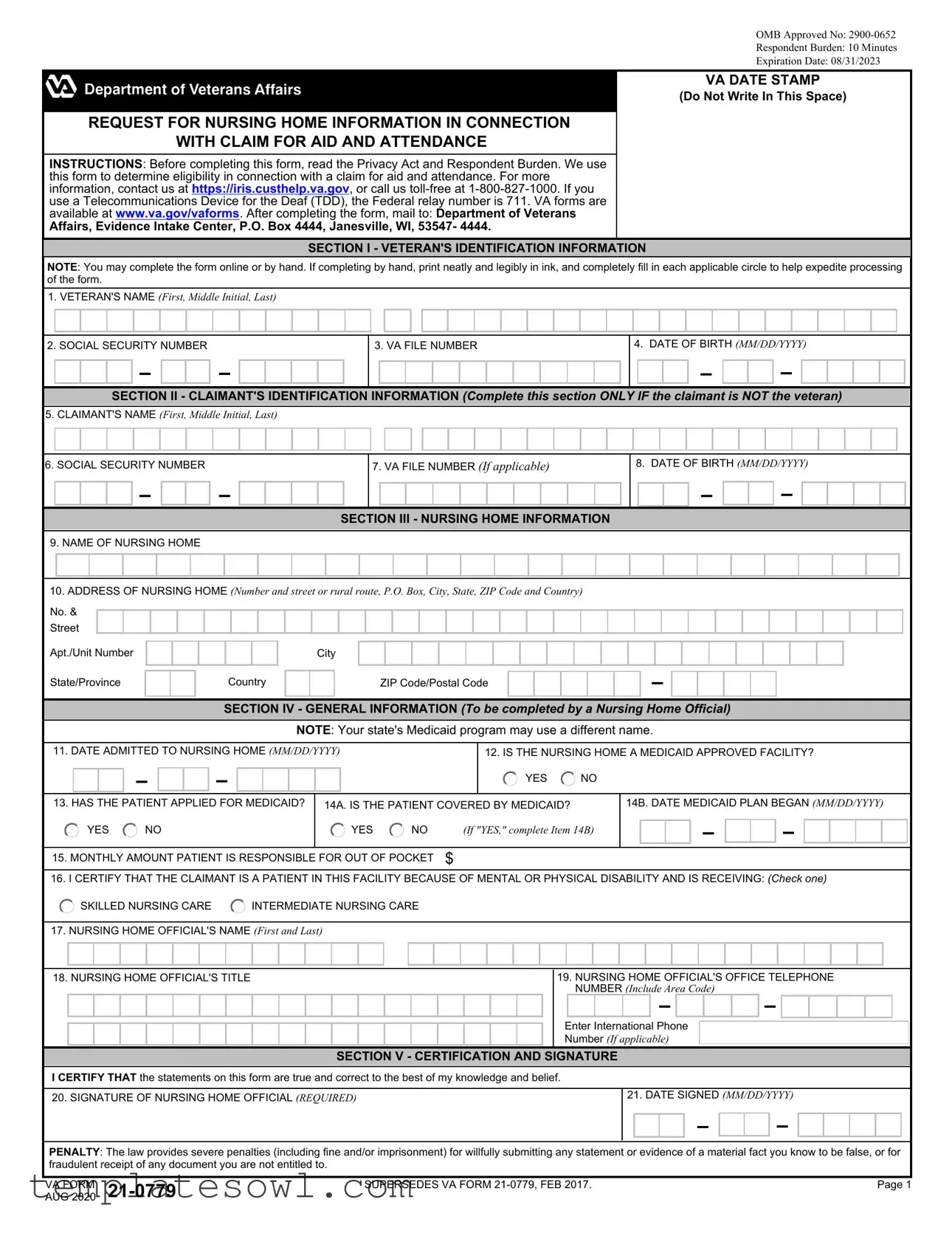
The VA Form 21-0779 serves a critical role in the process of determining a veteran's eligibility for aid and attendance benefits. This form focuses on gathering essential information regarding the nursing home in which the veteran resides. It includes various sections designed to collect identification details for both the veteran and the claimant, alongside specifics about the nursing home facility providing care. Questions on the form inquire about admission dates, Medicaid status, and the nature of care being received, whether skilled or intermediate. Specific instructions emphasize the importance of accurate completion, ensuring that the form is either filled out online or by hand in a legible manner. Completing the VA Form 21-0779 accurately not only aids in expediting processing but also contributes to a fair determination of benefits for those who have served. The Privacy Act Notice highlights the seriousness of maintaining confidentiality while underscoring the consequences of submitting false information. With an estimated completion time of just ten minutes, this form is a vital tool for both nursing home officials and veterans seeking necessary support and resources.
