Fill Out Your Vwc No 3 Form
The VWC No 3 form serves as a crucial document in the reporting of workplace injuries under the Virginia Workers’ Compensation Act. It is designed to facilitate the initial reporting process by both employers and claim administrators when an employee sustains an injury during the course of employment. Proper completion of the form ensures that essential information, such as the nature of the accident, details of the injured worker, and specific employer information, is communicated to the Virginia Workers’ Compensation Commission. Key elements include the employer’s legal name, Federal Employer Identification Number (FEIN), and the nature of the business. The form’s structure allows for a comprehensive description of the circumstances surrounding the injury, including the time, place, and cause. Additionally, it includes important dates, such as the date of the injury and the date it was reported. In the event of a fatal incident, the form also requires information about the deceased worker’s marital status and dependent children. Furthermore, the timely submission of this form is mandatory, as not doing so can result in complications with benefits. Another significant aspect is that the form must be accurately filled in by the employer and submitted to the appropriate claim administrator for the insurance provider, ensuring that the details are promptly relayed to the Commission. For those unfamiliar with the requirements, the form features instructions on the reverse side that provide guidance and clarify when and how to appropriately fill it out.
Vwc No 3 Example
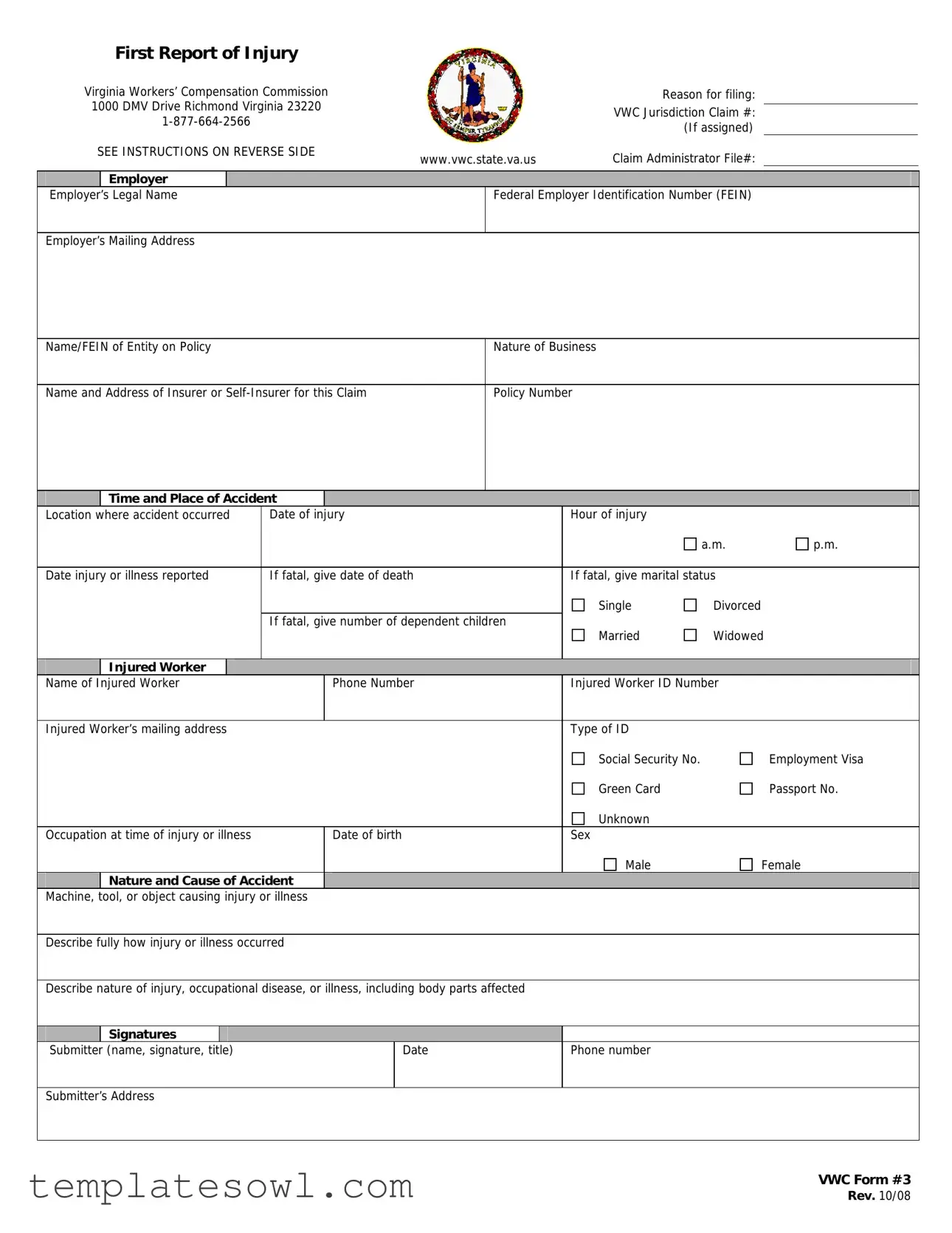
First Report of Injury
Virginia Workers’ Compensation Commission |
|
|
Reason for filing: |
|||
1000 DMV Drive Richmond Virginia 23220 |
|
|
|
|
||
|
|
VWC Jurisdiction Claim #: |
||||
|
|
|||||
|
|
(If assigned) |
|
|||
|
|
|
|
|
||
SEE INSTRUCTIONS ON REVERSE SIDE |
www.vwc.state.va.us |
Claim Administrator File#: |
||||
|
|
|
||||
|
|
|
|
|
|
|
|
Employer |
|
|
|
|
|
Employer’s |
Legal Name |
|
|
Federal Employer Identification Number (FEIN) |
||
|
|
|
|
|
|
|
Employer’s Mailing Address
Name/FEIN of Entity on Policy |
Nature of Business |
|
|
Name and Address of Insurer or |
Policy Number |
|
Time and Place of Accident |
|
|
|
|
||
Location |
where accident occurred |
Date of injury |
Hour of injury |
|
|
||
|
|
|
|
|
|
a.m. |
p.m. |
|
|
|
|
|
|||
Date injury or illness reported |
If fatal, give date of death |
If fatal, give marital status |
|
||||
|
|
|
|
|
Single |
