Fill Out Your Workers Compensation Injury Report Form
In the realm of workplace safety and employee rights, the Workers' Compensation Injury Report form serves as an essential document that facilitates the reporting of work-related injuries or illnesses. This form collects a wealth of information regarding the incident, starting from the employer’s details, which include the name, address, and policy information, down to specifics about the injured worker. Within its confines, it prompts the collection of crucial data such as the employee’s name, birth date, occupation, and employment status. The form further requires information about the incident itself—detailing the time and date of the occurrence, the nature of the injury, and the specific part of the body affected. Employers must specify whether safety equipment was in place and used at the time of the incident, while also giving a comprehensive description of how the injury occurred. This structured approach assists in evaluating claims for benefits and aids in ensuring that workers receive the necessary support for recovery. Additionally, it contains legal warnings about the repercussions of fraudulent claims, highlighting the importance of accuracy and honesty in the completion of this form. Understanding the various components within this report is vital for both employers and employees navigating the complexities of workplace injuries.
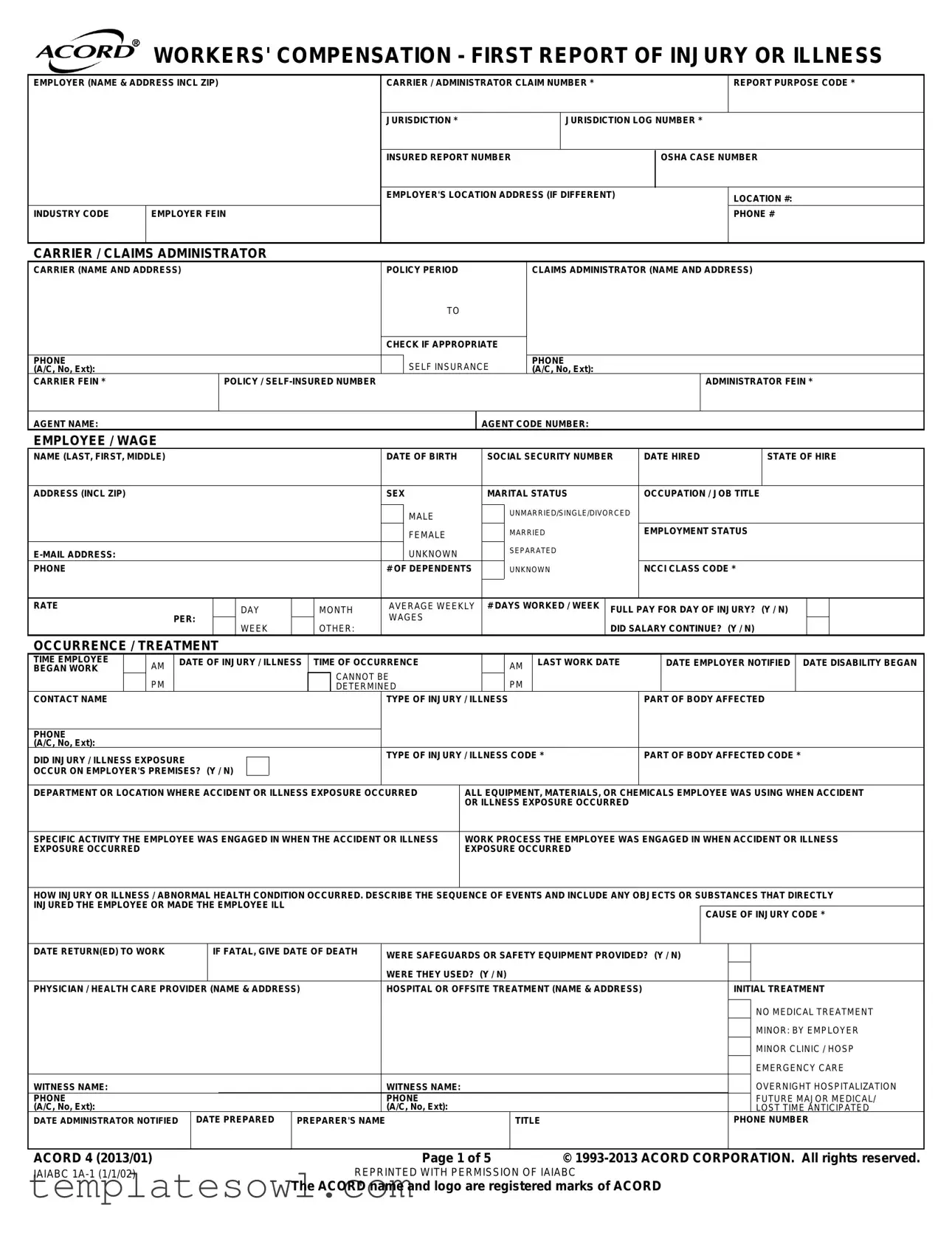
Workers Compensation Injury Report Example
WORKERS' COMPENSATION - FIRST REPORT OF INJURY OR ILLNESS
EMPLOYER (NAME & ADDRESS INCL ZIP) |
CARRIER / ADMINISTRATOR CLAIM NUMBER * |
|
REPORT PURPOSE CODE * |
||
|
|
|
|
|
|
|
|
JURISDICTION * |
JURISDICTION LOG NUMBER * |
||
|
|
|
|
|
|
|
|
INSURED REPORT NUMBER |
|
OSHA CASE NUMBER |
|
|
|
|
|
|
|
|
|
EMPLOYER'S LOCATION ADDRESS (IF DIFFERENT) |
|
LOCATION #: |
|
|
|
|
|
|
|
INDUSTRY CODE |
EMPLOYER FEIN |
|
|
|
PHONE # |
|
|
|
|
|
|
CARRIER / CLAIMS ADMINISTRATOR
CARRIER (NAME AND ADDRESS) |
POLICY PERIOD |
CLAIMS ADMINISTRATOR (NAME AND ADDRESS) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CHECK IF APPROPRIATE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PHONE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SELF INSURANCE |
|
|
|
PHONE |
|
|
|
|
|
|
|
|
|
|
|
||||||
(A/C, No, Ext): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(A/C, No, Ext): |
|
|
|
|
|
|
|
|
|
|
|
|||||||
CARRIER FEIN * |
|
|
|
|
|
|
POLICY / |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ADMINISTRATOR FEIN * |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
AGENT NAME: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
AGENT CODE NUMBER: |
|
|
|
|
|
|
|
|
|
|
|
||||||
EMPLOYEE / WAGE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
NAME (LAST, FIRST, MIDDLE) |
|
|
|
|
|
|
|
|
|
|
|
|
|
DATE OF BIRTH |
|
|
SOCIAL SECURITY NUMBER |
|
DATE HIRED |
|
|
|
STATE OF HIRE |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
ADDRESS (INCL ZIP) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SEX |
|
|
MARITAL STATUS |
|
|
OCCUPATION / JOB TITLE |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MALE |