Va 21 0779 Example
OMB Approved No:
Respondent Burden: 10 Minutes
Expiration Date: 08/31/2023
VA DATE STAMP
(Do Not Write In This Space)
REQUEST FOR NURSING HOME INFORMATION IN CONNECTION
WITH CLAIM FOR AID AND ATTENDANCE
INSTRUCTIONS: Before completing this form, read the Privacy Act and Respondent Burden. We use this form to determine eligibility in connection with a claim for aid and attendance. For more information, contact us at https://iris.custhelp.va.gov, or call us
Affairs, Evidence Intake Center, P.O. Box 4444, Janesville, WI, 53547- 4444.
SECTION I - VETERAN'S IDENTIFICATION INFORMATION
NOTE: You may complete the form online or by hand. If completing by hand, print neatly and legibly in ink, and completely fill in each applicable circle to help expedite processing of the form.
1.VETERAN'S NAME (First, Middle Initial, Last)
2. SOCIAL SECURITY NUMBER
3. VA FILE NUMBER
4.DATE OF BIRTH (MM/DD/YYYY)
SECTION II - CLAIMANT'S IDENTIFICATION INFORMATION (Complete this section ONLY IF the claimant is NOT the veteran)
5.CLAIMANT'S NAME (First, Middle Initial, Last)
6. SOCIAL SECURITY NUMBER
7.VA FILE NUMBER (If applicable)
8.DATE OF BIRTH (MM/DD/YYYY)
SECTION III - NURSING HOME INFORMATION
9.NAME OF NURSING HOME
10.ADDRESS OF NURSING HOME (Number and street or rural route, P.O. Box, City, State, ZIP Code and Country)
No. &
Street
Apt./Unit Number
State/Province
Country
City
ZIP Code/Postal Code
SECTION IV - GENERAL INFORMATION (To be completed by a Nursing Home Official)
NOTE: Your state's Medicaid program may use a different name.
11. DATE ADMITTED TO NURSING HOME (MM/DD/YYYY) |
|
|
12. IS THE NURSING HOME A MEDICAID APPROVED FACILITY? |
||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
YES |
NO |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
13. HAS THE PATIENT APPLIED FOR MEDICAID? |
14A. IS THE PATIENT COVERED BY MEDICAID? |
|
14B. DATE MEDICAID PLAN BEGAN (MM/DD/YYYY) |
||||||||||||||||||||||||||||||||
|
YES |
NO |
|
YES |
NO |
(If "YES," complete Item 14B) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
15. MONTHLY AMOUNT PATIENT IS RESPONSIBLE FOR OUT OF POCKET |
$ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
16. I CERTIFY THAT THE CLAIMANT IS A PATIENT IN THIS FACILITY BECAUSE OF MENTAL OR PHYSICAL DISABILITY AND IS RECEIVING: (Check one)
|
SKILLED NURSING CARE |
INTERMEDIATE NURSING CARE |
|||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
17. NURSING HOME OFFICIAL'S NAME (First and Last) |
|||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
18. NURSING HOME OFFICIAL'S TITLE |
|
|
|
|
|
|
|
|
|
|
|
19. NURSING HOME OFFICIAL'S OFFICE TELEPHONE |
|||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NUMBER (Include Area Code) |
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Enter International Phone |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Number (If applicable) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
SECTION V - CERTIFICATION AND SIGNATURE
I CERTIFY THAT the statements on this form are true and correct to the best of my knowledge and belief. |
|
20. SIGNATURE OF NURSING HOME OFFICIAL (REQUIRED) |
21. DATE SIGNED (MM/DD/YYYY) |
PENALTY: The law provides severe penalties (including fine and/or imprisonment) for willfully submitting any statement or evidence of a material fact you know to be false, or for fraudulent receipt of any document you are not entitled to.