Divorced |
|
|
|
|
If fatal, give number of dependent children |
Married |
Widowed |
||
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
Injured Worker |
|
|
|
|
|
|
Name of |
Injured Worker |
|
|
Phone Number |
Injured Worker ID Number |
|
|
|
|
|
|
|
|
||
Injured Worker’s mailing address |
|
|
Type of ID |
|
|
||
|
|
|
|
|
Social Security No. |
|
Employment Visa |
|
|
|
|
|
Green Card |
|
Passport No. |
|
|
|
|
|
Unknown |
|
|
Occupation at time of injury or illness |
|
Date of birth |
Sex |
|
|
||
|
|
|
|
|
Male |
|
Female |
Nature and Cause of Accident
Machine, tool, or object causing injury or illness
Describe fully how injury or illness occurred
Describe nature of injury, occupational disease, or illness, including body parts affected
Signatures |
|
|
Submitter (name, signature, title) |
Date |
Phone number |
Submitter’s Address
VWC Form #3
Rev. 10/08
First Report of Injury
Filing Instructions
The Virginia Workers’ Compensation Act requires that ALL injuries occurring in the course of employment be reported to the Commission pursuant to Va. Code
Employer
The employer is responsible for accurately completing all sections of this form when an employee is injured. It should be typed or legibly printed, signed, and dated by the preparer. Send the original form to the claim administrator for the insurance company who provided insurance coverage on the date of the occurrence. The claim administrator will report this information to the Commission.
Contact your workers’ compensation insurance provider for additional information.
Claim Administrator
Claim administrators who are EDI enabled will use the information contained on the paper form and submit electronic data to the Commission.
Claim administrators who are NOT EDI enabled must immediately file the completed form with the Commission. Please note: EDI is mandatory no later than June 30, 2009, after which time paper reports will no longer be accepted. Until you are in EDI production, mail the completed form to the Virginia Workers’ Compensation Commission, 1000 DMV Drive, Richmond, VA 23220. At the top of the form, use a numerical code
For questions or assistance in completing the form, please contact the Commission
*Criteria for filing are: (1) lost time exceeds seven days; (2) medical expenses exceed $1,000.00; (3) compensability is denied; (4) issues are disputed; (5) accident resulted in death; (6) permanent disability or disfigurement may be involved; and (7) a specific request is made by the Virginia Workers’ Compensation Commission.