|
|
|
|
UNMARRIED/SINGLE/DIVORCED |
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FEMALE |
|
|
|
|
MARRIED |
|
|
EMPLOYMENT STATUS |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
UNKNOWN |
|
|
|
|
SEPARATED |
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
PHONE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
# OF DEPENDENTS |
|
|
UNKNOWN |
|
|
NCCI CLASS CODE * |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RATE |
|
|
|
|
|
|
|
DAY |
|
|
MONTH |
|
AVERAGE WEEKLY |
# DAYS WORKED / WEEK |
FULL PAY FOR DAY OF INJURY? (Y / N) |
|
|
|||||||||||||||||||||
|
|
|
PER: |
|
|
|
|
|
WAGES |
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
WEEK |
|
|
OTHER: |
|
|
|
|
|
|
|
|
|
DID SALARY CONTINUE? (Y / N) |
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
OCCURRENCE / TREATMENT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
TIME EMPLOYEE |
|
AM |
|
DATE OF INJURY / ILLNESS |
|
TIME OF OCCURRENCE |
|
|
|
|
AM |
|
|
LAST WORK DATE |
|
DATE EMPLOYER NOTIFIED |
DATE DISABILITY BEGAN |
|||||||||||||||||||||
BEGAN WORK |
|
|
|
|
|
|
|
|
|
|
|
|
|
CANNOT BE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
PM |
|
|
|
|
|
|
|
|
|
|
|
|
DETERMINED |
|
|
|
|
PM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
CONTACT NAME |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TYPE OF INJURY / ILLNESS |
|
|
|
|
|
|
PART OF BODY AFFECTED |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PHONE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(A/C, No, Ext): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DID INJURY / ILLNESS EXPOSURE |
|
|
|
|
|
|
|
TYPE OF INJURY / ILLNESS CODE * |
|
|
PART OF BODY AFFECTED CODE * |
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
OCCUR ON EMPLOYER'S PREMISES? (Y / N) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||
DEPARTMENT OR LOCATION WHERE ACCIDENT OR ILLNESS EXPOSURE OCCURRED |
|
ALL EQUIPMENT, MATERIALS, OR CHEMICALS EMPLOYEE WAS USING WHEN ACCIDENT |
||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OR ILLNESS EXPOSURE OCCURRED |
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
||||||||||||||||||||||||||||||||||
SPECIFIC ACTIVITY THE EMPLOYEE WAS ENGAGED IN WHEN THE ACCIDENT OR ILLNESS |
|
WORK PROCESS THE EMPLOYEE WAS ENGAGED IN WHEN ACCIDENT OR ILLNESS |
||||||||||||||||||||||||||||||||||||
EXPOSURE OCCURRED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EXPOSURE OCCURRED |
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|||||||||||||||||||||||||||||||||||
HOW INJURY OR ILLNESS / ABNORMAL HEALTH CONDITION OCCURRED. DESCRIBE THE SEQUENCE OF EVENTS AND INCLUDE ANY OBJECTS OR SUBSTANCES THAT DIRECTLY |
||||||||||||||||||||||||||||||||||||||
INJURED THE EMPLOYEE OR MADE THE EMPLOYEE ILL |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CAUSE OF INJURY CODE * |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
DATE RETURN(ED) TO WORK |
|
|
|
IF FATAL, GIVE DATE OF DEATH |
|
WERE SAFEGUARDS OR SAFETY EQUIPMENT PROVIDED? (Y / N) |
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