VA FORM |
SUPERSEDES VA FORM |
Page 1 |
|
AUG 2020 |
|
|
PRIVACY ACT NOTICE: The VA will not disclose information collected on this form to any source other than what has been authorized under the Privacy Act of 1974 or Title 5, Code of Federal Regulations 1.526 for routine uses (i.e., civil or criminal law enforcement, congressional communications, epidemiological or research studies, the collection of money owed to the United States, litigation in which the United States is a party or has an interest, the administration of VA programs and delivery of VA benefits, verification of identity and status, and personnel administration) as identified in the VA system of records, 58VA21/22/28 Compensation, Pension, Education, and Vocational Rehabilitation and Employment Records - VA, published in the Federal Register. While you are not required to respond, your cooperation in providing this relevant and necessary information will help us determine the claimant's maximum benefit entitlement under the law. Information that you furnish may be utilized in computer matching programs with other Federal or state agencies for the purpose of determining the claimant's eligibility to receive VA benefits, as well as to collect any amount owed to the United States by virtue of the claimant's participation in any benefit program administered by the Department of Veterans Affairs.
RESPONDENT BURDEN: We need this information to determine eligibility for benefits and the proper rate of payment (38 U.S.C. 5503, 38 U.S.C. 1115 (1)(E)), 38 U.S.C. 1311(c), 38 U.S.C. 1315(h)). Title 38, United States Code, allows us to ask for this information. We estimate that you will need an average of 10 minutes to review the instructions, find the information and complete this form. VA cannot conduct or sponsor a collection of information unless a valid OMB control number is displayed. You are not required to respond to a collection of information if this number is not displayed. Valid OMB control numbers can be located on the OMB Internet Page at www.reginfo.gov/public/do/PRAMain. If you desire, you can call
VA FORM |
Page 2 |
Form Characteristics
| Fact Name | Fact Detail |
|---|---|
| OMB Approval Number | OMB Approved No: 2900-0652 |
| Respondent Burden | Estimated at 10 minutes for completion. |
| Expiration Date | This form expired on 08/31/2023. |
| Purpose of Form | This form is used to request nursing home information for claims related to aid and attendance eligibility. |
| Contact Information | For questions, call 1-800-827-1000 or visit https://iris.custhelp.va.gov. |
| Mailing Address | Send completed forms to: Department of Veterans Affairs, Evidence Intake Center, P.O. Box 4444, Janesville, WI, 53547-4444. |
| Privacy Act Notice | Information collected will be governed under the Privacy Act of 1974. |
| Certification Requirement | A nursing home official must sign and date the form to certify the information provided. |
| Governing Laws | This form is governed under Title 38, United States Code. |
Guidelines on Utilizing Va 21 0779
Completing the VA Form 21-0779 involves several steps. This form is essential for gathering information needed to determine eligibility for aid and attendance benefits. Once filled out, the form should be mailed to the designated address provided by the Department of Veterans Affairs.
- Begin by writing the veteran's name in the space provided (First, Middle Initial, Last).
- Enter the social security number of the veteran.
- Provide the VA file number.
- Fill in the date of birth for the veteran in MM/DD/YYYY format.
- If the claimant is not the veteran, complete the claimant's section:
- Write the claimant's name (First, Middle Initial, Last).
- Enter the social security number for the claimant.
- If applicable, provide the VA file number for the claimant.
- Fill in the date of birth for the claimant in MM/DD/YYYY format.
- In the nursing home information section, write the name of the nursing home.
- Provide the address of the nursing home, including street number, apartment/unit number (if any), city, state, ZIP code, and country.
- In the general information section, to be completed by a nursing home official:
- Enter the date admitted to the nursing home in MM/DD/YYYY format.
- Indicate whether the nursing home is a Medicaid approved facility by checking “YES” or “NO.”
- State whether the patient has applied for Medicaid.
- Indicate if the patient is covered by Medicaid.
- If the answer is “YES,” enter the date Medicaid plan began in MM/DD/YYYY format.
- Specify the monthly amount the patient is responsible for out-of-pocket.
- Certify that the claimant is a patient due to mental or physical disability and check the appropriate level of care: skilled nursing care or intermediate nursing care.
- Provide the nursing home official’s name (First and Last).
- Write the official’s title.
- Enter the nursing home official’s office telephone number, including area code. Enter the international phone number if applicable.
- In the certification section, the nursing home official must sign and date the form:
- Provide the signature of the nursing home official.
- Enter the date signed in MM/DD/YYYY format.
After completing each section, double-check all entries for accuracy. Once satisfied, mail the form to the following address: Department of Veterans Affairs, Evidence Intake Center, P.O. Box 4444, Janesville, WI, 53547-4444. It’s important to retain a copy of the completed form for your records, if possible.
What You Should Know About This Form
What is the purpose of the VA 21-0779 form?