Form Characteristics
| Fact Name | Details |
|---|---|
| Name of Form | VWC No 3 - First Report of Injury |
| Purpose | This form is used to report injuries occurring in the course of employment in Virginia. |
| Governing Law | Virginia Workers’ Compensation Act, specifically Va. Code §65.2-900. |
| Submission Details | The form must be submitted to the claim administrator for the insurance company on the date of the incident. |
| Claim Administrator | Claim administrators who are EDI enabled must use the form data to submit electronically. Otherwise, they must file the form directly with the Commission. |
| Information Required | The form requires details like employer information, injured worker's data, nature of the injury, and circumstances of the accident. |
| Filing Instructions | Contact the Virginia Workers’ Compensation Commission toll-free at 877-664-2566 for assistance or questions regarding the form. |
| Filing Criteria | Accidents must be reported if they meet certain criteria, such as causing lost time exceeding seven days or resulting in medical expenses over $1,000. |
| Form Revision | The current version of the VWC No 3 form was revised in October 2008. |
Guidelines on Utilizing Vwc No 3
After you gather the necessary information, you will fill out the VWC No. 3 form to report an injury that occurred during employment. Each section must be completed accurately to ensure proper handling of the claim. Below are the steps for filling out the form.
- Begin with Claim Information: Write down the VWC jurisdiction claim number, if assigned, in the designated box.
- Provide Employer Details: Fill in the employer’s legal name, Federal Employer Identification Number (FEIN), and mailing address.
- Insurer Information: Enter the name and address of the insurance company or self-insurer covering the claim, along with the policy number.
- Accident Details: Note the time and place of the accident, including the date and the hour. Specify if it was a.m. or p.m.
- Report Injury Date: Indicate the date when the injury or illness was reported to the employer.
- Fatality Information: If applicable, provide the date of death and the marital status of the injured worker, as well as the number of dependent children.
- Injured Worker’s Personal Information: Write the name, phone number, and mailing address of the injured worker. Also, include their identification type and number (e.g., Social Security No., Employment Visa, etc.).
- Occupation Details: Fill in the injured worker’s occupation at the time of the injury and their date of birth. Indicate the sex of the injured worker.
- Accident Description: Describe the machine, tool, or object causing the injury. Fully explain how the injury or illness occurred, including details about the nature of the injury, occupational disease, or illness and the body parts affected.
- Signatures: The preparer of the form must write their name, sign, and provide their title along with the date and phone number. Ensure to include the submitter’s mailing address.
Once you have completed the form, it must be submitted for processing. Remember to check if your claim administrator is EDI enabled. If not, mail the original form to the Virginia Workers’ Compensation Commission at the provided address. Make sure to keep a copy for your records.
What You Should Know About This Form
What is the purpose of the Vwc No 3 form?
The Vwc No 3 form, known as the First Report of Injury, is used to report work-related injuries or illnesses to the Virginia Workers’ Compensation Commission. Employers must file this form when an injury occurs in the course of employment to ensure compliance with Virginia Workers’ Compensation Act.
Who is responsible for completing the form?
The employer is responsible for accurately completing all sections of the Vwc No 3 form when an employee is injured. The information should be typed or legibly printed, signed, and dated by the individual preparing the report.
What should I do after completing the form?
Once the form has been completed, the original should be sent to the claim administrator for the insurance company that provided coverage on the date of the accident. The claim administrator will then report this information to the Commission.
What if the claim administrator is not EDI enabled?
If the claim administrator is not EDI enabled, the completed Vwc No 3 form must be filed directly with the Virginia Workers’ Compensation Commission. This should be done as soon as possible to ensure timely processing.
What is the timeline for filing the Vwc No 3 form?
The form should be submitted promptly after the injury occurs. The Virginia Workers’ Compensation Act requires that all injuries are reported to the Commission regardless of the insurer's status. Delays in reporting could affect claim processing.
How do I indicate the reason for filing the form?