WERE THEY USED? (Y / N) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
PHYSICIAN / HEALTH CARE PROVIDER (NAME & ADDRESS) |
|
|
|
HOSPITAL OR OFFSITE TREATMENT (NAME & ADDRESS) |
|
|
|
INITIAL TREATMENT |
||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NO MEDICAL TREATMENT |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MINOR: BY EMPLOYER |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MINOR CLINIC / HOSP |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EMERGENCY CARE |
||||
WITNESS NAME: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
WITNESS NAME: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OVERNIGHT HOSPITALIZATION |
|||||||
PHONE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PHONE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FUTURE MAJOR MEDICAL/ |
|||||||
(A/C, No, Ext): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(A/C, No, Ext): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LOST TIME ANTICIPATED |
|||||||
DATE ADMINISTRATOR NOTIFIED |
|
DATE PREPARED |
PREPARER'S NAME |
|
|
|
|
|
|
|
TITLE |
|
|
|
|
|
PHONE NUMBER |
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
ACORD 4 (2013/01) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Page 1 of 5 |
|
|
|
© |
|||||||||||||||||||
IAIABC |
|
|
|
|
|
|
|
|
|
|
|
|
|
REPRINTED WITH PERMISSION OF IAIABC |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
The ACORD name and logo are registered marks of ACORD |
|
|
|
|
|
|
|
|||||||||||||||||||
APPLICABLE IN ALABAMA
Any person who knowingly presents a false or fraudulent claim for payment of a loss or benefit or who knowingly presents false information in an application for insurance is guilty of a crime and may be subject to restitution fines or confinement in prison, or any combination thereof.
APPLICABLE IN ALASKA
A person who knowingly and with intent to injure, defraud, or deceive an insurance company files a claim containing false, incomplete, or misleading information may be prosecuted under state law.
APPLICABLE IN ARIZONA
For your protection, Arizona law requires the following statement to appear on this form. Any person who knowingly presents a false or fraudulent claim for payment of a loss is subject to criminal and civil penalties.
APPLICABLE IN ARKANSAS
Any person or entity who willfully and knowingly makes any material false statement or representation or who willfully and knowingly omits or conceals any material information, or who willfully and knowingly employs any device, scheme or artifice for the purpose of obtaining any benefit or payment, or for the purpose of defeating or wrongfully decreasing any claim for benefit or payment or obtaining or avoiding workers' compensation coverage or avoiding payment of the proper insurance premium (or who aids and abets for either said purpose), under this chapter shall be guilty of a Class D. felony.
APPLICABLE IN CALIFORNIA
Any person who makes or causes to be made any knowingly false or fraudulent material statement or material representation for the purpose of obtaining or denying workers compensation benefits or payments is guilty of a felony.