The VA 21-0779 form is used to request nursing home information in connection with a claim for aid and attendance benefits. This form helps the Department of Veterans Affairs (VA) determine the eligibility of veterans or claimants who may need additional assistance due to their physical or mental conditions while residing in a nursing home.
Who needs to complete and submit the VA 21-0779 form?
The form must be completed either by the veteran themselves or a designated claimant, such as a family member or legal representative. If completing the form on behalf of the veteran, the claimant's identification information should also be provided. It is essential that all relevant details regarding the nursing home and the patient's Medicaid status are included to facilitate the claim process.
How long does it take to fill out the VA 21-0779 form?
The estimated time to complete the VA 21-0779 form is about 10 minutes. This estimate includes reviewing the instructions, gathering necessary information, and filling out the required sections of the form. However, individuals may need additional time depending on their familiarity with the information required.
Where should the completed VA 21-0779 form be sent?
After completing the form, it should be mailed to the Department of Veterans Affairs, Evidence Intake Center, P.O. Box 4444, Janesville, WI, 53547-4444. It is important to ensure that the form is filled out accurately and completely to prevent delays in processing the claim.
Common mistakes
When filling out the VA Form 21-0779, individuals often overlook important details that can lead to processing delays or even rejection of the application. One common mistake arises in the Veteran’s Identification Information section. Applicants frequently forget to include all required personal details, such as the complete name and Social Security number. Any missing information can create signals that confuse the processing system or necessitate follow-up correspondence, resulting in delays.
Another mistake pertains to the Nursing Home Information section. Individuals may provide incomplete or inaccurate addresses for the nursing home. It is crucial to ensure that the name and address reflect the exact details of the facility. Failure to include the correct city or state can ultimately impede the verification process, thwarting timely access to benefits.
Moreover, in the General Information section, applicants sometimes overlook the importance of providing precise answers regarding Medicaid coverage. Questions such as whether the patient applied for Medicaid or is currently covered must be answered accurately. Incorrect answers may not only hinder eligibility determinations but can also raise questions about the applicant's understanding of the patient's situation.
Lastly, many fail to pay attention to the Certification and Signature section. A common error includes neglecting to have a nursing home official sign the form, or submitting a signature that is not accompanied by the official’s title or contact number. Such oversights can render the application void or incomplete, requiring resubmission and further delay in processing.
Documents used along the form
The VA Form 21-0779 is crucial for veterans seeking assistance with nursing home care benefits. Along with this form, other documents may be required to ensure a streamlined process for veterans applying for aid and attendance benefits. Here are a few forms frequently used alongside VA Form 21-0779:
- VA Form 21-2680: This form, known as the Examination for Housebound Status or Permanent Need for Regular Aid and Attendance, is used to gather medical evidence about the veteran’s needs. It provides crucial information from a physician regarding the veteran’s physical and mental health status, which assists in evaluating the need for aid and attendance benefits.
- VA Form 21-526EZ: This is the Application for Disability Compensation and Related Compensation Benefits form. It is used to apply for disability benefits. When applying for aid and attendance, veterans may need to submit this to ensure that all relevant aspects of their eligibility are considered, especially if they have a disability rating.
- VA Form 21-534EZ: This document, the Application for DIC, Survivors Pension, and Accrued Benefits, is essential when a deceased veteran's surviving spouse or child seeks benefits. In the context of aid and attendance, it helps in assessing continued eligibility for benefits post the veteran's passing.
- VA Form 21-0770: This form is known as the Request for Nursing Home Information in Connection with Claim for Aid and Attendance. It collects similar information as the 21-0779 but focuses on the care needs of the patient, providing a comprehensive look at their eligibility for nursing home care and the benefits that may be available.
Ensuring that all relevant forms are filled out accurately and submitted together can significantly improve the chances of a successful application for aid and attendance benefits. Every detail matters in these situations, and the more complete the submission, the smoother the process will be for everyone involved.
Similar forms
Understanding the VA Form 21-0779, which is used to request nursing home information in relation to claims for aid and attendance, can be made easier by comparing it to other similar documents. Each of these forms serves specific purposes related to veteran care and benefits. Here are four documents that share similarities with the VA Form 21-0779:
- VA Form 21-526EZ - This is the application for disability compensation and related compensation benefits. Like the VA Form 21-0779, it verifies essential information about the veteran and requires claimant details. Both forms ensure that veterans receive the support they are entitled to.