At the top of the Vwc No 3 form, use a numerical code from 1 to 7 to indicate the reason for filing. These numbers correspond to specific filing criteria related to the nature and impact of the injury. If none apply, simply leave the "reason for filing" section blank.
What are the criteria for filing this form?
The form must be filed if any of the following apply: lost time exceeds seven days, medical expenses exceed $1,000, compensability is denied, there are disputed issues, the accident resulted in death, permanent disability or disfigurement may occur, or a specific request is made by the Commission.
What information must be included in the form?
Essential information includes details about the injured worker, such as name, phone number, occupation, and nature of the injury. Employers should also report the time and place of the accident, as well as a full description of how the injury occurred.
What should I do if I have questions while completing the form?
If there are any questions or if assistance is needed while completing the Vwc No 3 form, contact the Virginia Workers’ Compensation Commission at their toll-free number, 1-877-664-2566. They can provide guidance and support for the filing process.
Can I use another form instead of the Vwc No 3 form?
If the criteria for filing do not apply, you may still report the accident but can use either the Vwc No 3 form or Form 45A to do so. It is important to ensure that all required information is submitted to facilitate proper reporting.
Common mistakes
Completing the VWC No 3 form accurately is crucial for ensuring that injury claims are processed smoothly. However, many individuals make mistakes that can lead to delays or complications. One common error occurs when the reason for filing the form is not clearly indicated. Individuals often leave this section blank or select an inappropriate numerical code. Without a proper reason, the form may not be processed in a timely manner, causing frustration for both the injured worker and the employer.
Another frequent mistake is failing to provide comprehensive details in the injury description section. Specifically, individuals may abbreviate or omit important information about the nature of the injury or the circumstances leading up to it. A lack of clarity leaves the form open to misinterpretation. This situation can complicate the claims process and affect the injured worker's ability to receive benefits.
Incorrectly listing the employer’s information can also hinder the processing of the claim. For instance, using an outdated address or an incorrect Federal Employer Identification Number (FEIN) can lead to significant issues. Since the form must be sent directly to the claim administrator based on the information provided, ensuring accuracy is essential. Any discrepancies may result in delays or rejections of the claim, leading to unnecessary complications.
Lastly, signatures and dates are often overlooked. The submitter’s name, title, signature, and date must be provided to validate the document. Omitting any of these elements can render the form incomplete. This mistake not only prolongs the filing process, but it can also immediately halt any progress on the claim, adding further stress to all parties involved.
Documents used along the form
The VWC No 3 form is an essential document for reporting workplace injuries in Virginia. Several other forms and documents may be used in conjunction with this form to ensure all necessary information is submitted correctly.
- VWC Form 45A: This form is used when the required criteria for filing the VWC No 3 form do not apply. It allows for the reporting of any workplace accident even if the circumstances do not meet specific reporting guidelines.
- Claim Administrator Report: This report details the insurance company’s assessment of the claim. It includes information about the claim status and any actions taken, serving as an important communication tool between the employer, the injured worker, and the insurance provider.
- Worker's Compensation Insurance Policy: This document outlines the coverage provided by the employer's insurance policy. It includes details about the policy terms, premium costs, and any exclusions that might affect the injured worker’s claim.
- Injury Medical Report: This report is generated by the healthcare provider who treated the injured worker. It documents the nature of the injury, treatment provided, and any prognosis, which is vital for the claims process.
- Notice of Claim Acceptance or Denial: This document is issued by the claim administrator once a decision is made regarding the claim. It formally communicates whether the claim has been accepted or denied and outlines the reasons for the decision.
Utilizing these additional forms and documents helps to streamline the workers' compensation claims process, ensuring that all relevant information is available for proper evaluation and resolution.
Similar forms
-
First Report of Injury (FROI): Like the VWC No 3 form, the FROI is used to notify the workers’ compensation authority about an employment-related injury or illness. Both forms require detailed information about the incident, the injured worker, and the employer.
-
Claim Investigation Form: This document shares similarities with the VWC No 3 form, as it gathers comprehensive details about the injury or illness for insurance claims. Both forms aim to document critical information required for processing claims.
-
Employee Incident Report: This report is also focused on documenting workplace injuries. It requires specifics about what occurred, similar to the information captured in the VWC No 3 form, ensuring consistency in reporting across different forms.