APPLICABLE IN COLORADO
It is unlawful to knowingly provide false, incomplete, or misleading facts or information to an insurance company for the purpose of defrauding or attempting to defraud the company. Penalties may include imprisonment, fines, denial of insurance, and civil damages. Any insurance company or agent of an insurance company who knowingly provides false, incomplete, or misleading facts or information to a policy holder or claimant for the purpose of defrauding or attempting to defraud the policy holder or claimant with regard to a settlement or award payable from insurance proceeds shall be reported to the Colorado Division of Insurance within the Department of Regulatory Agencies.
APPLICABLE IN CONNECTICUT
This form must be completed in its entirety. Any person who intentionally misrepresents or intentionally fails to disclose any material fact related to a claimed injury may be guilty of a felony.
APPLICABLE IN DELAWARE AND OKLAHOMA
Any person who knowingly and with intent to injure, defraud, or deceive any Insurer, files a statement of claim containing any false, incomplete or misleading information is guilty of a felony. The lack of such a statement shall not constitute a defense against prosecution under this section. *Delaware Statutes Regulations: Del #C Section 913(B)
APPLICABLE IN THE DISTRICT OF COLUMBIA
Warning: It is a crime to provide false or misleading information to an insurer for the purpose of defrauding the insurer or any other person. Penalties include imprisonment and/or fines. In addition, an insurer may deny insurance benefits, if false information materially related to a claim was provided by the applicant.
APPLICABLE IN FLORIDA
Pursuant to S. 817.234, Florida Statutes, any person who, with the intent to injure, defraud, or deceive any insurer or insured, prepares, presents, or causes to be presented a proof of loss or estimate of cost or repair of damaged property in support of a claim under an insurance policy knowing that the proof of loss or estimate of claim or repairs contains any false, incomplete, or misleading information concerning any fact or thing material to the claim commits a felony of the third degree, punishable as provided in
S. 775.082, S. 775.083, or S. 775.084, Florida Statutes.
APPLICABLE IN HAWAII
For your protection, Hawaii law requires you to be informed that presenting a fraudulent claim for payment of a loss or benefit is a crime punishable by fines or imprisonment, or both.
EMPLOYEE SIGNATURE:
ACORD 4 (2013/01) |
Page 2 of 5 |
APPLICABLE IN IDAHO
Any person who knowingly and with the intent to injure, Defraud, or Deceive any Insurance Company Files a Statement of Claim Containing any False, Incomplete or Misleading information is Guilty of a Felony.
APPLICABLE IN INDIANA
A person who knowingly and with intent to defraud an insurer files a statement of claim containing any false, incomplete, or misleading information commits a felony.
APPLICABLE IN KANSAS
Any person who, knowingly and with intent to defraud, presents, causes to be presented or prepares with knowledge or belief that it will be presented to or by an insurer, purported insurer, broker or any agent thereof, any written statement as part of, or in support of, an application for the issuance of, or the rating of an insurance policy for personal or commercial insurance, or a claim for payment or other benefit pursuant to an insurance policy for commercial or personal insurance which such person knows to contain materially false information concerning any fact material thereto; or conceals, for the purpose of misleading, information concerning any fact material thereto commits a fraudulent insurance act.
APPLICABLE IN KENTUCKY, LOUISIANA, MAINE, MICHIGAN, NEW JERSEY, NEW MEXICO, NEW YORK, NORTH DAKOTA, PENNSYLVANIA, RHODE ISLAND, SOUTH DAKOTA, VIRGINIA AND WEST VIRGINIA
Any person who knowingly and with intent to defraud any insurance company or another person files a statement of claim containing any materially false information, or conceals for the purpose of misleading, information concerning any fact material thereto, commits a fraudulent insurance act, which is a crime, and subjects the person to criminal and [NY: substantial] civil penalties. In LA, ME and VA, insurance benefits may also be denied.
APPLICABLE IN MARYLAND
Any person who knowingly or willfully presents a false or fraudulent claim for payment of a loss or benefit or who knowingly or willfully presents false information in an application for insurance is guilty of a crime and may be subject to fines and confinement in prison.
APPLICABLE IN MINNESOTA
A person who files a claim with intent to defraud or helps commit a fraud against an insurer is guilty of a crime.
APPLICABLE IN NEVADA
Pursuant to NRS 686A.291, any person who knowingly and willfully files a statement of claim that contains any false, incomplete or misleading information concerning a material fact is guilty of a felony.