- VA Form 21-534EZ - This application is specifically for survivors seeking Dependency and Indemnity Compensation (DIC) benefits. Similar to the VA Form 21-0779, the 21-534EZ gathers vital identification information and requires specific documentation, in order to establish eligibility for these benefits.
- VA Form 21-550 - This document is used to request miscellaneous benefits and aid for veterans. It also demands careful patient or veteran identification information and relevant details about their circumstances. Consequently, both forms follow a structured process to collect essential data for benefit determination.
- VA Form 21-0972 - This form requests a nursing home’s eligibility to provide services under the VA. It is akin to the VA Form 21-0779 in that it seeks detailed nursing home information for establishing the nature and extent of care provided. This ensures that the veteran’s needs are accurately assessed.
Each of these documents shares a common goal: to facilitate the processing of benefits related to the care and support of veterans and their families. While the specific details may differ, the underlying purpose remains focused on ensuring veterans receive the care and assistance they deserve.
Dos and Don'ts
When filling out the VA Form 21-0779, there are important practices to follow to ensure a smooth application process. Below is a list of dos and don'ts to keep in mind.
- Do read the instructions carefully before beginning the form.
- Do print legibly if you are completing the form by hand.
- Do ensure all relevant sections are filled out completely.
- Do verify that all information is accurate and current.
- Don't leave any applicable circle unfilled.
- Don't use correction fluid or tape on the form; errors should be neatly crossed out.
- Don't forget to sign and date the form before submitting it.
- Don't submit the form without ensuring that all mandatory sections are completed.
Following these guidelines can help prevent delays and ensure that your form is processed efficiently. Take the time needed to complete the form accurately, as this diligence can significantly affect your claim process.
Misconceptions
Misconceptions can often lead to confusion, especially regarding forms like the VA 21 0779. Here’s a breakdown of common misunderstandings:
- It’s only for veterans. Some believe that this form is exclusively for veterans. In fact, it can also be completed by a claimant who is not the veteran, which means family members may fill it out on behalf of veterans.
- Filling it out is complicated. Many think that the form is overly complex. However, it is straightforward, with sections clearly structured for identification and nursing home information.
- Submitting online is not an option. Some assume you can only complete and submit the form by hand. Actually, it can be filled out online for added convenience.
- All nursing homes qualify. A common assumption is that any nursing home can be listed on this form. Not true; the nursing home must be an approved facility to assist in receiving benefits.
- The information is not confidential. People often underestimate the privacy of their details. The information provided is protected under the Privacy Act, ensuring confidentiality.
- Only financial details are necessary. Some individuals think this form solely addresses financial aspects. In reality, it covers medical, personal, and financial information relevant to assessing aid and attendance benefits.
- There’s no penalty for errors. Some believe it’s acceptable to submit the form with mistakes. However, providing false information intentionally can lead to severe penalties.
- It can be submitted at any time. Many think the form can be sent whenever. While it's valid whenever it’s needed, processing may be delayed if sent close to deadlines or without the necessary support documentation.
- Help is not available for completing the form. Lastly, some may feel they must navigate this form independently. Assistance is readily available through the VA’s customer support services, ensuring that help is only a call away.
Understanding these misconceptions can make the process smoother for veterans and their families.
Key takeaways
Filling out the VA 21 0779 form requires careful attention to detail. This form is essential for determining eligibility for aid and attendance benefits.
- The VA 21 0779 form stands for Request for Nursing Home Information in Connection with Claim for Aid and Attendance.
- It is crucial to provide accurate and complete information to expedite the processing of the claim.
- The form can be completed online or by hand. If completed by hand, use ink and print clearly.
- Do not overlook the sections dedicated to the veteran’s and claimant’s identification information.
- Verify the social security numbers and VA file numbers before submission to avoid delays.
- Complete the nursing home information section with thoroughness to ensure accuracy.
- A nursing home official must certify the information in the General Information section.
- Check the appropriate boxes regarding the veteran’s Medicaid status and care needs.
- Understand that submitting false information can result in severe legal penalties.
- After completion, the form should be mailed to the specified address for processing.
Using the VA 21 0779 form accurately is not just a formality; it directly affects the benefits eligibility of the claimant. Take this process seriously and ensure that every detail is correct.
Browse Other Templates
Bankruptcy Proof of Claim Form - The annual interest rate applicable to the secured claim must also be indicated on the form.
Fairbanks Accident Report - Specific street names and highway locations must be noted.