-
Employer's Report of Injury: This document aligns closely with the VWC No 3, as it is completed by the employer following an injury. Both forms solicit substantial data regarding the incident in order to establish the context and facts surrounding the claim.
-
Workers’ Compensation Claim Form: This form is ultimately a claim for benefits resulting from work-related injuries. While the VWC No 3 form is for reporting, both documents will collect similar essential details that are critical for determining eligibility and compensation.
-
Medical Report of Work-Related Injury: As with the VWC No 3, this report provides insight into the nature and extent of injuries. It often supplements the claims process, ensuring that detailed medical assessments are aligned with the information reported by the employer.
Dos and Don'ts
- Do ensure that all sections of the VWC No 3 form are filled out accurately.
- Do type or print legibly to avoid confusion or errors in processing.
- Do submit the original form to the claim administrator in a timely manner.
- Do check the option that best explains the reason for filing the form.
- Don't leave any sections blank; complete every part of the form.
- Don't use outdated forms; ensure you have the most recent version.
- Don't hesitate to contact the Virginia Workers’ Compensation Commission if assistance is needed.
Misconceptions
Misconceptions about the VWC No 3 form can lead to mistakes in reporting workplace injuries. Below are seven common misconceptions explained.
- The VWC No 3 form is only for severe injuries. Many believe this form is only needed for critical incidents. In reality, it must be used for all workplace injuries, regardless of severity.
- Only the injured worker should file the form. It is a common misconception that only employees can submit the VWC No 3 form. The employer is actually responsible for completing and submitting it.
- Filing the form is optional. Some think the VWC No 3 form is optional. However, it is mandated by the Virginia Workers’ Compensation Act for all work-related injuries.
- The form does not have a deadline. A prevalent belief is that the deadline for submission is flexible. However, it must be submitted promptly after an injury occurs to ensure compliance and timely processing.
- Information on the form can be completed vaguely. Many assume that providing general details is sufficient. The form requires specific information about the incident and the injured worker.
- All claims are automatically approved. Some individuals may think that submitting the VWC No 3 form guarantees claim approval. Actual decisions depend on the details and circumstances of the injury.
- The form can be submitted electronically or as a paper form interchangeably. There is a misconception regarding the submission format. Claim administrators must adhere to electronic reporting requirements, with paper submissions only allowed under specific conditions.
Understanding these misconceptions is vital for ensuring accurate reporting of workplace injuries in Virginia.
Key takeaways
Understanding the VWC No. 3 form is essential for employers and employees navigating the workers' compensation system in Virginia. Here are key takeaways regarding this important document:
- Timely Reporting is Crucial: The form must be completed and submitted without delay if an employee suffers an injury in the course of their work. Timeliness helps ensure that claims are processed efficiently and that injured workers receive the benefits they deserve.
- Accurate Completion Matters: Employers are responsible for filling out the form accurately. Each section should be completed with care, as inaccuracies can lead to delays in the claims process.
- Submission Procedures: After completing the form, send the original to the claim administrator associated with the employer’s workers' compensation insurance. If the claim administrator is not EDI enabled, the form must be filed directly with the Virginia Workers' Compensation Commission.
- Categorizing the Claim: At the top of the form, a numerical code (1-7) must be used to indicate the reason for filing. This coding assists in categorizing the claim and triggers the appropriate procedures.
- Seek Assistance When Needed: For assistance in completing the VWC No. 3 form, employers and employees should not hesitate to contact the Virginia Workers’ Compensation Commission by calling 877-664-2566. Engaging with the Commission can clarify doubts and enhance the accuracy of the submission.
In summary, the effective use of the VWC No. 3 form is a critical component of managing workers' compensation claims in Virginia, benefiting both employers and employees alike.
Browse Other Templates
Small Business Workers Compensation Insurance Companies - The U-26.3 form is a certificate indicating workers' compensation coverage in New York State.
Life Insurance Change Request Form,Universal Change Notification Form,Beneficiary Update Request Form,Life Policy Modification Form,Ownership Transfer Form,Contact Information Update Form,Coverage Adjustment Request Form,Insurance Account Modificatio - This form must be signed and dated before submission to 5Star Life for processing.