APPLICABLE IN NEW HAMPSHIRE
Any person who, with purpose to injure, defraud or deceive any insurance company, files a statement of claim containing any false, incomplete or misleading information is subject to prosecution and punishment for insurance fraud, as provided in RSA 638:20.
APPLICABLE IN OHIO
Any person who, with intent to defraud or knowing that he/she is facilitating a fraud against an insurer, submits an application or files a claim containing a false or deceptive statement is guilty of insurance fraud.
APPLICABLE IN TENNESSEE
It is a crime to knowingly provide false, incomplete or misleading information to any party to a workers compensation transaction for the purpose of committing fraud. Penalties include imprisonment, fines and denial of insurance benefits.
APPLICABLE IN TEXAS
Any person who knowingly presents a false or fraudulent claim for the payment of a loss is guilty of a crime and may be subject to fines and confinement in state prison.
APPLICABLE IN UTAH
Any person who knowingly presents false or fraudulent underwriting information, files or causes to be filed a false or fraudulent claim for disability compensation or medical benefits, or submits a false or fraudulent report or billing for health care fees or other professional services is guilty of a crime and may be subject to fines and confinement in state prison.
APPLICABLE IN WASHINGTON
It is a crime to knowingly provide false, incomplete, or misleading information to an insurance company for the purpose of defrauding the company. Penalties include imprisonment, fines and denial of insurance benefits.
EMPLOYEE SIGNATURE:
ACORD 4 (2013/01) |
Page 3 of 5 |
EMPLOYER'S INSTRUCTIONS
DO NOT ENTER DATA IN FIELDS MARKED *
DATES:
Enter all dates in MM/DD/YY format.
INDUSTRY CODE:
This is the code which represents the nature of the employer's business which is contained in the Standard Industrial Classification Manual or the North American Industry Classification System published by the Federal Office of Management and Budget.
OSHA CASE NUMBER:
Transfer the case number from the OSHA 300 log after you record the case there.
CARRIER:
The licensed business entity issuing a contract of insurance and assuming financial responsibility on behalf of the employer of the claimant.
CLAIMS ADMINISTRATOR:
Enter the name of the carrier, third party administrator, state fund, or
AGENT NAME & CODE NUMBER:
Enter the name of your insurance agent and his/her code number if known. This information can be found on your insurance policy.
OCCUPATION / JOB TITLE:
This is the primary occupation of the claimant at the time of the accident or exposure.
EMPLOYMENT STATUS: |
|
|
|
Indicate the employee's work status. The valid choices are: |
|
||
On Strike |
Unknown |
Volunteer |
|
Disabled |
Apprenticeship |
Seasonal |
|
Not Employed |
Retired |
Apprenticeship |
Piece Worker |
DATE DISABILITY BEGAN:
The first day on which the claimant originally lost time from work due to the occupation injury or disease or as otherwise deigned by statute.
CONTACT NAME / PHONE NUMBER:
Enter the name of the individual at the employer's premises to be contacted for additional information.
TYPE OF INJURY / ILLNESS:
Briefly describe the nature of the injury or illness, (eg. Lacerations to the forearm).
PART OF BODY AFFECTED:
Indicate the part of body affected by the injury/illness, (eg. Right forearm, lower back).
DEPARTMENT OR LOCATION WHERE ACCIDENT OR ILLNESS EXPOSURE OCCURRED: (eg. Maintenance Department or Client's office at 452 Monroe St., Washington, DC 26210)
If the accident or illness exposure did not occur on the employer's premises, enter address or location. Be specific.
ACORD 4 (2013/01) |
Page 4 of 5 |
ALL EQUIPMENT, MATERIAL OR CHEMICALS EMPLOYEE WAS USING WHEN ACCIDENT OR ILLNESS EXPOSURE OCCURRED:
(eg. Acetylene cutting torch, metal plate)
List all of the equipment, materials, and/or chemicals the employee was using, applying, handling or operat- ing when the injury or illness occurred. Be specific, for example: decorator's scaffolding, electric sander, paintbrush, and paint.
Enter "NA" for not applicable if no equipment, materials, or chemicals were being used. NOTE: The items listed do not have to be directly involved in the employee's injury or illness.
SPECIFIC ACTIVITY THE EMPLOYEE WAS ENGAGED IN WHEN THE ACCIDENT OR ILLNESS EXPOSURE OCCURRED:
(eg. Cutting metal plate for flooring)
Describe the specific activity the employee was engaged in when the accident or illness exposure occurred, such as sanding ceiling woodwork in preparation for painting.
WORK PROCESS THE EMPLOYEE WAS ENGAGED IN WHEN ACCIDENT OR ILLNESS EXPOSURE OCCURRED: Describe the work process the employee was engaged in when the accident or illness exposure occurred, such as building maintenance. Enter "NA" for not applicable if employee was not engaged in a work process (eg. walking along a hallway).
HOW INJURY OR ILLNESS / ABNORMAL HEALTH CONDITION OCCURRED. DESCRIBE THE SEQUENCE OF EVENTS AND INCLUDE ANY OBJECTS OR SUBSTANCES THAT DIRECTLY INJURED THE EMPLOYEE OR MADE THE EMPLOYEE ILL:
(Worker stepped back to inspect work and slipped on some scrap metal. As worker fell, worker brushed against the hot metal.)
Describe how the injury or illness / abnormal health condition occurred. Include the sequence of events and name any objects or substance that directly injured the employee or made the employee ill. For example: Worker stepped to the edge of the scaffolding to inspect work, lost balance and fell six feet to the floor. The worker's right wrist was broken in the fall.
DATE RETURN(ED) TO WORK:
Enter the date following the most recent disability period on which the employee returned to work.
ACORD 4 (2013/01) |
Page 5 of 5 |
Form Characteristics
| Fact Name | Description |
|---|---|
| Purpose | The Workers' Compensation Injury Report form serves to document information about work-related injuries or illnesses, facilitating claims processing. |
| Employer Details | Employers must provide their name and address, including ZIP code, as well as their employer identification number (FEIN) when filling out the form. |
| Legal Mandates | State-specific laws govern the reporting process. For instance, in California, it’s a felony to make false statements to obtain workers' compensation benefits. |
| Injury Specifics | The form requires details about the type of injury or illness, including the affected body parts and a description of how it occurred. |
| Notification Timeline | Employers are typically required to notify the appropriate parties about the injury, documenting the dates of notification and the day the employee was last worked. |
| Witness Information | The form allows for the inclusion of witness names and contact information, which can provide additional context and support for the claim. |
Guidelines on Utilizing Workers Compensation Injury Report
Completing the Workers Compensation Injury Report form accurately is crucial for ensuring claims are processed smoothly. Once the form is submitted, the appropriate parties will review it to determine the next steps in the claims process. This means it’s important to provide as much detail as possible to support the claim. Here are the steps to follow:
- Enter the employer’s name and address, including ZIP code, at the top of the form.
- Provide the carrier or administrator's name and address in the indicated fields.
- Input the claim number, report purpose code, jurisdiction, and jurisdiction log number as required.
- Fill out the employer's location address if it differs from the main address provided.
- Enter the industry code and the employer's FEIN (Federal Employer Identification Number).
- Add a contact phone number for the employer.
- Complete the carrier or claims administrator’s information, including policy period and self-insurance details where applicable.
- Provide the name of the employee (first, middle, last), their date of birth, social security number, and date hired.
- Fill in the employee's address, sex, marital status, occupation, employment status, and email address.
- Indicate the average weekly wage and the number of days worked per week.
- Specify if full pay was received for the day of injury and whether salary continued.
- Document the date and time of the injury or illness occurrence, last work date, and notification date to the employer.
- Provide details regarding the type of injury or illness, and the part of the body affected.
- Mention if the injury or illness occurred on the employer's premises and describe the department or location related to the incident.
- List all equipment, materials, or chemicals the employee was using during the incident.
- Describe the specific activity or work process the employee was engaged in when the injury occurred.
- Explain the sequence of events that led to the injury or illness, detailing how it transpired.
- Specify the date the employee returned to work if applicable.
- If the injury was fatal, include the date of death.
- Indicate whether safety equipment was provided and if it was used.
- Fill in the name and address of the physician or healthcare provider, along with any treatment information.
- Include witness names and contact details for further verification.
- Finally, ensure the form is signed by the employee and the preparer, entering their name, title, and phone number.
What You Should Know About This Form
What is the purpose of the Workers Compensation Injury Report Form?
The Workers Compensation Injury Report Form is designed to document any injuries or illnesses that occur in the workplace. This form serves several critical functions: it allows employers to collect and report necessary information to their insurance providers, ensures compliance with state laws, and provides a record that can be used for claims processing. Accurately completing this form helps speed the process of compensation for affected employees and ensures that all relevant details are captured for review.
What information is required on the form?
The form requires several pieces of information to be filled out accurately. Key details include the employer's name and address, employee information such as name, date of birth, and job title, along with specifics about the injury or illness, like the date and time it occurred. It’s important to include a description of how the injury happened, which aids in determining fault and coverage. Additionally, details regarding any medical treatment received, witness names, and the contact information for the claims administrator must also be provided. Make sure to avoid entering data in fields marked with an asterisk (*), as these are pre-defined criteria that should remain unchanged.
How should the form be submitted after completion?
What happens if the form is filled out incorrectly?
Common mistakes
When completing the Workers' Compensation Injury Report form, many people inadvertently make mistakes that can hinder the processing of their claims. Understanding these common errors can help you and others avoid pitfalls during this important task.
One frequent mistake is failing to provide complete information about the injury or illness. It’s essential to describe not just what happened, but also how it occurred. Be specific about the sequence of events, the objects involved, and the exact nature of the injury. A vague description can lead to confusion and delays in processing the claim.
Another error is overlooking the contact information. Often, the person filling out the form fails to include a reliable contact name and phone number. Including accurate contact information ensures that the claims administrator can quickly reach someone to gather any additional details needed for processing.
Additionally, people often neglect to report the employment status of the injured employee. This section helps determine eligibility for wage loss benefits. Failing to accurately indicate whether the employee was full-time, part-time, or in another work condition can lead to discrepancies and potential denial of benefits.
Many individuals also misinterpret the date of injury. It’s crucial to enter the correct date in the MM/DD/YY format, as errors here can complicate the claim process. A simple mistake in this area can result in unnecessary delays or even denials based on statute limitations.
Finally, a major pitfall involves the crucial section for medical treatment. Some report that no medical treatment was received when in reality, they’ve seen a healthcare provider. Be honest and thorough about all medical visits related to the injury, as failing to disclose this information can create significant issues with the claim.
By focusing on these areas and being meticulous when filling out the Workers' Compensation Injury Report form, employees can help ensure that their claims are processed efficiently and accurately.
Documents used along the form
When filing a workers' compensation claim, several documents are typically required in addition to the Workers' Compensation Injury Report form. Each of these forms plays a crucial role in the claims process and helps ensure that all necessary information is accurately recorded and submitted.
- Medical Report: This document provides detailed information about the employee's medical condition following the injury. It includes the diagnosis, treatment given, and the prognosis. This report is essential for assessing the severity of the injury and determining appropriate compensation.
- Witness Statements: Statements from co-workers or others who witnessed the incident can help clarify the circumstances surrounding the injury. Their accounts may provide valuable insight into how the accident occurred, which can be critical for the claims review process.
- Employer's Accident Investigation Report: Employers often conduct their own investigations after an incident. This report outlines their findings, including any unsafe conditions or violations of safety procedures that may have contributed to the injury. It serves as an additional layer of information for the claims evaluation.
- OSHA Report: If the injury was serious enough to require reporting under Occupational Safety and Health Administration (OSHA) regulations, an OSHA report may be necessary. This report details the safety violation and the employer's response to prevent future incidents.
Having these documents ready can facilitate a smoother claims process and assist in the quick resolution of any issues that may arise. By clearly documenting the injury, treatment, and context, employees and employers can strive for a fair assessment of the claim.
Similar forms
-
Accident Report Form: Similar to the Workers Compensation Injury Report, the Accident Report Form provides a detailed account of an incident that causes injury or damage. It includes information about the accident's time, place, and nature, ensuring that all pertinent details are documented for review.
-
First Aid Report: The First Aid Report captures details about any medical assistance provided immediately after an injury. Like the Workers Compensation Injury Report, it notes the specifics of the injury, the treatment given, and the individuals involved in the response to the situation.
-
Employee Incident Report: This document serves to record any workplace incidents, including those that may not result in injury. The Employee Incident Report is similar in its focus on the event details—time, location, and description—making it a vital tool for workplace safety analysis.
-
OSHA 300 Log: The OSHA 300 Log is specifically designed to record work-related injuries and illnesses for compliance with Occupational Safety and Health Administration regulations. It shares similarities with the Workers Compensation Injury Report as both documents track injury details, causation, and personnel involved, facilitating safety and claims processing.
Dos and Don'ts
When filling out the Workers' Compensation Injury Report form, it's critical to get it right. Accurate and complete information not only aids in processing your claim but also protects your rights. Here's a helpful list of dos and don'ts to consider:
- Do provide accurate names and addresses. Ensure you spell everything correctly.
- Don't omit any required fields marked with an asterisk. Missing information can delay your claim.
- Do include detailed descriptions of the incident. Provide a clear account of how the injury occurred.
- Don't downplay the severity of your injury. Describe symptoms truthfully and without embellishment.
- Do state the exact time and date of the incident. This information is crucial for your claim.
- Don't provide vague answers. Specifics enhance the credibility of your report.
- Do include names and contact information of witnesses. This can strengthen your claim.
- Don't sign the form until all sections are complete and accurate. Your signature certifies the truthfulness of the information.
- Do make a copy of the completed form for your records. Having documentation is essential for follow-up.
By following these guidelines, you ensure a smoother process for your workers' compensation claim. Remember, clarity and honesty are your best tools when it comes to reporting workplace injuries.
Misconceptions
Misunderstandings can often arise around the Workers Compensation Injury Report form. Here is a list of common misconceptions along with clarifications for each.
- The form is only for serious injuries. Many people believe this form is only for catastrophic events. However, it is also necessary for minor injuries or illnesses.
- Only the employee needs to fill out the form. Some think only the injured employee is responsible for completion. In reality, input from employers and supervisors is often required as well.
- Submitting the form guarantees a claim approval. While the form is essential for starting a claim, it does not automatically assure that the claim will be accepted.
- The form must be filled out immediately. A misconception exists that the report needs to be completed right after the injury. While timeliness is important, injuries can be reported within a specified timeframe based on state regulations.
- The information is only for insurance purposes. Individuals often think the details solely serve insurance entities. The data is also crucial for workplace safety assessments and potential improvements.
- Injury reports are confidential and never shared. Some might assume that the report remains entirely private. However, it can be shared with various parties, including your employer, insurance providers, and regulatory agencies.
- Submitting a report will affect future job chances. Fear exists that filing a report might harm future employment. Employers are generally prohibited from retaliating against employees for filing a legitimate workers' compensation claim.
- You cannot report an injury if it wasn't witnessed. It is believed that without witnesses, injuries cannot be reported. In fact, personal accounts and medical evidence can adequately support a claim.
- The form does not need to be detailed. Some feel brief descriptions suffice, but thorough, accurate details help build a stronger case and can expedite the claims process.
- All injuries must be caused at work to be reported. There is a notion that only injuries occurring on the job site can be reported. Injuries related to job duties, even off-site, may also qualify as compensable.
Key takeaways
1. Complete Every Section: Ensure all fields of the Workers Compensation Injury Report form are filled out, including those labeled with an asterisk (*). Leaving sections blank can delay the processing of your claim.
2. Accurate Dates Matter: Record all dates in the MM/DD/YY format. This clarity helps avoid confusion and errors during claim processing.
3. Specific Job Details Are Crucial: Include the exact job title and the industry code that describes the employer's business. This provides a clear context for the injury within the workplace.
4. Describe the Injury Clearly: When noting the type and part of the body affected by the injury, be precise. For example, refer to “lacerations to the right forearm” rather than using vague terms.
5. Include Witness Information: If there were witnesses present during the incident, include their names and contact details. This can support the validity of your claim.
6. Document Equipment and Chemicals Used: Specify all equipment, materials, or chemicals the employee was handling at the time of the accident. Even items not directly involved may provide crucial context.
7. Provide a Detailed Incident Narrative: Describe how the injury or illness occurred, including a sequence of events and any factors that contributed. This narrative is key to understanding the context of the incident.
8. Understand Your Employment Status: Correctly indicate whether the employee was full-time, part-time, or in a different employment status at the time of injury. This classification affects eligibility for benefits.
9. Review for Accuracy Before Submission: Take the time to review all entries for accuracy and completeness. Mistakes or omissions can impede timely processing of your workers' compensation claim.
Browse Other Templates
Are Kidney Transplant Patients Considered Disabled - Clear communication is vital when responding to the questions and sections within the form.
First Report of Injury Form - This form helps in documenting essential details related to an injury for proper compensation claims.